
Abstract
Background:
Biomarkers collected in synovial tissue and fluid have been identified as potential predictors of outcomes after arthroscopy.
Purpose:
To provide a narrative review of the current literature that assesses the associations between preoperative biomarkers in the synovial fluid or synovial tissue and patient outcomes after knee arthroscopy.
Study Design:
Narrative review.
Methods:
We searched the PubMed database with keywords, “biomarkers AND arthroscopy,” “biomarkers AND anterior cruciate ligament reconstruction,” and “biomarkers AND meniscectomy.” To be included, studies must have collected synovial fluid or synovial tissue from patients before or during arthroscopic knee surgery and analyzed the relationship of biomarkers to postoperative patient outcomes. Biomarkers were classified into 4 main categories: metabolism of aggrecan in cartilage, metabolism of collagen in cartilage (type II collagen), noncollagenous proteins in the knee, and other. When biomarker levels and outcomes were expressed with continuous variables, we abstracted the Pearson or Spearman correlation coefficients as the effect measure. If the biomarker values were continuous and the outcomes binary, we abstracted the mean or median biomarker values in those with favorable versus unfavorable outcomes. We calculated effect sizes as the difference between means of both groups divided by the standard deviation from the mean in the group with better outcomes.
Results:
Eight studies were included in the review. Each study reported different patient outcomes. Biomarkers associated with metabolism of aggrecan, type II collagen metabolism, and noncollagenous proteins as well as inflammatory biomarkers had statistically significant associations with a range of patient outcomes after knee arthroscopy. Difference across studies in sample size and outcome measures precluded choosing a single biomarker that best predicted patient outcomes.
Conclusion:
The findings suggest that biomarkers associated with metabolism of aggrecan, type II collagen metabolism, noncollagenous proteins, as well as inflammatory biomarkers may help surgeons and their patients anticipate surgical outcomes.
Knee arthroscopy, a minimally invasive surgical procedure, allows surgeons to treat a wide range of knee conditions including injuries to the meniscus, anterior cruciate ligament (ACL), and other structures. Arthroscopy is performed frequently, with approximately 200,000 arthroscopic ACL reconstructions (ACLRs) and more than 400,000 arthroscopic partial meniscectomies (APMs) performed annually in the United States. 17,37
Although most patients have improvements in pain and function for up to 10 years after ACLR, outcomes are variable 11 and patients with ACLR are at risk of developing posttraumatic osteoarthritis. 34,36 APM procedures typically show improvement in pain and functional outcomes within the first 12 months after surgery 15,21 ; however, outcomes are variable after APM, and the literature concerning factors that affect these outcomes is inconsistent. 16,22,38 Patients who undergo APM are also at risk for progression of radiographic knee osteoarthritis (OA). 7,21,32
Since knee arthroscopy is a common procedure, a diagnostic tool to predict poor short- and longer-term outcomes of these procedures on the basis of preoperative findings would advance care. Several studies have found demographic and imaging factors associated with outcome including age, sex, smoking history, preoperative health status, body mass index, and presence of chondral lesions. 6,7,13,21,24 However, these studies only explain about 20% of the variability in outcome. 6 In an effort to explain more of the variability in outcome and provide a better prediction for patients and surgeons, investigators have evaluated the effects on surgical outcome of biomarkers in synovial fluid, synovial tissue, serum, and urine. Synovial fluid biomarkers have been studied in patients with knee OA to detect early joint degradation and serve as a potential target for pharmaceutical therapies. 10,25 Serum and urine biomarkers were analyzed to determine their effectiveness for predicting knee OA progression in the Phase I Foundation for the National Institutes of Health case control study, but only N-telopeptide of type I collagen in urine predicted progression. 2 Osteoarthritis Research Society International published recommendations for soluble biomarker assessments in knee OA clinical trials in 2015, encouraging investigators to determine if specific biomarkers are useful for detecting earlier stages of knee OA. 18
In addition to predicting degenerative changes of the knee, biomarkers present a potential opportunity for predicting a patient’s pain and function after knee arthroscopy. We are not aware of published summaries of the role of synovial fluid and tissue biomarkers as predictors for knee arthroscopy outcomes. We aimed to provide a narrative review that identifies synovial fluid and synovial tissue biomarkers collected at baseline that can predict outcomes after multiple types of arthroscopic knee procedures. The research question guiding this review was: what is the current evidence surrounding the association of synovial fluid and synovial tissue biomarkers obtained before arthroscopic knee surgery and the outcomes of surgery, including pain, function, structure, or need for additional surgery?
