
Abstract
Pigmented villonodular synovitis (PVNS) is an uncommon entity involving articular or extra-articular tissues and maybe localized or diffuse in extent. The knee is by far the commonest joint to get involved. Localized PVNS of the knee can occur in any location but its confinement to the posterior compartment is infrequent. We present our experience of managing localized posterior compartment PVNS of the knee. There were 10 patients (7 males and 3 females) with average age of 33 years. These patients had symptoms of pain, locking, or swelling for a mean of 13.9 years before diagnosis. All the patients underwent arthroscopic synovectomy without adjuvant therapy, and PVNS was proven on histopathology. At an average follow-up of 23 months, no patient had recurrence of symptoms. The average International Knee Documentation Committee (IKDC) score at last follow-up was 85.21. Magnetic resonance imaging evaluation at final follow-up did not reveal any residual disease or recurrence in any patient.
Introduction
Pigmented villonodular synovitis (PVNS) was defined by Jaffe as a benign proliferation of synovial tissue affecting joint, tendon sheath, and bursa. It is a rare, benign disease of the synovial membrane, characterized by hyper-vascular proliferation of the synovium, multinucleated giant cells, macrophages, and hemosiderin deposits, which give it the characteristic brown color. 1 The etiology of this condition is unknown but the presence of aneuploidy and trisomy 7 in diseased synovial cells point to a neoplastic origin. 2 There are two variants based on the extent of involvement; when the entire synovium of a joint is affected, the condition is referred to as diffuse PVNS (DPVNS) and when a single discrete mass is present in the synovium, it is known as localized PVNS (LPVNS). Both forms may arise from intra-articular or extra-articular synovial tissue. The term giant cell tumor of the tendon sheath is used for tenosynovial involvement. Though histological and cytogenetic features of these conditions are identical, they present a different clinical course and are regarded as separate entities. 3,4 Perka et al. postulated that DPVNS is of neoplastic nature, whereas the localized variety is of reactive granulomatous origin due to invasiveness, aneuploidy, high recurrence rate, chromosomal abnormalities, malignant transformation, and metastases seen with DPVNS. 5
PVNS is a locally aggressive lesion that may invade and destroy surrounding soft tissue and bone, resulting in functional deterioration of the joint and the extremity. It may involve any synovial joint but the large joints are affected frequently. The most common localization of DPVNS is the knee, followed by the hip, shoulder, and other joints. 6 Involvement of the axial skeleton (mainly in the posterior elements of spine) has been reported, albeit rarely. 7,8 Recently, PVNS has been reported from the temporomandibular joint as a locally aggressive tumor arising from the base of skull. Both localized and diffuse types of PVNS are common in the age group of 40–50 years, and there is no sex predilection. 2
There are very few studies reporting the clinical outcome and treatment measures for this condition. Various treatment modalities are available for management of PVNS. Surgical options include synovectomy either by arthrotomy or arthroscopy. Nonsurgical adjuvants used are external beam radiotherapy or brachytherapy. 9 The most important factor determining a successful outcome is recurrence of the disease. DPVNS has a higher recurrence rate than LPVNS. By virtue of its localized nature, LPVNS lends itself amenable to successful arthroscopic treatment. 10
Previous reports on management of PVNS have included both diffuse and localized types in a single cohort. In this study, we are reporting our series of patients with LPVNS involving the posterior knee compartment only.
Materials and methods
Our series includes 10 cases (7 male and 3 female) of histopathology proven LPVNS involving the posterior compartment of the knee joint only for whom arthroscopy was done by the senior author (SRT) with at least 1-year follow-up after surgery (range: 12–36 months, average 23 months). The predominant symptom was swelling in all patients and seven patients complained of pain. Seven patients had mechanical symptoms of locking or catching. All patients had previously consulted a primary care physician or orthopedician and the preliminary working diagnosis included nonspecific inflammation, meniscus tear, Morrant-Baker’s cyst, and rheumatological affliction of the knee. All were on some form of anti-inflammatory medication and physical therapy, while 1 of the 10 was initiated on disease modifying antirheumatic drugs for over a year. All patients were examined clinically for effusion, synovitis, range of motion, stability, and meniscal signs. Radiographs of the knee in anteroposterior, lateral, and skyline views along with magnetic resonance imaging (MRI) scan of affected knee were obtained. MRI scans in all cases were indicative of PVNS in only the posterior compartment of knee. All patients were counseled for arthroscopic management and informed consent obtained.
