
Abstract
Background:
Significant variation exists in the published rates of return to sport after anterior cruciate ligament (ACL) reconstruction (ACLR). Functional outcomes and psychological response to injury have been implicated as factors that influence return to sport. Most studies focus on patients aged in the mid-20s, and less is known about this topic in adolescents.
Purpose:
To report midterm ACLR results for adolescent patients with regard to return to primary sport, patient-reported outcomes, and reinjury rate.
Study Design:
Case-control study; Level of evidence, 3.
Methods:
Adolescent athletes were contacted at a minimum of 2 years after ACLR. Patients completed 2 patient-reported outcome measures, the ACL--Return to Sport After Injury (ACL-RSI) and the International Knee Documentation Committee (IKDC) subjective form, and responded to questions regarding preinjury primary sport and level of competition, post-ACLR return to primary sport status, and reinjury.
Results:
A total of 74 patients (mean ± SD surgical age, 15.9 ± 1.5 years; follow-up age, 19.9 ± 2.0 years; response rate, 24.5%) completed the surveys at a mean of 4.0 ± 2.0 years after primary ACLR. Outcome scores averaged 90.3 ± 12.3 for IKDC and 81.6 ± 20.4 for ACL-RSI. Questionnaire responses indicated that 27.0% of patients did not return to or sustain primary sport participation after ACLR; the principal reasons were poor knee function, team/training change, and fear of another injury. Both IKDC and ACL-RSI scores were statistically lower in patients who did not successfully return to their primary sport in contrast to patients who successfully resumed their primary sport (IKDC, P = .026; ACL-RSI, P < .001). IKDC and ACL-RSI scores were moderately positively correlated with one another (r Spearman = 0.60). There were 18 patients (reinjury rate, 24.3%) who suffered another ACL injury; 8 of these injuries included ipsilateral ACL graft tear (retear rate, 10.8%).
Conclusion:
In our cohort, 73% of adolescent patients successfully returned to their primary preinjury sport at a minimum of 2 years after ACLR. Both knee function and psychological responses to injury were important in determining an adolescent athlete’s return to sport. The findings support the use of the IKDC and ACL-RSI at midterm follow-up, with higher scores associated with a greater likelihood of adolescent patients returning to sport after ACLR.
The anterior cruciate ligament (ACL) plays a vital role in providing translational and rotatory stability to the knee. 22 More than 200,000 ACL injuries occur in the United States annually, 17 with the highest incidence seen in athletes aged 15-25 years who participate in pivoting sports. 9 Most athletes undergo ACL reconstruction (ACLR) in order to regain knee function, with the goal of returning to sport participation 23 at the same or higher level of competition.
Despite surgical intervention, many patients do not return to their primary sport. Return-to-sport rates vary widely; studies have reported that 55% to 97% of patients participate in their primary sport after ACLR. 1,8,17,19 Patient characteristics, such as age at time of injury and sex, have been identified as factors that can contribute to the ability to return to sport. Additionally, functional and psychological factors obtained from patient-reported outcomes have been identified to influence return to sports. These functional deficits include knee pain, 15,17 effusion, 15,17 instability, 15,17 and decreased strength. 17 Psychological barriers to return to sports include fear of reinjury and kinesiophobia. 13,15 However, the mean age of patients in each of these studies ranged from 22 to 28 years, and limited evidence exists on return to sport in adolescent athletes. One study 24 focusing only on return to sport in adolescents found that those who met clinical strength and International Knee Documentation Committee (IKDC) cutoff for return to sport were more likely to sustain their sport participation for 1 year after returning to play from ACLR, but the study did not include any comparison with adolescents who failed to return to sport or the psychological factors contributing to return to sport.
Patient-reported outcomes are gold standard clinical tools to evaluate knee function and psychological response to sport participation. Several series with patient-reported functional outcomes, as assessed by the IKDC questionnaire, indicated that 86% of patients (mean age in mid-20s) reported to have normal or nearly normal knee function at 2 years after ACLR. 3,6 –8,15,18,28 Patient-reported psychological outcomes, as evaluated via the ACL--Return to Sport After Injury (ACL-RSI) Scale, have indicated that patients (mean age, 27-30 years) with a more positive psychological response to sport are more likely to have returned to competitive sports at 6 and 12 months after ACLR. 14,16,21 These studies focus on patients who are, on average, in their mid- to late-20s and provide insufficient evidence for a younger, adolescent population.