Methods
Study Selection
To address our research question, we reviewed the PubMed database for studies between 1990 and 2021, with 3 separate searches in the following order: “biomarkers AND arthroscopy,” “biomarkers AND anterior cruciate ligament reconstruction,” and “biomarkers AND meniscectomy.” To be eligible, a study must have included patients who underwent arthroscopic knee surgery with collection of synovial fluid or synovial tissue before or during the procedure. The study needed to analyze the relationship of biomarkers obtained before or during knee arthroscopy to postoperative patient outcomes, including pain, function, cartilage damage, and the need for further surgeries. The inclusion and exclusion criteria are summarized in Table 1. We also reviewed the reference lists of all included studies for additional studies that may not have been in the original searches.
Study Inclusion and Exclusion Criteria

Biomarkers Assessed
We organized the biomarkers in knee OA according to the 4 categories used by Lotz et al 23 : biomarkers associated with the metabolism of aggrecan in cartilage, those associated with the metabolism of collagen in cartilage (type II collagen), those related to noncollagenous proteins that play a role in metabolic pathways in the knee joint, and those associated with other processes, specifically inflammation. We included all biomarkers reported in each study in this review.
Statistical Analysis
The specification of biomarker values and outcomes varied across studies. If both were expressed with continuous variables, we abstracted the Pearson or Spearman correlation coefficients as the effect measure. If the biomarker values were continuous and the outcomes binary, we abstracted the mean or median biomarker values in those with favorable and unfavorable outcomes. We defined the effect size as the difference between the means of both groups divided by the standard deviation of the group with better outcomes. In studies that reported Cohen d effect sizes, we still calculated a separate effect size to compare the same effect measure across all studies. In studies that reported median (rather than mean) values of the biomarker, we were unable to calculate a comparable effect size and simply present the median values (with interquartile ranges where available) in the comparison groups. Excel (Microsoft Corporation) was used for statistical analysis.
Results
Search Results
The initial search (“biomarkers AND arthroscopy”) yielded 211 results, which were narrowed down to 34 after abstract screening. After full-text review, 5 studies were found to meet eligibility criteria. We completed the same protocols for the second (“biomarkers AND anterior cruciate ligament reconstruction”) and third searches (“biomarkers AND meniscectomy”). The second search yielded an additional 101 studies, and 3 studies met the eligibility criteria. However, we excluded 1 study 1 from further analysis because we were unable to abstract correlations derived from the entire cohort. The third search yielded 39 studies, none of which met eligibility criteria. One additional study was included in our analysis after a review of reference listings. Figure 1 shows the winnowing of the 351 initial studies to the 8 final studies. 8,9,12,19,26,27,30,33

Flowchart of search methodology and manuscript inclusion and exclusion. The number of exclusions exceeds the number of studies excluded because some studies were excluded for multiple reasons. Three studies met two exclusion criteria after records were screened by abstract (Takahasi et al 35 , No arthroscopy performed AND Other; Bresnihan et al 5 , Nonclinical study AND Rheumatoid arthritis; Salvador et al 29 , Rheumatoid arthritis AND Psoriatic arthritis).
