
Abstract
Background:
Return-to-sports (RTS) rates after anterior cruciate ligament (ACL) reconstruction (ACLR) differ according to the level at which patients return. It is unclear whether the level of RTS is affected by psychological readiness to return.
Purpose:
To examine the association between psychological readiness to RTS and subjective RTS level 12 months after ACLR.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
A total of 47 patients who underwent unilateral primary ACLR surgery were enrolled. Assessments at 6 and 12 months postoperatively consisted of knee strength testing (isokinetic quadriceps and hamstring strength), the International Knee Documentation Committee Subjective Knee Evaluation Form (IKDC-SKF), and the Anterior Cruciate Ligament-Return to Sport after Injury (ACL-RSI) scale to measure psychological readiness to RTS. Patients were assigned to 1 of 3 subgroups based on their subjective assessment of RTS level at 12 months postoperatively: RTS at or above preinjury level (RTS≥Pre; n = 19), RTS below preinjury level (RTS<Pre; n = 24), or no RTS (n = 4). Two-way mixed-model analysis of variance was used to examine the effects of RTS subgroup, postoperative time point, and group × time interaction with patient characteristics, knee strength, and IKDC-SKF and ACL-RSI scores. Multivariate logistic regression analysis was performed to determine which factors were associated with RTS subgroupings.
Results:
Significant differences were found among the RTS≥Pre, RTS<Pre, and no-RTS groups in age, ACL-RSI score at 6 and 12 months, quadriceps strength at 6 and 12 months, and IKDC-SKF score at 6 and 12 months (P < .001 for all). Multivariate logistic regression analysis revealed that RTS at or above preinjury level was associated with higher ACL-RSI score at 12 months postoperatively (odds ratio [OR], 1.11; 95% CI, 1.05-1.20; P = .003) and younger age (OR, 0.80; 95% CI, 0.61-0.92; P = .012).
Conclusion:
The ACL-RSI score was significantly different among the study groups, and the ACL-RSI score at 12 months postoperatively and younger age were associated with RTS at or above preinjury level.
Return to sports (RTS) is the goal of most patients undergoing anterior cruciate ligament (ACL) reconstruction (ACLR). 27 However, RTS rates after ACLR vary widely, ranging from 25% to 82%.8,10,13,18,23,24,30,31 In addition, approximately half of all athletes who undergo ACLR have a reduced RTS level compared with preinjury.5,7,22 The factors related to RTS after ACLR include younger age, male sex, higher patient-reported knee function, higher quadriceps strength, and higher hamstring strength.5,9,28,32 In addition, psychological readiness to RTS has recently received widespread attention as a factor related to RTS after ACLR. ‖ A systematic review of RTS after ACLR showed that psychological readiness was better in patients who were able to RTS than in those who did not. 33 However, the associations between psychological readiness and RTS levels are not fully understood.
One reason for the variation in RTS rates after ACLR may be due to the difference in the definitions of “RTS.” Some reports define RTS as returning at or above preinjury level,10,18,24,30 while others define RTS as returning to any sport.8,13,23,31 The International Federation of Sports Physical Therapy defines RTS according to 3 consecutive levels: return to participation, return to sport, and return to performance. 3 Return to participation means that the athletes play (any sport) at a lower level than their RTS goal. RTS means that the athletes return to the same sport as before injury but do not perform at their desired level (below preinjury level). Return to performance means that the athletes return to the same sport as before the injury and perform at or above their preinjury level. These different levels of return are important for a common understanding of RTS after ACLR.
Identifying the factors associated with different RTS levels would be informative for clinicians and athletes to achieve successful RTS after ACLR. The purpose of this study was to examine the association between patient characteristics, knee strength, knee function, and psychological readiness to RTS with the patient’s subjective assessment of RTS level at 12 months after ACLR. The hypothesis was that psychological readiness to RTS would be associated with subjective RTS level at 12 months after ACLR.
