
Abstract
Background:
Arthroscopic suture repair is the main treatment option for hip labral tears; however, anchor insertion and placement from arthroscopic portals is difficult.
Purpose:
To quantitatively evaluate the safety of various arthroscopic portals for suture anchor placement during hip labral repair.
Study Design:
Descriptive laboratory study.
Methods:
The computed tomography scans of 20 patients with normally developed hip joints were used to create 3-dimensional models. The distances from the anchor to the articular cartilage (DAC) and from the acetabular insertion point to the cortical bone (DCB) were measured in the anterolateral portal (AL), posterolateral portal (PL), midanterior portal (MAP), medial MAP, and 3 distal anterolateral accessory portals (DALAs): DALA-proximal, DALA-middle, and DALA-distal. Labral tears were divided into anterior (4, 3, and 2 o’clock), lateral (1, 12, and 11 o’clock), and posterior (10, 9, and 8 o’clock) acetabular zones, and the Kruskal-Wallis and Mann-Whitney U test were used to compare DAC and DCB in the zones. The success rate was defined as anchors placed with DAC ≥1 mm and DCB ≥15 mm.
Results:
The DAC was significantly smaller in the AL at 1 o’clock (0.68 ± 0.32 mm; P < .001) and 12 o’clock (0.37 ± 0.30 mm; P < .001), and in the PL at 12 o’clock (-0.35 ± 0.38 mm; P < .001) and 11 o’clock (0.60 ± 0.24 mm; P < .001). The DCB was significantly smaller in the DALA-P at 3 o’clock (8.93 ± 2.12 mm; P < .001) and 11 o’clock (9.59 ± 2.84 mm; P < .001), the MAP at 12 o’clock (13.76 ± 3.89 mm; P < .001) and 11 o’clock (0.27 ± 0.27 mm; P < .001), and the MMA at 12 o’clock (5.96 ± 2.31 mm; P < .001) and 11 o’clock (0 mm; P < .001). Success rates were high for MAP and MMA between 4 o’clock and 1 o’clock, for DALA-proximal at 12 o’clock, for AL at 11 o’clock, and for PL between 10 o’clock and 8-o’clock.
Conclusion:
There were significant differences in the success rate of anchor placement using different portals during hip arthroscopic labral repair.
Clinical Relevance:
MAP is recommended for labral repair between 4 o’clock and 1 o’clock, DALA-P is recommended between 2 o’clock and 12 o’clock, AL is suitable at 11 o’clock, and PL is suitable between 10 o’clock and 8 o’clock.
Hip labral tears are caused by injuries, structural problems, or degenerative conditions and are associated with pain, locking or clicking, limited range of motion, and joint stiffness. 11 Due to the histological structure of fibrocartilage and poor acetabular labrum blood supply, 19 arthroscopic surgery is often required for labral tears to restore the sealing suction of the labrum, 20,27 and prevent degenerative changes and osteoarthritis of the hip joint. 15,23
Arthroscopic suture repair is the main treatment option for labral tears; suture anchors provide reliable fixation for suture repair and reconstruction of the labrum. 8,10,15,17 However, unlike the shoulder joint, anchor insertion and placement from arthroscopic portals is more difficult in the hip joint due to the long soft tissue tunnel and limited operative range. Details regarding the safety and complications of anchor placement in hip arthroscopy have been reported in cadaveric studies. 5,9,26 According to the results of some studies, there is no difference in the safety of various portals with the same placement position, 5,9 while other results have suggested that the safety performance of some portals was better. 26 However, the current literature lacks comprehensive evaluations of the safety and success rates of anchor placement that would allow optimizing portals for common labral tear regions.
The aim of this study was to evaluate the safety parameters of suture anchor placement using 3-dimensional (3-D) models from hip computed tomography (CT) scans. It was hypothesized that there will be differences in safety parameters and success rates with different portals during hip arthroscopic labral repair.