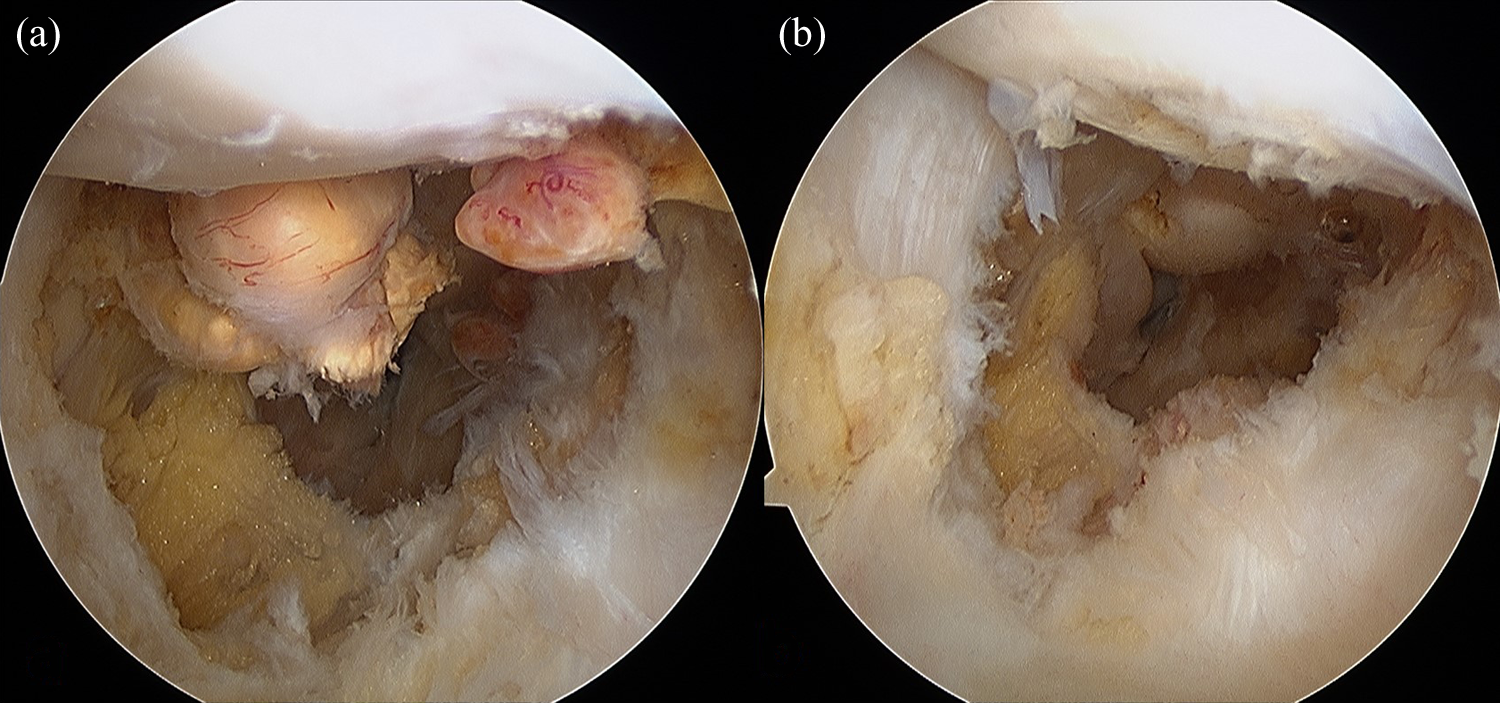
Arthroscopy was performed under tourniquet in supine position under spinal anesthesia. A diagnostic round was done to confirm the diagnosis and look for other intra-articular pathologies. The posterior compartment was approached using the two portal technique. Initially, the posteromedial portal is made using an outside in technique. The 30° arthroscope is passed to the posteromedial aspect of the knee from the standard anterolateral portal in between the medial femoral condyle and the medial edge of the posterior cruciate ligament (PCL). An 18-G spinal needle is passed using the assistance of transillumination, portal created, and a Wissinger rod is inserted. The arthroscope is then shifted to the posteromedial portal over the Wissinger rod for viewing the posterior compartment. The arthroscope is advanced from medial to lateral after taking down the posterior intercondylar septum. The posterolateral portal is then created and a Wissinger rod passed across from posteromedial to posterolateral compartment. The arthroscope is then shifted to the posterolateral portal so that this becomes the viewing portal and the posteromedial portal becomes the working portal. The lesions were identified and were removed completely with the help of a radiofrequency device (VAPR 3®, DePuy Mitek, Reynham, Massachusetts, USA) and a motorized shaver