Methods
Participants
The protocol for this study received institutional review board approval, and all participants signed informed consent forms. We reviewed the records of patients who underwent unilateral primary ACLR surgery at an orthopaedic hospital between November 1, 2018, and November 30, 2021. Patients were excluded if they reported a history of lower extremity surgery other than ACLR, had a time interval between ACL injury and ACLR of more than 1 year, had a cartilage injury that required additional surgical procedures, or did not participate in a sport with a modified Tegner activity score of ≥6 before ACL injury. A total of 106 patients were eligible, and 47 patients with all available data were ultimately included in this study (Figure 1).

Flowchart of study enrollment. ACLR, anterior cruciate ligament reconstruction; ACL-RSI, anterior cruciate ligament-return to sport after injury; RTS, return to sport.
All included patients underwent double-bundle ACLR with hamstring tendon autografts and completed a standardized rehabilitation protocol in which they were allowed to start running at 12 weeks, participating in sports-specific drills without any restrictions at 6 months, and RTS at 9 months after ACLR. 17 Each patient performed exercise supervised by his or her physical therapist, focusing on improving range of motion, quadriceps function, and hip and trunk muscle strength up to 12 weeks, followed by more aggressive strength training and gradually retraining neuromuscular control in sport activities. If symptoms such as pain, obvious claudication, or severe muscle weakness remained, running or sports-specific drills were delayed by the physical therapist and/or physician.
Postoperative Assessment
Assessments at 6 and 12 months postoperatively consisted of knee strength testing (isokinetic quadriceps and hamstring strength), the International Knee Documentation Committee Subjective Knee Evaluation Form (IKDC-SKF), and the Anterior Cruciate Ligament-Return to Sport after Injury (ACL-RSI) scale to measure psychological readiness to RTS. 29 In addition, the modified Tegner activity score was confirmed preoperatively and at 12 months.
Knee Strength Testing
Isokinetic quadriceps and hamstring strength was assessed using a dynamometer (Biodex System 3; Biodex Medical Systems) 6 and 12 months after ACLR. The concentric strength was measured at a velocity of 60 deg/s. The participants performed 5 repetitions with maximal effort after some practice trials. The limb symmetry index (LSI) of the peak torque, calculated as the percentage of the value in the involved limb to that in the uninvolved limb, was used.
International Knee Documentation Committee Subjective Knee Evaluation Form
The IKDC-SKF ranges from 0 to 100, and this assessment scores for knee symptoms, function, and sports activities. 16 The Japanese version of the IKDC-SKF, which was used in the current study, has been determined to have high validity and reliability. 15
ACL-RSI Scale
The ACL-RSI scale consists of 12 items and includes 3 domains: emotions, confidence in performance, and risk appraisal. The score can range from 0 to 100, with higher scores indicating greater psychological readiness. The Japanese version of the ACL-RSI scale, which has shown high validity and reliability, was used in the current study. 14
Assessment of Subjective RTS Level
The RTS level was based on previous studies and assessed 12 months postoperatively.2,10,18,19,24,26,30 Patients were asked to select their current RTS level from among the following 4 options: (1) return to the same sports as before the injury, at or above the preinjury level; (2) return to the same sports as before injury, but without the desired level; (3) return to any sports but not to the same sports (or desired sports); or (4) no RTS. 3 Those patients who did not return at their preinjury level were asked to indicate their reason(s): (1) fear of reinjury; (2) knee functional limitations; (3) social reasons (eg, changed school or work, busy at work, moved); and/or (4) other (patients were provided space to include details). Patients who did not return due to social reasons were excluded from this study.
In the present study, there were no patients who reported their current RTS status as “return to any sports”; thus, the patients were classified into the 3 remaining subgroups: RTS at or above preinjury level (RTS≥Pre), RTS below preinjury level (RTS<Pre), or no RTS.