Adolescents differ significantly from young adults for numerous reasons. Adolescents have much more access to organized sports through school and community leagues, and thus the intensity and commitment to sports are different from most young adults who are not collegiate- or professional-level athletes. Further, skeletally immature or recently skeletally mature patients may have different functional outcomes from ACLR, which may or may not be because of underlying neuromuscular control issues. Finally, the psychological response to injury and the ability to cope with the associated challenges may be different in adolescents versus adults. Together, these differences highlight the necessity to study adolescents as a separate cohort from young adults.
The purpose of this study was to evaluate return to sport, patient-reported outcomes, and reinjury rate for adolescent athletes at a minimum of 2 years after ACLR. Results from this study may allow orthopaedic surgeons to more accurately counsel adolescent athletes on midterm functional outcomes and return to same-level sport.
Methods
Study Population
The study cohort included adolescent athletes treated at a single outpatient pediatric sports medicine clinic by 2 fellowship-trained, board-certified orthopaedic surgeons. After institutional review board approval, a chart review was conducted on patients who underwent ACLR between December 2006 and December 2016. Inclusion criteria included patients who were 18 years of age or younger at the time of ACLR and were more than 2 years out from ACLR surgery. Patients were excluded from the study if they were nonathletes, underwent revision ACLR, or were non-English speaking. Patients undergoing multiligamentous knee reconstruction were also excluded. Patients who met the inclusion criteria for this study were contacted via telephone and asked to complete a series of surveys. After providing informed consent, patients were given the option to complete the surveys by telephone or email.
A chart review yielded 314 patients that met inclusion criteria between December 2006 and December 2016. Of these patients, 77 were successfully contacted and agreed to participate in the study, indicating a response rate of 24.5% (Figure 1). Three patients were excluded because they did not consider themselves athletes before their ACLR. The final study population included 74 patients with a mean ± SD follow-up of 4.0 ± 2.0 years (range, 2.0-12.1 years) after ACLR.
Study Measures
Patient-reported outcomes were evaluated using the IKDC Subjective Knee Form and the ACL-RSI questionnaires. In addition, participants were asked to complete a return-to-sport questionnaire with their preinjury primary sport and level of competition (middle school recreational, middle school competitive, high school recreational, or high school competitive), ability to return to their primary sport post-ACLR (yes or no), ability to return to preinjury level of competition after ACLR (same level, higher level, lower level), and any subsequent ACL injuries. Patient who did not return to their primary sport after ACLR were asked follow-up questions regarding the reason for not returning, with the following possible responses: “poor knee function,” “I do not trust my knee,” “fear of getting a new injury,” “team or training has changed,” “moving on to college/work,” and “other reasons.”
The IKDC Subjective Knee Form, 10 intended to assess the total overall knee function, includes information on symptoms/pain, function, and sports/physical activity. A higher score indicates a higher level of knee function and a lower degree of symptoms. This form is considered valid for all patients 10 years and older, whether the patients complete the form alone or with the assistance of their parent or guardian. The ACL-RSI questionnaire 26 is a validated 12-question scale to evaluate patients’ confidence in their knee and fears associated with return to sport after ACLR. Scores range from 0 to 100, with a higher score indicating an increased psychological desire to return to sport.
Patients were grouped based on their return to primary sport response: those who returned to and sustained participation in their primary sport after ACLR (group 1) and those who did not return to their primary sport after ACLR (group 2). Patients who initially returned to sport for a limited period of time but who had a subsequent injury that prevented sustained sport participation were considered to have not successfully returned to sport and were included in group 2. Patients who returned to sports after ACLR but completed their sport career before follow-up were considered to have successfully returned to sport and were included in group 1.
Statistical Analysis
Descriptive statistics were generated for characteristic data for both the initial study population (299 patients) and the final study cohort (74 patients). Characteristic data were compared between the study population and the study cohort as well as between groups 1 and 2 within the study cohort. Age at surgery was normally distributed and was compared using independent-samples t tests (α = .05). Time to follow-up, age at follow-up, and body mass index (BMI) were not normally distributed and were compared using Mann-Whitney U tests. Categorical characteristic data were compared using a chi-square test or Fisher exact test. Within the study cohort, neither ACL-RSI nor IKDC scores were normally distributed in group 1; as such, Mann-Whitney U tests were used to compare these scores between the 2 groups. Power analysis was performed for sample size estimation based on preliminary data collected for this study, which compared ACL-RSI scores at minimum 2-year follow-up between patients who returned and those who did not return to sport. The difference in group means was 25, with a mean SD of 21. With α = .05 and power = 0.8, the projected sample size needed was approximately N = 22 (11 patients in each group).