blade (4.5 mm DYONICS Incisor® Plus Elite™, Smith & Nephew, Andover, Massachusetts, USA). The regions where we identified PVNS include the posterior capsular synovium, the medial and lateral gastrocnemius recesses (Figure 1) and as pedunculated mass attached to the PCL near its femoral attachment (Figure 2). The entire diseased synovium and the localized mass were meticulously excised and sent for histopathological examination. Complete macroscopic local clearance was achieved. Intra-articular drains were placed to avoid hemarthrosis. None of the patients received radiotherapy postsurgery. The diagnosis was confirmed on histopathology with typical features seen in each case (Figure 3). Patients were mobilized with crutches and allowed weight bearing as tolerated the next day. Quadriceps, hamstring, and ankle exercises were begun immediately.
(a) Tumor localized near the posterolateral femoral condyle near lateral gastrocnemius origin and (b) after excision.

(a) Tumor attached to the posterior cruciate ligament being excised with a radiofrequency device and (b) after excision when PCL is free. PCL: posterior cruciate ligament.
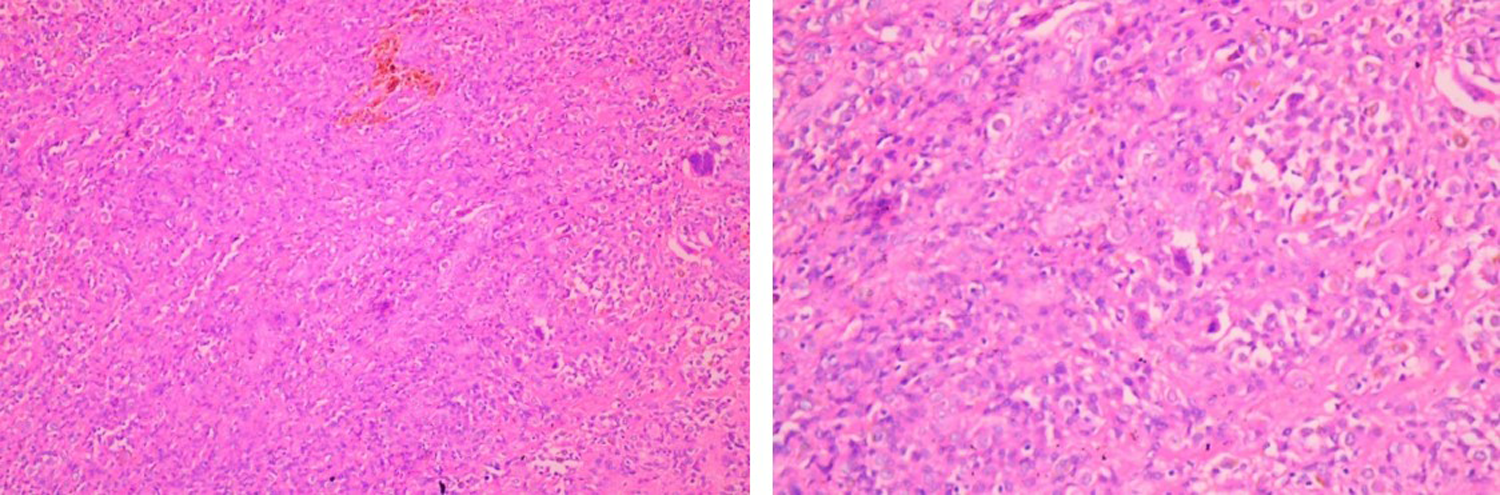
Histopathology examination showing PVNS with typical synovial cell hyperplasia, multinucleated giant cells, macrophages, and hemosiderin deposit: ×10 view and ×40 view. PVNS: pigmented villonodular synovitis.