Outcomes and Biomarkers Assessed
Outcomes and biomarkers assessed for the 8 included studies are summarized in Table 2. Biomarker source was synovial fluid for all studies except for Sobue et al, 33 who used synovial tissue. Of note, 2 studies 26,27 reported follow-up surgery as a method of distinguishing favorable from unfavorable outcomes. Sobue et al 33 assessed progression in cartilage damage by comparing the number of high-grade lesions (assessed arthroscopically on 6 articular surfaces with the Outerbridge scoring system 28,39 at the initial ACLR) and at 2-year follow-up (reassessed arthroscopically during routine surgery for tibial staple removal). Patients in the progression group had an increased number of high-grade (grades 3 and 4) cartilage lesions during the second arthroscopy; patients without an increase in high-grade cartilage lesions in the second arthroscopy were in the nonprogression group. 33 Tables 3 to 5 present the data for all biomarkers that had a statistically significant association with improvement in patient outcomes within the corresponding categories of biomarkers.
Summary of Patient Outcomes and All Biomarkers Tested in Each Study a

a Biomarker source was synovial fluid for all studies except for Sobue et al, who used synovial tissue. ACLR, anterior cruciate ligament reconstruction; APM, arthroscopic partial meniscectomy; C2C, collagenase-generated cleavage neoepitope of type II collagen; C4S, chondroitin-4-sulfate; C6S, chondroitin-6-sulfate; CCL, C-C chemokine ligand; CCR, C-C chemokine receptor; COMP, cartilage oligomeric matrix protein; CTX-II, C-terminal crosslinked telopeptide of type II collagen; FGF-2, fibroblast growth factor 2; HGF, hepatocyte growth factor; IFNγ, interferon γ; IKDC, International Knee Documentation Committee; IL, interleukin; IL-1Ra, interleukin 1 receptor antagonist; KEM, internal knee extension; KFA, knee flexion angle; KOOS-PS, Knee injury and Osteoarthritis Outcomes Score–Physical Function; KOOS-QOL, Knee injury and Osteoarthritis Outcomes Score–Quality of Life; KS, keratan sulfate; MCP-1, monocyte chemotactic protein 1; MIP, macrophage inflammatory protein; MMP, matrix metalloproteinase; NR, not reported; NTX-1, N-terminal crosslinking telopeptide of type I collagen; PASS, Patient Acceptable Symptom State; PDGF-BB, platelet-derived growth factor BB; RANTES, regulated upon activation, normal T cell expressed and secreted; sGAG, sulfated glycosaminoglycan; TIMP, tissue inhibitor of metalloproteinase; TNF-α, tumor necrosis factor α; TSG-6, tumor necrosis factor-stimulated gene 6 protein; U, units/mL; VAS, visual analog scale; VEGF, vascular endothelial growth factor; vGRF, vertical ground-reaction force.
b When biomarker units of measurement differed from other measurements in the same study, the measurement was provided in parentheses.
c Cuellar et al 8 included 10 patients who underwent ACL reconstruction, 35 patients who underwent arthroscopic partial meniscectomy, 20 patients who underwent arthroscopy for a combination of injured ACL and meniscus, and 5 patients who underwent knee arthroscopy for cartilage lesions.
Correlation Between Biomarkers and Patient Outcomes a

a ACLR, anterior cruciate ligament reconstruction; APM, arthroscopic partial meniscectomy; CCL, C-C chemokine ligand; CCR, C-C chemokine receptor; IL, interleukin; MMP, matrix metalloproteinase; PDGF-BB, platelet-derived growth factor BB; RANTES, regulated upon activation normal T cell expressed and secreted; TIMP, tissue inhibitor of metalloproteinase; VAS, visual analog scale.
b Spearman correlation coefficients were used in Scanzello et al30 and Gupta et al,12 Pearson correlation coefficients were used in Cuellar et al.8
c Cuellar et al 8 included 10 patients who underwent ACLR, 35 patients who underwent arthroscopic partial meniscectomy, 20 patients who underwent arthroscopy for a combination of injured ACL and meniscus, and 5 patients who underwent knee arthroscopy for cartilage lesions.
d TIMP-3 was only significant in patients who underwent ACLR, but not in patients with meniscal injuries only.