Spearman rank correlation was performed to describe the linear relationship between IKDC and ACL-RSI in the study cohort. Logistic regression was performed on the following independent variables to determine any additional influence on return to sport: BMI, sex, age at surgery, laterality, preinjury level of competition, primary sport, time between injury and surgery, type of insurance, graft type, presence or absence of meniscal tear, and type of meniscal surgery performed. Calculations and statistical analysis were performed using Microsoft Excel (Microsoft 2010) and SAS software Version 9.4 (SAS Institute).
Results
Characteristic data on the 299 patients in the study population and the 74 patients ultimately included in the study cohort (Figure 1) are reported in Table 1. Female athletes represented 62.2% of the study cohort.

Flowchart of patient cohort selection. ACLR, anterior cruciate ligament reconstruction.
Patient Characteristics a
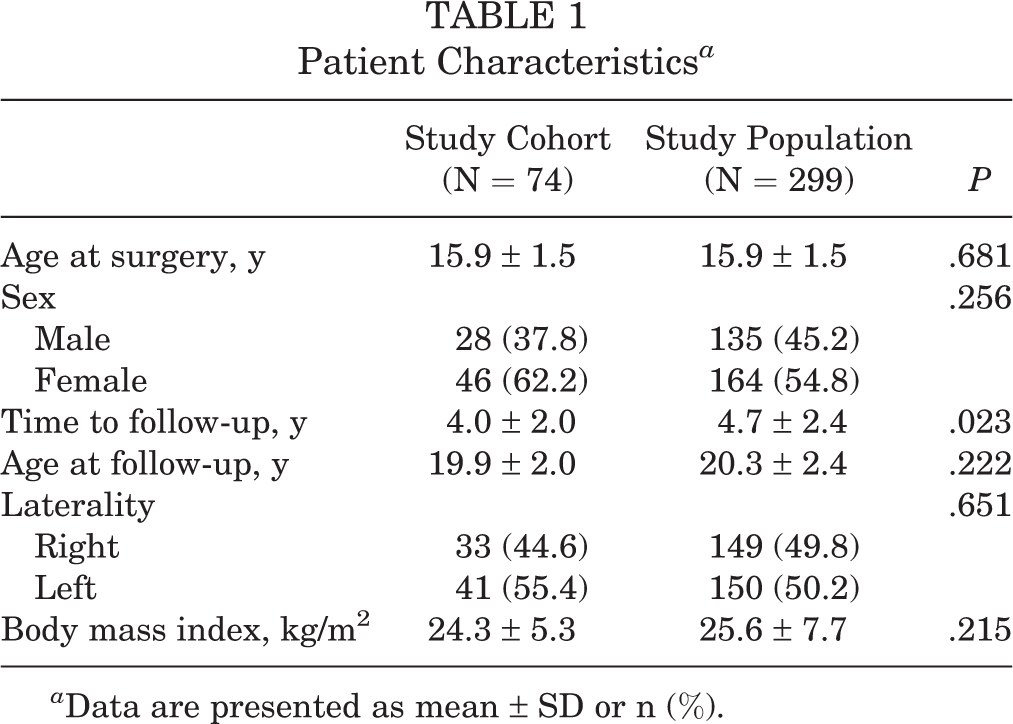
a Data are presented as mean ± SD or n (%).
The study cohort included 54 patients in group 1 (73.0%) and 20 patients in group 2 (27.0%). Within group 1, the majority of patients (90.7%) reported returning to the same level (29 patients) or a higher level (20 patients) of competition. There were 4 patients who reported returning to a lower level of competition and 1 patient who was unsure. In group 2, there were 3 patients who indicated that they had initially returned to their primary sport but underwent a subsequent knee injury; among them, 2 had second ACL tears, which led them to stop participation. Table 2 summarizes patient-reported reasons for not returning to sport. Table 3 summarizes the patient characteristics of each group. No significant differences were found between groups on any of the included characteristics.