Results
All patients were followed up at 6 weeks, 3 months, 6 months, and at 6 monthly intervals thereafter. They were evaluated for recurrence of symptoms, and assessment was done using the IKDC subjective knee evaluation form. MRI scan of the knee was performed at last follow-up. There was no incidence of infection, neurovascular damage, deep vein thrombosis, or wound healing problems. The average IKDC score at last follow-up was 85.21 (range: 78.5–90.3). At last follow-up, no patient had any recurrence of the symptom, and follow-up MRI scans did not show any residual disease or recurrence (Table 1).
Patient data.

M: male; F: female.
Discussion
Localized form of PVNS is a well-known entity. Myers presented a series with 166 cases of PVNS of which 6% were patients with articular PVNS. With a prevalence of 1.8/1,000,000 population, this is a rare condition affecting most patients in their 30s. The average age of patients in this cohort was 33 years (range: 22–46 years), typical for PVNS. The duration of symptoms varied from 4 months to 36 months (average 13.9 months) before a definitive diagnosis was made. This was because of both, a delay in seeking medical attention as the symptoms are episodic and because empirical treatment is started initially due to the nonspecific nature of the symptoms. In the series by Dines, the interval between symptom onset and diagnosis was 15 months. 11 Seven patients complained of locking, as mechanical symptoms are more common with LPVNS because the localized and sometimes pedunculated lesion may float freely on the joint and mimic a meniscus tear. 12 Radiographs are usually negative in early PVNS. MRI is the most sensitive and specific tool for diagnosing PVNS but bone involvement in the knee joint is not as common as in the hip, ankle, wrist, or elbow. 13 Hemosiderin is a magnetic material and its deposit in proliferative synovial tissue results in a spotty low signal or extensive low-signal area within the synovial masses on T1- (T1WI) (Figure 4) and T2-weighted (T2WI) images, best seen on fast field echo (FFE) sequence MRI images (Figure 5). Fat-suppressed sequences obscure the deposit. This is diagnostic of PVNS. The MRI features of PVNS include variable extent of synovial proliferation, joint effusion, and erosion of bone, and in particular the deposit of hemosiderin within the synovial masses. 13 An almost similar lesion is the localized nodular synovitis. It shares radiological and histological features with LPVNS but the presence of diffuse frond-like projections of synovium and an abundance of hemosiderin deposition serve as distinguishing observations. 14

T1-weighted MRI images show well-defined, lobulated isointense lesions localized to the posterior compartment. MRI: magnetic resonance imaging.

T2-weighted proton density sagittal MRI images showing the lesions located posterior and superior to the posterior cruciate ligament (yellow arrows). MRI: magnetic resonance imaging.