Mean Values Reported for Biomarkers Associated With Improved Patient Outcomes a

a ACLR, anterior cruciate ligament reconstruction; APM, arthroscopic partial meniscectomy; HGF, hepatocyte growth factor; IKDC, International Knee Documentation Committee; IL-α, interleukin-1 α; IL-1Ra, interleukin-1 receptor antagonist; KS, keratan sulfate; KOOS-QOL, Knee injury and Osteoarthritis Outcomes Score–Quality of Life; MMP, matrix metalloproteinase; PASS, Patient Acceptable Symptom State (KOOS-QOL threshold, 62.5 points; IKDC threshold, 75.9 points).
b Effect sizes were calculated by dividing the difference between means of both groups by the standard deviation from the mean in the group with better outcomes.
c Nakajima et al 27 included patients who underwent synovectomy, debridement, and excision of degenerative meniscal tears, fragments of articular cartilage, or chondral flaps and osteophytes
Median Values Reported for Biomarkers Associated With Improved Patient Outcomes a
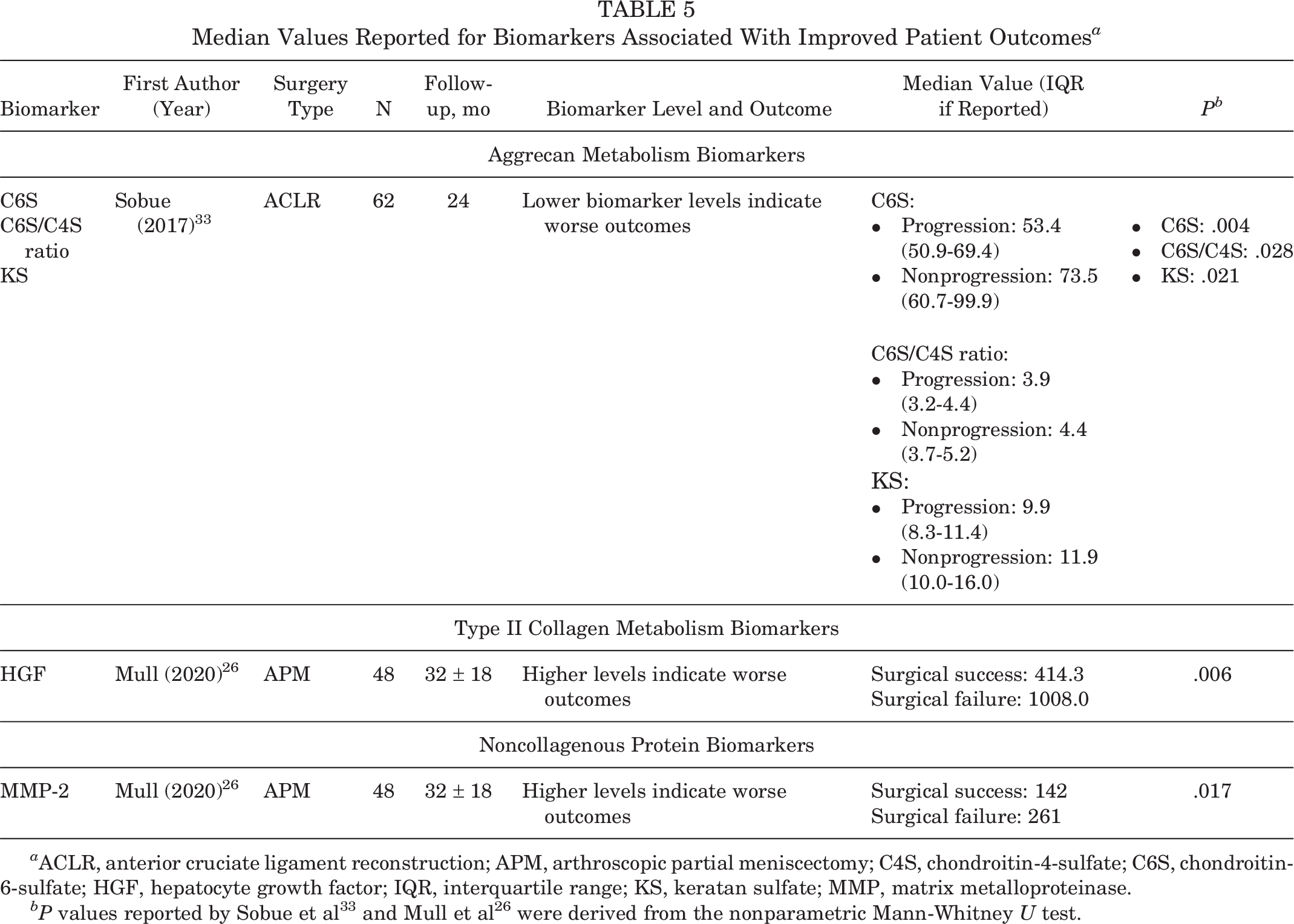
a ACLR, anterior cruciate ligament reconstruction; APM, arthroscopic partial meniscectomy; C4S, chondroitin-4-sulfate; C6S, chondroitin-6-sulfate; HGF, hepatocyte growth factor; IQR, interquartile range; KS, keratan sulfate; MMP, matrix metalloproteinase.