Statistical Analysis
The Shapiro-Wilk test was used to confirm the normality of continuous variables. Two-way mixed model analysis of variance was used to examine the effects of group (RTS≥Pre, RTS<Pre, no RTS), time (6 and 12 months postoperatively), and group × time interaction on ACL-RSI score, IKDC-SKF score, quadriceps strength LSI, and hamstring strength LSI. The 1-way analysis of variance or chi-square test was used to examine the difference in age and sex among the subgroups. Post hoc comparisons were conducted using Tukey test, with the Cohen d calculated as the effect size of the post hoc comparisons. 12 A Cohen d value >0.80 was interpreted as large, 0.50 to 0.79 as moderate, and 0.20 to 0.49 as small. 12
Univariate logistic regression analysis was used to examine the association between independent variables and RTS levels. The independent variables were age, sex (0, male; 1, female), ACL-RSI at 6 and 12 months, quadriceps and hamstring strength LSI at 6 and 12 months, and IKDC-SKF at 6 and 12 months. Factors with P < .10 in the univariate logistic regression analysis were used as candidate variables in a subsequent multivariate logistic regression analysis. The selection criterion of the variables for the multiple logistic regression analysis was backward stepwise based on the minimum Akaike information criteria. The statistical significance level for all tests was set at P < .05. Statistical analyses were performed using JMP Pro Version 16 (SAS Institute).
Results