Treatment of PVNS can be by multiple modalities like open or arthroscopic excision, radiotherapy—by external beam or intra-articular yttrium-90 injection. In cases with advanced joint destruction, joint replacement and arthrodesis may be needed but, at that time also, performing a complete synovectomy is imperative. LPVNS of the knee is amenable to complete resection, and achieving total macroscopic disease removal is crucial. The posterior compartment of the knee is one area which is perhaps better approached arthroscopically than by open surgery, is view of the complex anatomy and vicinity of neurovascular structures and lesser morbidity with the minimally invasive approach. In all our patients, we were able to remove the entire diseased synovium by approaching through the posteromedial and posterolateral portals. The prognosis of localized form of PVNS is better than the diffuse form. Recurrence of the disease is the most important prognostic factor and it is more common with the diffuse type than the localized and higher in larger joints. 15 Recurrent PVNS tumors were more likely to be located in the knee, which may be related to larger tumor size. Patient age, sex, completeness of surgical removal, DNA ploidy, and MIB-I proliferation were not significantly different between recurrent and nonrecurrent lesions in their group. 16
Schwartz demonstrated that a disease-free margin is one of the important factors in prevention of recurrence. They also observed that rate of recurrence increases with time and was highest in the knee joint. Mean rate of recurrence was 7% in the first year and 15% at 5 years. The probability of continuous recurrence-free survivorship at 25 years was 65%. 6 We did not have any recurrence in our patient cohort (longest follow-up of 36 months, average 23 months). Byers’ series included patients with DPVNS and LPVNS. Among those with involvement of the knee joint, 2 of 13 patients with LPVNS had a recurrence after open excision, whereas this rate was 46% for the diffuse group following extensive synovectomy. The authors attributed this to the failure to eradicate all diseased tissue. 17 Flandry reported a recurrence in 2 of 23 patients with DPVNS of the knee who were treated by open total synovectomy and extensor mechanism realignment to manage redundancy of retinacular tissue caused by chronic distension. Eight of this group developed early knee stiffness and underwent closed manipulation. 18 Thus, an open surgery to achieve clear margins in diffuse disease reduces recurrence but is associated with scarring as well. This is not a problem with LPVNS. In our study, all patients had localized disease limited to the posterior compartment of the knee. These were treated by arthroscopic synovectomy. Arthroscopic synovectomy is always better than open synovectomy when disease is limited as the postoperative morbidity is less and disease can be cleared better than open procedure. Ogilvie-Harris reported no recurrence in their five patients with localized knee PVNS who underwent arthroscopic local excision. However, in the patients who had had DPVNS, the rate of recurrence was lower (1 in 11) in those who had had a complete arthroscopic synovectomy than in those (5 in 9) who had had a partial arthroscopic synovectomy (p = 0.01). 19
In Dines’ series of LPVNS, there was no recurrence on long-term follow-up of average 65.8 months. Three of 26 patients in their study had the tumor localized in the popliteal fossa. 11
Zvijac reported two recurrences in their series of 12 patients with DPVNS but none in cases of LPVNS treated by arthroscopic synovectomy. There were no complications, and 10 patients (72%) were rated as excellent or good, 2 patients (14%) as fair, and 2 patients (14%) as poor on subjective assessment. 20
Kubat presented a series with four LPVNS and nine DPVNS patients in knee, all treated with arthroscopic synovectomy and followed up for average 84 months. One patient with diffuse disease developed recurrence but all others were rated as “excellent” on subjective assessment. 21 De Ponti reported arthroscopic treatment of 19 patients who had PVNS. Fifteen patients who had the diffuse form of the disease underwent partial (eight patients) or total (seven patients) synovectomy. No significant complications related to surgery like infection, neurovascular injury, or stiffness were encountered, although patients treated with extensive synovectomy showed slower functional recovery. In the partial synovectomy group, 50% cases recurred with obvious clinical symptoms (effusion, pain, and movement impairment). 10
A recent literature review by Auregan et al. 22 revealed that the recurrence rate was 0–8% for LPVNS and 8–70% for DPVNS. For LPVNS, there was no difference found in terms of local recurrence (8.7% for open synovectomy and 6.9% for arthroscopic synovectomy) and postoperative complications (<1% for open synovectomy and 0% for arthroscopic synovectomy). Similarly, for DPVNS, no difference was found in terms of local recurrence following open synovectomy (22.6%) or arthroscopic synovectomy (16.1%), but complication rates were much higher following open synovectomy. 22 Radiation therapy is a safe and effective treatment for PVNS in the postoperative setting after incomplete resection and also as a salvage option for treatment of recurrences it provides a high rate of local control. This can be either external beam radiation therapy or intra-articular injection of radioactive material as yttrium-90 (90Y). 23 Internal irradiation or external beam radiation as an adjuvant treatment to surgical synovectomy seemed to decrease the rate of local recurrence in DPVNS case. 22 No patients in our study were put on radiation therapy as this was deemed unnecessary based on current evidence.
To the best of our knowledge, we are presenting the only series of PVNS localized to posterior compartment of knee joint, managed by arthroscopic synovectomy with excellent clinical outcomes postoperatively.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.