Reporting Associations between Biomarkers and Outcomes
Three studies 8,12,30 reported correlations between preoperative synovial biomarkers and postoperative patient outcomes. All correlation values are presented in Table 3. Three studies 19,26,27 compared the mean preoperative levels of synovial fluid biomarkers between patients with favorable postoperative patient outcomes and with unfavorable outcomes. Since the studies used a variety of effect measures (eg, correlation, difference in means, difference in medians), we indicate those with statistically significant associations with outcome. Two studies reported median biomarker levels associated with postoperative outcomes. 26,33
Associations Between Biomarkers and Outcomes in APM
Higher preoperative levels of C-C chemokine receptor 7 (CCR7) and C-C chemokine ligand 19 (CCL19), both inflammatory markers, had strong correlations with greater changes in Lysholm score (score improvement) at 16 weeks (CCR7, 0.70; CCL19, 0.71) and 24 months (CCR7, 0.79; CCL19, 0.85) after arthroscopy. 30 Mull et al 26 classified patients who underwent a second knee surgery as having unfavorable postoperative outcomes and those who did not have a second surgery as having favorable outcomes. Mull et al 26 showed that those with favorable outcomes had lower preoperative levels of hepatocyte growth factor (HGF) 26 (type II collagen metabolism biomarker) and matrix metalloproteinase-2 (MMP-2) 26 (noncollagenous protein biomarker), with effect sizes of 1.3 and 0.81, respectively (Table 4). In addition to reporting mean values, Mull et al 26 also reported that the median HGF in the surgical failure group was 2.4 times higher at baseline than in the surgical success group (P = .006), and the median MMP-2 was 1.8 times higher in the surgical failure group (P = .017).
Associations Between Biomarkers and Outcomes in ACLR
Higher baseline levels of interleukin (IL)-6 (inflammatory marker) had moderate correlations with higher visual analog scale (VAS) pain scores, indicating worse pain, at all follow-up timepoints (r = 0.364-0.536) (Table 3). 12 Higher IL-6 levels were also associated with greater knee laxity 2, 6, and 12 months post-ACLR (r = 0.513, 0.626, and 0.740, respectively), with lower functional Lysholm scores (worse function) at 2, 6, and 12 months post-ACLR (r = –0.317, –0.714, and −0.436, respectively) and with lower Tegner activity levels (less activity) at 12 months post-ACLR (r = −0.570). 12 Lattermann et al 19 found that higher baseline levels of IL-1α (inflammatory biomarker), IL-1 receptor antagonist (IL-1ra; inflammatory biomarker), and MMP-9 (noncollagenous protein biomarker) were all statistically significantly associated with Knee injury and Osteoarthritis Outcomes Score--Quality of Life subscale below the Patient Acceptable Symptom State (PASS) threshold (worse outcome) with effect sizes of 3.30 (P = .004), 0.09 (P = .03), and 2.33 (P = .01), respectively. Higher baseline levels of IL-1α were also statistically significantly associated with International Knee Documentation Committee scores that fell below the PASS threshold (worse outcome) with an effect size of 0.38 (P = .02). 19 Sobue et al 33 reported that median preoperative levels of keratan sulfate (KS), chondroitin-6-sulfate (C6S), and the C6S/ chondroitin-4-sulfate (C4S) ratio were higher in subjects with a smaller number of high-grade cartilage lesions between baseline and implant removal at follow-up (Table 5). 33 Evans-Pickett et al 9 analyzed the association between high and low baseline concentrations of IL-6 (inflammatory biomarker) and MMP-3 (noncollagenous biomarker) and gait biomechanics and found that high synovial fluid concentrations of these markers were associated with aberrant gait biomechanics at 6 months after ACLR.