Of the 47 participants, 19 were assigned to the RTS≥Pre group, 24 to the RTS<Pre group, and 4 to the no-RTS group. The time from surgery to measurement was 184.1 ± 12.9 days (range, 148-225 days) for 6 months and 369.9 ± 16.9 days (range, 340-463 days) for 12 months. The RTS≥Pre group was significantly younger than the RTS<Pre and no-RTS groups (vs RTS<Pre, P = .007, d = 1.03; vs no RTS, P < .001, d = 4.47), and the RTS<Pre group was significantly younger than the no-RTS group (P = .004, d = 1.55). There was no significant difference in sex between the groups.
A significant group effect and time effect on ACL-RSI was found, while there was no significant interaction effect of group × time (Table 1). The RTS≥Pre group showed significantly higher ACL-RSI score than the other groups at 6 months (vs RTS<Pre, P = .001, d = 1.17; vs no RTS, P < .001, d = 3.88) (Figure 2A) and at 12 months (vs RTS<Pre, P < .001, d = 1.39; vs no RTS, P < .001, d = 3.70; Figure 2B). Furthermore, the RTS<Pre group showed significantly higher ACL-RSI than the no-RTS group at 6 months (P < .001, d = 2.39) and at 12 months (P = .002, d = 1.76).
Participant Characteristics by Study Group a
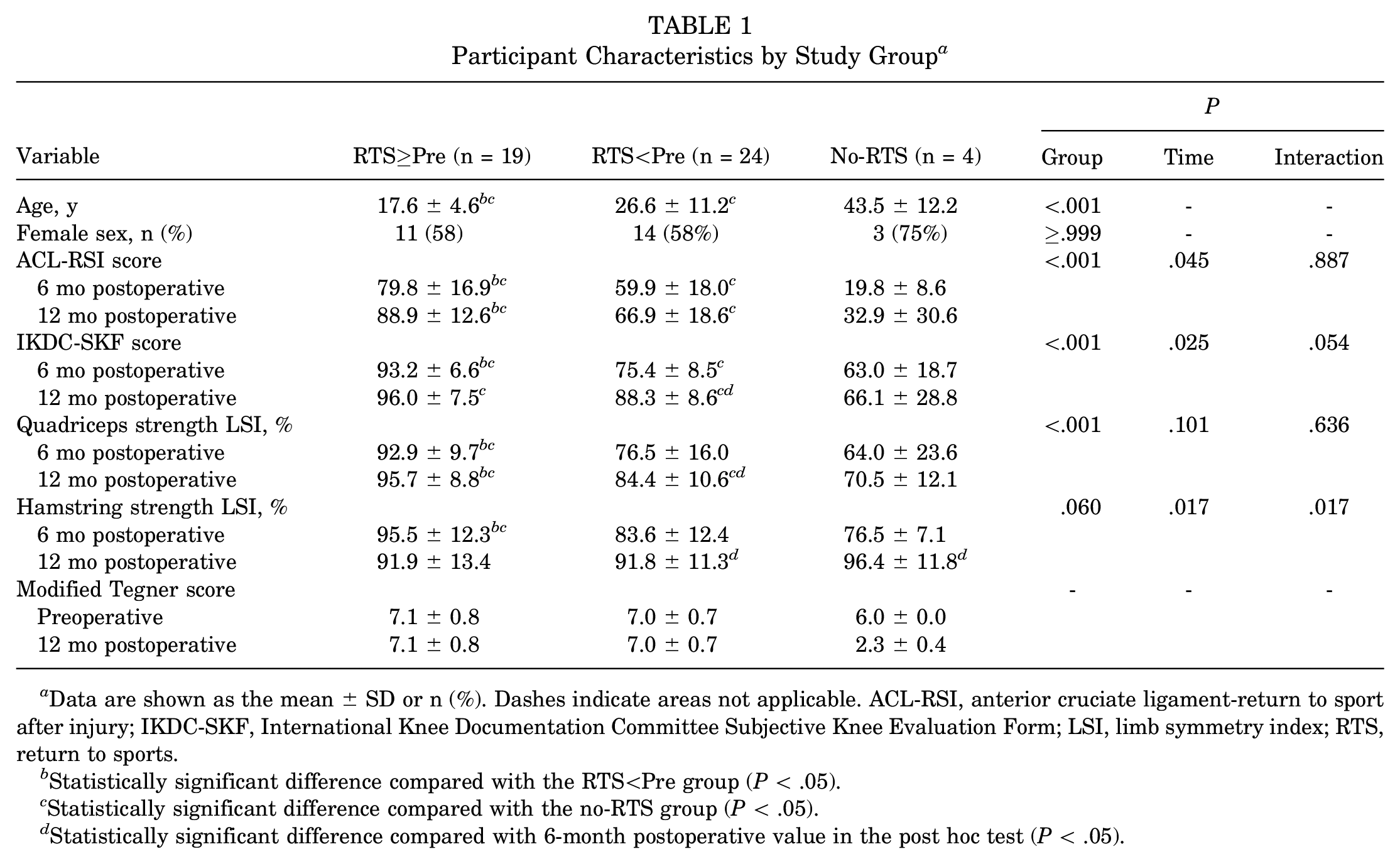
Data are shown as the mean ± SD or n (%). Dashes indicate areas not applicable. ACL-RSI, anterior cruciate ligament-return to sport after injury; IKDC-SKF, International Knee Documentation Committee Subjective Knee Evaluation Form; LSI, limb symmetry index; RTS, return to sports.
Statistically significant difference compared with the RTS<Pre group (P < .05).
Statistically significant difference compared with the no-RTS group (P < .05).
Statistically significant difference compared with 6-month postoperative value in the post hoc test (P < .05).