Reasons for Not Returning to Primary Sport

Characteristics of Study Groups a
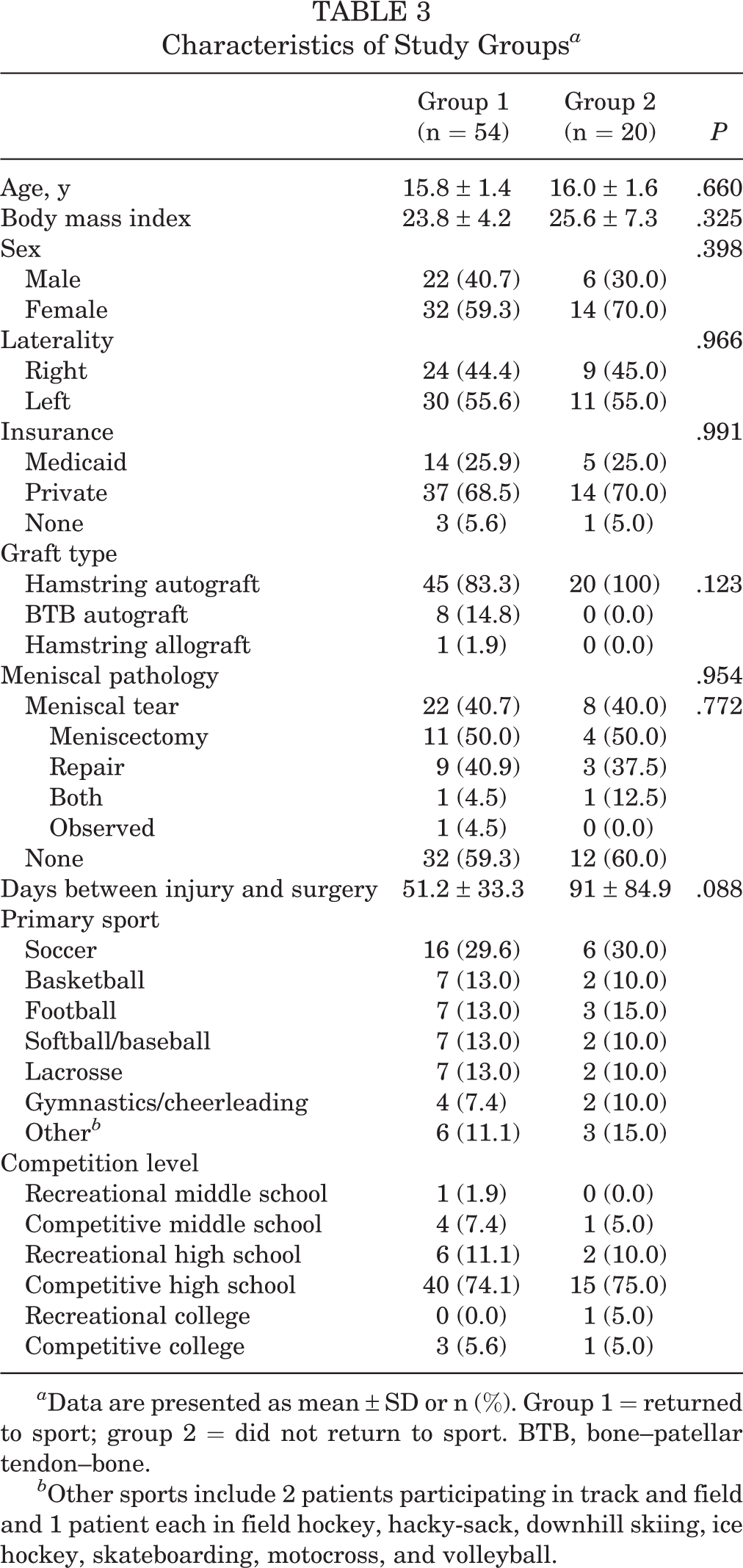
a Data are presented as mean ± SD or n (%). Group 1 = returned to sport; group 2 = did not return to sport. BTB, bone--patellar tendon--bone.
b Other sports include 2 patients participating in track and field and 1 patient each in field hockey, hacky-sack, downhill skiing, ice hockey, skateboarding, motocross, and volleyball.