Associations Between Biomarkers and Outcomes in Multiple Knee Arthroscopies
Two inflammatory biomarkers had weak to moderate correlations with VAS scores 1 year after surgery, with lower biomarker levels associated with less pain: platelet-derived growth factor BB (PDGF-BB; r = −0.29) and regulated upon activation, normal T cell expressed and secreted (RANTES; r = −0.28). 8 Similar to Mull and colleagues, 26 Nakajima et al 27 classified patients who underwent a second knee surgery as having unfavorable postoperative outcomes and those who did not have a second surgery as having favorable outcomes. Nakajima et al 27 showed that the association between the change in KS levels (an aggrecan metabolism biomarker) between baseline and 12 weeks after surgery and improved patient outcomes (patients that did not require total knee replacement [TKR] 2 years after the initial surgery) had an effect size of 1.33.
Discussion
Our principal finding in this review was that in patients undergoing APM, inflammatory (CCR7 and CCL19), 30 type II collagen metabolism (HGF), 26 and noncollagenous protein biomarkers (MMP-2) 26 were significantly associated with patient outcomes after surgery. In patients undergoing ACLR, inflammatory (IL-6, IL-1α, and IL-1ra), 12,19 noncollagenous protein (MMP-9 and tissue inhibitor of metalloproteinase [TIMP]-3), 8,19 metabolism of aggrecan biomarkers (C6S, C6S/C4S, and KS) 33 were all significantly associated with patient outcomes after surgery. In patients undergoing multiple types of knee arthroscopies, inflammatory (PDGF-BB and RANTES) 8 and noncollagenous protein biomarkers (MMP-3: TIMP-2) 8 were associated with patient outcomes after knee arthroscopy.
At baseline, higher levels of biomarkers associated with cartilage metabolism breakdown and inflammation (CCR7 and CCL19) 30 and lower expression levels of markers associated with noncollagenous proteins, type II collagen metabolism, and inflammation (PDGF-BB and RANTES) 8 were associated with improved patient outcomes. These results offer useful information for clinicians identifying which biomarkers could potentially predict patient outcomes after arthroscopy.
Knee arthroscopy patients are at a higher risk for development and progression of knee OA after surgery. 7,21,32,34,36 Boffa et al reported cluster of differentiation (CD)14, CD163, C-terminal telopeptide (CTX)I, CTXII, IL-6, procollagen type II carboxy-terminal propeptide (PIICP) tumor necrosis factor (TNF)-α, and tumor necrosis factor-stimulated gene 6 protein (TSG)-6 as promising biomarkers associated with prognosis of knee OA (according to the BIPED classification) in patients that did not undergo arthroscopy in their systematic review including 201 synovial fluid biomarkers. 3 CD14 and CD163 were both positively associated with osteophyte progression and CTXI and CTXII were associated with rapid clinical progression. 4 Increased levels of IL-6 and TNF-α after APM and TSG-6 and PIICP in nonsurgical OA patients were associated with radiographic progression. 4 Our analysis also focused on prognostic biomarkers for predicting functional outcomes after knee arthroscopy. Although we evaluated all these prognostic biomarkers suggested by Boffa et al, 4 we identified only IL-6 9,12 and MMP-3 8,9 as significantly associated with postoperative outcomes after knee arthroscopy. 4 This may be because patients undergoing knee arthroscopy are relatively earlier in their disease process than the OA patients captured by the review by Boffa et al. 4 Although the patients in the review by Boffa et al 4 did not undergo surgery, these prognostic biomarkers reviewed might provide helpful insight for predicting OA progression after arthroscopy.