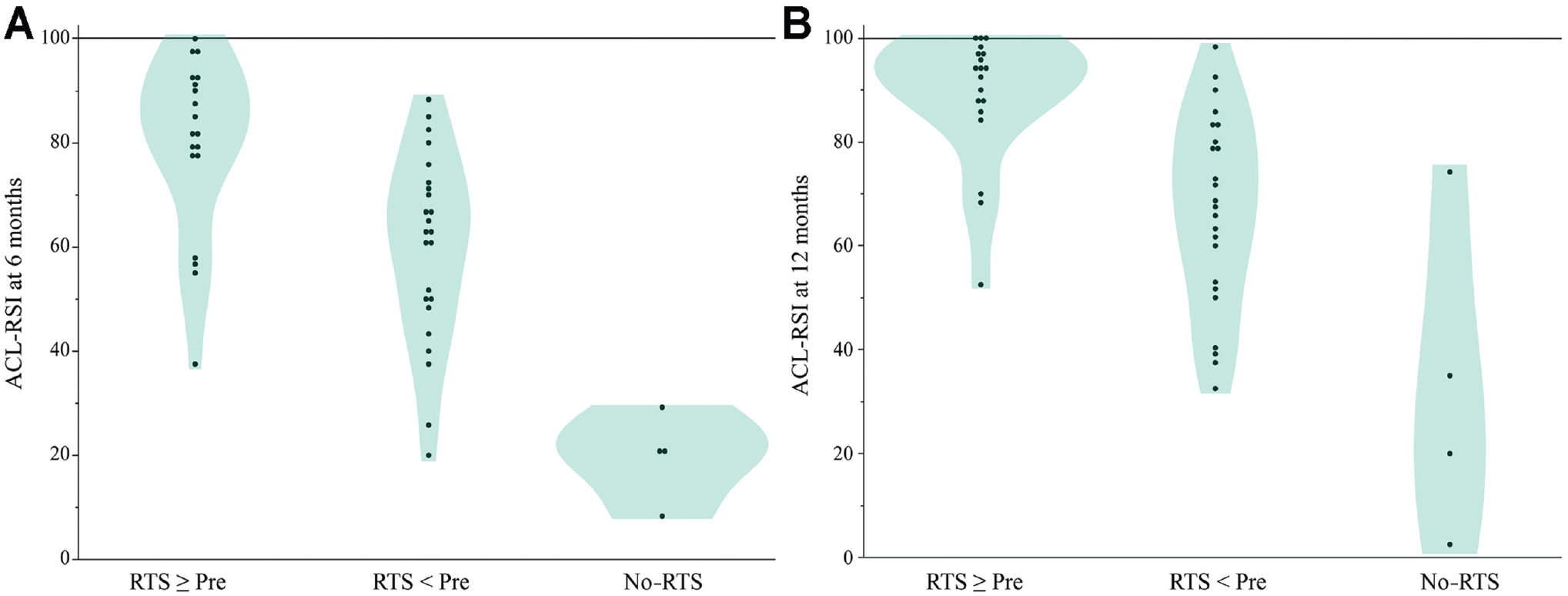
Comparison of the ACL-RSI between study groups at (A) 6 months and (B) 12 months postoperatively. RTS, return to sports; ACL-RSI, Anterior Cruciate Ligament-Return to Sport after Injury.
A significant group effect was also found for IKDC-SKF and quadriceps strength LSI, while a significant group × time interaction was found only for hamstring strength LSI. The RTS≥Pre group showed significantly higher IKDC-SKF scores than the other groups at 6 months (vs RTS<Pre, P < .001, d = 2.36; vs no RTS, P < .001, d = 3.54) and at 12 months (vs no RTS, P < .001, d = 2.58). Furthermore, the RTS<Pre group showed significantly higher IKDC-SKF scores than the no-RTS group at 6 months (P = .036, d = 1.29) and at 12 months (P = .001, d = 1.91). The RTS≥Pre group showed significantly higher quadriceps strength LSI than the other groups at 6 months (vs RTS<Pre, P = .002, d = 1.24; vs no-RTS, P = .002, d = 2.47) and at 12 months (vs RTS<Pre, P = .002, d = 1.18; vs no-RTS, P < .001, d = 2.84). Furthermore, the RTS<Pre group showed a significantly higher quadriceps strength LSI than the no-RTS group at 12 months (P = .040, d = 1.34). The RTS≥Pre group showed a significantly higher hamstring strength LSI than the other groups at 6 months (vs RTS<Pre, P = .007, d = 0.98; vs no-RTS, P = .018, d = 1.67).
Tables 2 and 3 show the results of the univariate and multivariate logistic regression analyses for independent variables determining subjective RTS levels at 6 and 12 months postoperatively. Univariate regression analysis of the 6-month variables revealed that younger age, higher ACL-RSI, higher quadriceps strength LSI, higher hamstring strength LSI, and higher IKDC-SKF were significantly associated with RTS at or above preinjury compared with RTS below preinjury. For 12-month variables, younger age, higher ACL-RSI, higher quadriceps strength LSI, and higher IKDC-SKF were significantly associated with RTS at or above preinjury compared with RTS below preinjury. Stepwise multivariate analysis of the 6-month variables revealed that IKDC-SKF (P = .004) and quadriceps strength LSI (P = .037) remained significant predictors of RTS at or above preinjury, and stepwise multivariate analysis of the 12-month variables revealed that ACL-RSI (P = .003) and age (P = .012) remained significant explanatory variables of RTS at or above preinjury.