There was a statistically significant difference in IKDC and ACL-RSI scores between groups, with group 1 patients reporting higher scores on both the IKDC and ACL-RSI relative to patients in group 2 (Table 4). Spearman rank correlation indicated a significant positive correlation between IKDC score and ACL-RSI score (r Spearman = 0.60; P < .001). Logistic regression identified that time between injury and surgery had a significant association with the ability to return to sports (P = .0442; 95% CI, 0.975-1.000; odds ratio, 0.987). This signifies that a delay of surgery by 1 day reduces the odds of return to sport by 1.3%. No other variables analyzed reached statistical significance.
Difference in PROs Between Patients Who Returned Versus Those Who Did Not Return to Sport After ACLR a

a Data are presented as mean ± SD. Group 1 = returned to sport; group 2 = did not return to sport. ACL-RSI, ACL-return to sport after injury; ACLR, anterior cruciate ligament reconstruction; IKDC, International Knee Documentation Committee; PRO, patient-reported outcome.
A total of 18 patients (13 female, 5 male) reported a second ACL tear, for an overall reinjury rate of 24.3% of the study population. Of these, 5 patients tore their ipsilateral ACL, 10 patients tore their contralateral ACL, and 3 patients tore both their ipsilateral and contralateral ACLs. A total of 16 of these patients received hamstring autograft and 2 had bone--patellar tendon--bone (BTB) autograft. Additionally, 7 of these patients had concurrent meniscal pathology, of which 4 had meniscectomy, 2 were repaired, and 1 was observed. Of the 18 patients who sustained a subsequent ACL injury, 13 (72%) reported returning to their primary sport and were thus included in group 1. Of the 5 patients who did not return to sport, 3 patients never returned to their primary sport and 2 patients returned to sport after their first but not their second ACL injury. These 5 patients were all included in group 2. No difference was found regarding IKDC and ACL-RSI scores in patients with a subsequent ACL injury (P = .160 and P = .150, respectively) relative to adolescents without a subsequent injury, but there was not sufficient power to exclude failure of finding this effect given the low number of reinjuries in the study cohort.
Discussion
Overall, this study established a midterm return to sustained sport participation rate of 73% and a reinjury rate of 24.3% for adolescent athletes at a minimum of 2 years after ACLR. These findings provide focused results on the high-risk adolescent population to help orthopaedic surgeons more accurately counsel these athletes on their expected outcomes after ACLR. Further, this study suggests that those who do return to sport have higher ACL-RSI and IKDC scores, indicating that an adolescent’s return to sport participation is associated with both knee function and knee confidence.
Previously reported return-to-sport rates have varied widely among studies, in large part because of variation in the characteristics and the definition of return to sport across the literature. 1,8,17,19 In this study, we found the rate of sustained return to primary sport participation to be 73% for adolescent patients, suggesting that the majority of young patients are able to achieve their presurgery goal to return to sport. These findings are comparable with the 56%-97% return rates for highly competitive young athletes 11,12,19,27 and are higher than the 55%-65% reported by recreational adult athletes (mean age, 22-28 years). 1,8,17 Of the 27% unable to maintain sport participation after ACLR, 3 patients (4.1% of the study cohort) were able to return to their primary sport initially but did not sustain sport participation secondary to a subsequent knee injury. Despite this, the overall sustained return-to-sport rate among patients with a subsequent ACL injury was 72%, which is comparable with the overall rate of 73% for the whole cohort.
Of the 20 patients in our study who were unable to return and maintain their primary sport through the end of their sport career, 30% reported changes in their life circumstances (changes in training or starting work/college), 25% reported psychological reasons (fear of reinjury or lack of trust in knee), and 25% reported poor knee function. A recent systematic review 12 on pediatric and adolescent athletes’ return to sport after ACLR also identified the life transition period from adolescence to young adulthood as a possible bias in return rates. In our cohort, this held true for 30% of patients who did not return back to their primary sport. These patients experienced a change in priorities, became ineligible to play on their team owing to time away during postsurgical rehabilitation, or were unable to continue their sports at the collegiate level after high school. This aligns with the trend of decreased sport participation with age, as it has been reported that 45% of sport participants will stop athletics during childhood or adolescence. 5 The second major barrier to return to sports was psychological reasons, present among 25% of our cohort. Recent studies 4,13,15,27 have increasingly identified that some of these psychological reasons include fear of reinjury and the psychological stress of undergoing rehabilitation. 4 The third major reason for failing to return to sports was poor knee function, accounting for 25% of the patients. Of the 5 patients citing poor knee function, 3 had concurrent meniscal pathology, 2 of which had meniscectomy and 1 had a repair. This aligns with multiple studies 11,15,17,21 that have shown lower knee function among groups that fail to return to sport.