Two conflicting findings were presented in this review that were most likely due to small sample sizes in the following studies (Table 2). Although Sobue et al 33 reported that lower baseline C6S biomarker levels were significantly associated with more cartilage damage progression on arthroscopic diagnosis; Nakajima et al 27 reported that baseline C6S levels were not significantly associated with the patient’s likelihood of receiving a TKR 2 years after initial knee arthroscopy. Chondroitin sulfate is a major component of the extracellular matrix of many connective tissues including cartilage and is responsible for resistance and elasticity in cartilage. 14 Since knee OA is characterized by the breakdown of cartilage, as well as structural and metabolic changes to the joint tissues including subchondral bone and synovial tissue, we hypothesize that higher levels of C6S might reflect a less-advanced knee OA joint. The results of Sobue et al reflect this hypothesis because patients with less initial C6S had worse cartilage damage after arthroscopy. 33 The lack of a statistically significant correlation between C6S levels and outcomes in Nakajima et al 27 reflect the study’s small sample size and the inclusion in their cohort of patients that underwent multiple types of knee arthroscopic surgery. In contrast to Nakajima et al, 27 patients in Sobue et al 33 only underwent ACLR and the association between C6S and outcomes might be specific to ACLR. Further, the outcomes assessed in both these studies are not the same, which could also account for the different association. Sobue et al 33 assessed cartilage damage and Nakajima et al 27 assessed the need for TKR after arthroscopy. Both studies did report that KS was significantly associated with their respective patient outcomes measured. 27,33 In addition, Scanzello et al 30 reported higher baseline expression levels of inflammatory biomarkers (CCR7 and CCL19) were associated with improved patient outcomes, while Cuellar et al 8 reported lower baseline expression levels of inflammatory biomarkers (PDGF-BB and RANTES) were associated with improved patient outcomes.
Limitations
We acknowledge limitations to this review. Sample sizes of the studies we reviewed were small and outcomes and follow-up intervals varied. Further, each study reviewed different types of knee arthroscopic procedures. In addition, we recognize that the reconstructive setting during ACLR and degenerative setting during APM are different environments and might affect the types of biomarkers found in the synovial tissue or fluid. Our data render it difficult to extract a biomarker category or even specific marker found in the synovial fluid or tissue that is only present in either the reconstructive or degenerative setting.
However, to the best of the authors’ knowledge, this is the first summary that relates preoperative levels of synovial tissue and fluid biomarkers with postoperative outcomes after knee arthroscopy. By applying the biomarker classification categories from Lotz et al, 23 we were able to categorize potential biomarkers that are involved with knee arthroscopy postoperative outcomes, even though a single biomarker did not show significance across all studies.
Conclusion
The findings of this review suggest that biomarkers associated with metabolism of aggrecan, type II collagen metabolism, noncollagenous proteins, as well as inflammatory biomarkers may help surgeons and their patients anticipate surgical outcomes. Further research is needed to improve the understanding of synovial fluid biomarkers for predicting patient outcomes after surgery, specifically how these biomarkers are associated with cartilage anabolism, metabolism, and inflammatory pathways in the knee joint. In addition, future research should focus on the difference in types of biomarkers present in the reconstructive and degenerative arthroscopic setting. This knowledge will allow clinicians to investigate potential treatments targeting these molecular processes to improve postoperative outcomes. Since there are few studies analyzing preoperative synovial fluid and tissue biomarkers for postoperative outcomes after arthroscopy, conclusions from individual studies are provisional. A high-quality study that analyzes a larger cohort of patients undergoing knee arthroscopy for synovial cartilage and inflammatory biomarkers would provide useful information for understanding which markers predict outcomes.
Footnotes
Final revision submitted April 10, 2023; accepted May 3, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.N.K. has received honoraria from Pfizer. M.H.J. has received research support from Flexion Therapeutics (now Pacira) and consulting fees from Regeneron Pharmaceuticals and Samumed (now Biosplice). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.