Logistic Regression Analysis Using Variables at 6 and 12 Months After ACLR to Examine Factors Determining RTS at or Above Preinjury Versus Below Preinjury a

B indicates the partial regression coefficient. Dashes indicate areas not applicable. ACL-RSI, anterior cruciate ligament-return to sport after injury; CI, confidence interval; IKDC-SKF, International Knee Documentation Committee Subjective Knee Evaluation Form; LSI, limb symmetry index; OR, odds ratio; RTS, return to sports.
Logistic Regression Analysis Using Variables at 6 and 12 Months After ACLR to Examine Factors Determining RTS Below Preinjury Versus no RTS a

B indicates the partial regression coefficient. ACLR, anterior cruciate ligament reconstruction; ACL-RSI, anterior cruciate ligament-return to sport after injury; CI, confidence interval; IKDC-SKF, The International Knee Documentation Committee Subjective Knee Evaluation Form; LSI, limb symmetry index; OR, odds ratio; RTS, return to sports.
In the comparison of RTS below preinjury and no RTS, the univariate logistic regression analysis using variables at 6 months after ACLR revealed that younger age was significantly associated with RTS below preinjury (Table 3). For variables at 12 months, younger age, higher ACL-RSI and higher quadriceps strength LSI were significantly associated with RTS below preinjury. Stepwise multivariate analysis of variables 6 months revealed that only ACL-RSI remained a predictor of RTS below preinjury, but the coefficient did not reach statistical significance (P = .079). For variables at 12 months, stepwise multivariate analysis revealed that ACL-RSI score (P = .054) and age (P = .062) remained significant explanatory variables of RTS below preinjury, but the coefficients of these variables were not statistically significant.
Discussion
The most important findings of the present study were that ACL-RSI scores at 6 and 12 months were significantly associated with both RTS at or above preinjury and RTS below preinjury. These findings indicate that psychological readiness is related to level of RTS after ACLR.
Previous studies have reported that the ACL-RSI was significantly better in patients with RTS at or above preinjury than in those with other RTS levels, including no RTS.10,18,30 Other studies showed that ACL-RSI was significantly worse in patients with no RTS than in those with RTS at any level.2,13,26 However, it was unclear whether ACL-RSI differed between patients in the RTS≥Pre, RTS<Pre, and no-RTS groups. The present study revealed that the ACL-RSI at 6 and 12 months was significantly different among the subgroups based on the subjective RTS level 12 months after ACLR. The RTS≥Pre group had significantly higher ACL-RSI scores than the other groups 6 and 12 months after ACLR. The univariate regression analysis revealed that ACL-RSI at 6 months was a significant predictive variable for RTS at or above preinjury, and ACL-RSI at 12 months was a significant explanatory variable for both RTS at or above preinjury and RTS below preinjury. Furthermore, multivariate regression analysis revealed that RTS at or above preinjury was associated with ACL-RSI at 12 months and age. These findings indicate that the ACL-RSI is associated with subjective RTS levels after ACLR.
Significant group differences were also found in age, with patients in the RTS≥Pre group being youngest (17.6 ± 4.6 years), followed by the RTS<Pre group (26.6 ± 11.2 years) and no-RTS group (43.5 ± 12.2 years). Quadriceps strength LSI was significantly higher in the RTS≥Pre versus RTS<Pre group at 6 and 12 months and the RTS<Pre versus no-RTS group at 12 months. Although age and quadriceps strength have been reported to affect RTS after ACLR,5,9 there are no reports on the differences in these factors by subjective RTS level. When comparing patients who did and did not RTS, some studies have shown younger age and higher quadriceps strength LSI in patients who returned than those who did not return, while other studies have shown no differences.5,6,18,20,31 In previous studies,6,18,20,31 RTS was defined as “return to the same sports as before injury at or above the preinjury level,” and all other patients were included in the group of those who did not RTS. These differing definitions of RTS may help explain the difference in findings between the previous studies and the present study. A new finding of the current study was that age and quadriceps strength LSI at 6 and 12 months were different according to subjective RTS level.