The IKDC scores reported in this study are in agreement with those previously reported in the literature. A study inclusive only of adolescents who returned to sport participation reported a mean IKDC score of 87.5 at the time of return to sport. 24 Another study 17 reported mean IKDC scores of 93.8 for adult patients (mean age, 22.4 years) who returned to sport and 78.0 for those who did not return to sport at 2-year follow-up. These results suggest that adolescent athletes have self-reported functional knee outcomes similar to adults after ACLR.
ACL-RSI scores presented in this adolescent cohort are in line with prior literature focused on young adults. A previous study 14 reporting ACL-RSI scores between those who returned and those who did not return to sport (mean patient age, 27.5 years) did not find a significant difference at 3 months postoperatively but did find significant a difference at 1-year follow-up (71.05 ± 16.25 vs 58.61 ± 18.34; P = .001). We found a similar difference in ACL-RSI scores at 2-year follow-up (81.6 for group 1 and 52.7 for group 2; P < .001) in adolescent athletes, and this suggests that the likelihood of adolescent patients returning to sport after ACLR is strongly associated with their trust in their knee. Further, the Spearman rank correlation showed a moderately strong positive correlation between ACL-RSI and IKDC. Those who scored highly on the IKDC were likely to score highly on the ACL-RSI, and vice versa. This suggests that knee function and psychological readiness to return to sport after ACLR were related in this adolescent cohort.
ACL reinjury is a feared consequence of ACLR. Previously reported rates of secondary ACL injury to either the ipsilateral or the contralateral knee in adolescent athletes (mean age, 16-17 years) have ranged from 20% to 35%, with a greater incidence of contralateral ACL injury. 20,25 Factors implicated with an increased rate of reinjury include age <19 years, female sex, and greater self-reported confidence. 20 Furthermore, adolescents younger than 18 years are more likely to have a secondary ACL injury relative to 18- and 19-year-olds. 25 The reinjury rate of 24.3% observed in this study population aligns with the rates reported by previous studies 20,25 on adolescent athletes. Most of these patients (16 patients; 89%) had a hamstring autograft, while the remainder (2 patients) had a BTB autograft. Despite experiencing a subsequent ACL injury, there was no difference found on ACL-RSI or IKDC scores in the reinjury cohort relative to those without a reinjury.
One limitation of this study is the response rate of 24.5%, as some selection bias may exist between patients who chose to participate in the study and those who did not. However, given that there were no significant between-group differences in patient characteristics, with the exception of follow-up time, we think this bias did not affect our results. Another limitation of this study is that the retrospective study design increased the chance of recall bias and limited our analysis. Last, we were only able to find that time between injury and surgery had a significant association with the ability to return to sport on regression analysis. It is possible that this analysis was underpowered to show other significant associations.
This study suggests that both knee function and psychological response to injury are important in determining an adolescent athlete’s return to previous sport participation. These 2 factors were related to one another such that those who scored higher on the IKDC were likely to score higher on the ACL-RSI and vice versa. These findings highlight the importance of both the functional and psychological recovery after ACLR in adolescent athletes’ return to sport. This is consistent with the current literature. 1,2,13,17,21 Applying this to clinical practice can increase the support not only for strong physical therapy interventions after ACLR but also for psychological support to help patients increase their confidence in their knee. Further studies are necessary to see if interventions focused on increasing psychological confidence in knee function can improve return-to-sport rates among adolescent athletes. Additional studies are also necessary to evaluate the influence of ACL reinjury on return-to-sport participation.
Footnotes
Final revision submitted May 12, 2020; accepted June 8, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.L.P. has received educational support from Arthrex; consulting fees from Arthrex, Ceterix, Grand Rounds, and Smith & Nephew; and nonconsulting fees from Arthrex. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Connecticut Children’s Medical Center (study No. 14-109).