There was no significant difference in sex among RTS levels. Hamstring strength LSI was significantly higher in patients in the RTS≥Pre group compared with the RTS<Pre and no-RTS groups at 6 months, but there were no significant group differences at 12 months. A previous study comparing patients who returned to sports with those who did not return found no significant differences in sex or hamstring strength LSI between the groups, 18 which is consistent with the results of the present study. Hamstring strength LSI 12 months after ACLR with hamstring tendon autograft has been reported as being above 90%, 17 and the hamstring strength LSI at 12 months in the present study was above 90% in all groups. These results indicate that hamstring strength may be restored 12 months postoperatively with rehabilitation, even when the hamstring is used for grafting. Thus, the effect of hamstring strength on RTS level would be smaller than that of quadriceps strength because hamstring strength recovery was good after ACLR.
Age, quadriceps strength, and IKDC-SKF score have been reported to affect ACL-RSI, suggesting that ACL-RSI is influenced by the patient’s physical condition.13,21,31 Factors such as age, quadriceps strength, and IKDC-SKF have also been reported to affect RTS after ACLR, and these factors could also affect the RTS levels.5,9,28 However, even when age was included as a variable, we found that ACL-RSI was a significant factor determining RTS level at 12 months. Furthermore, there was a significant group difference in ACL-RSI at 6 months, and in univariate analysis, ACL-RSI at 6 months predicted RTS at or above preinjury level at 12 months. This indicates that psychological readiness was different among the 3 study groups even before RTS, and suggests that psychological readiness may be important. IKDC-SKF and quadriceps strength also differed among the 3 study groups and, since IKDC-SKF and quadriceps strength remained in the multivariate analysis, they may be more important as predictors before RTS. However, since ACL-RSI was the most associated factor for determining level of RTS at 12 months, psychological follow-up after RTS may be important. The present findings provide further support for the importance of evaluating ACL-RSI. The cause-and-effect relationship between psychological readiness and RTS level is unclear because the present study was retrospective in nature. Further studies are needed to investigate whether interventions that improve psychological readiness will improve subjective RTS levels after ACLR.
In the present study, the ACI-RSI differed between the RTS groups, but why psychological readiness was low is not fully understood. Although previous studies have reported that quadriceps strength and IKDC-SKF were associated with ACL-RSI,21,25,31 it is known that some patients with good recovery of knee function may have difficulty returning to sport or have low ACL-RSI.1,7 It should also be kept in mind that the ACL-RSI is an assessment measure that may be influenced by the personality of each patient. In addition, it is not yet clear how to improve ACL-RSI. Further research is needed on the causes of low psychological readiness and how to improve it.
Limitations
There are some limitations to this study. First, it was a single-center study. Second, the number of patients in the no-RTS group was small (n = 4). However, the percentage of patients in the no-RTS group was 10%, which was comparable with that of a previous study. 26 Third, the follow-up rate was low. Since this study was retrospective by design, there was a possibility of selection bias in the results. Fourth, the validity and reliability of the subjective RTS level was not assessed. Finally, the causal relationship between subjective RTS level and psychological readiness could not be determined due to the retrospective study design.
Conclusion
In the present study, the ACL-RSI score was significantly different according to subjective RTS level, and the ACL-RSI score at 12 months postoperatively as well as lower younger age were associated with RTS at or above preinjury level.
Footnotes
Acknowledgements
The authors thank all of the study participants.
Final revision submitted March 30, 2023; accepted May 3, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: T.I. and M.S. have been involved in a joint research project with Nitto Denko. M.S. has also been involved in a joint research project with Nitoms Corp. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Hokkaido University (approval number: 22-49).