Methods
3-D Model Reconstruction
Institutional review board approval was obtained for the study protocol. A total of 20 CT scans (Energy Spectral CT, Siemens) of patients with normally developmental hip joints taken between June 1, 2021 and October 31, 2022 were included in the study. Inclusion criteria were acetabular abduction angle of 35° to 55°, acetabular anteversion angle of 5° to 25°, and femoral neck anteversion angle of 5° to 20°. Exclusion criteria were Tönnis grade ≥2 osteoarthritis, femoral-acetabular impingement, and developmental dysplasia of the hip. The 3-D models were reconstructed using Mimics (Version 19; Materialise) and optimized using Geomagic Wrap (Version 2021; Geomagic).
The 3-D hip models were used to test the safety of anchor placement during hip arthroscopic repair under various portals. The portals and their locations are shown in Figure 1. The anterolateral portal (AL), posterolateral portal (PL), anterior portal (AP), midanterior portal (MAP), and distal anterolateral accessory portal (DALA) were located using anatomic marks, including the anterior superior iliac spine, the lateral margin of the patella, and the tip of the greater trochanter after rotation and traction of the femur. 24 The medial MAP (MMA) was 1 cm medial to the MAP. In addition, 3 typical DALAs distributed on the anterior margin of the femur were located based on positions reported in the literature: DALA-proximal (DALA-P), 5,7 DALA-middle (DALA-M), 26 and DALA-distal (DALA-D). 24
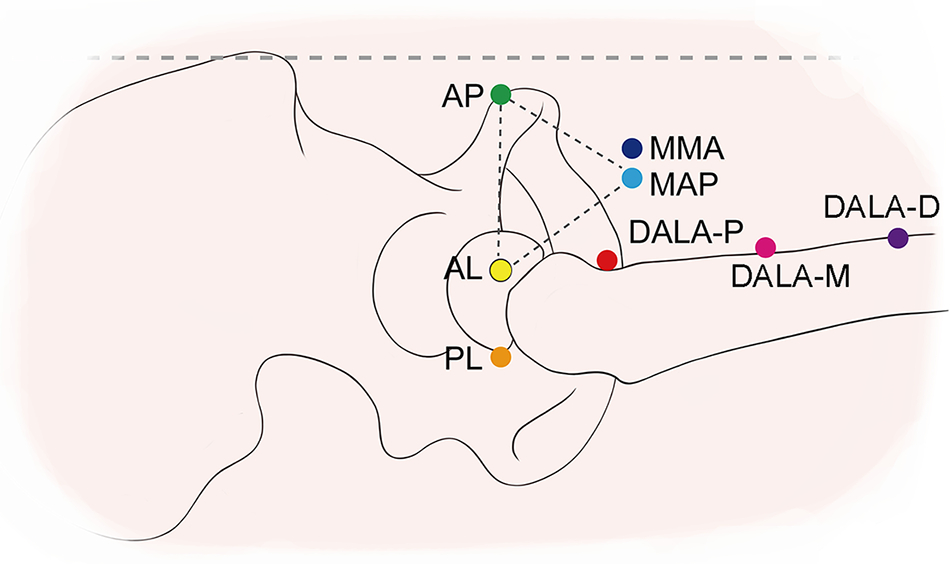
Schematic diagram of portals used during hip arthroscopic labral repair. The horizontal dashed line indicates the line from the anterior superior iliac spine to the lateral border of patella. The AL is 1 cm superior and 1 cm anterior to the tip of greater trochanter. The PL is 1 cm superior and 1 cm posterior to the tip of greater trochanter. The AP is at the same level as the AL and 1 cm lateral to the line between the anterior superior iliac spine and the lateral margin of the patella. The MAP is the distal vertex of an equilateral triangle composed of the AL, AP, and MAP (dashed lines). The MMA is 1 cm medial to the MAP. Three typical DALAs are distributed on the anterior margin of the femur: DALA-P, DALA-M, and DALA-D. DALA-P is 5 cm distal to, but in line with, the AL. DALA-M is the distal vertex of an isosceles triangle composed of DALA-M, MAP, and AL; the distance between MAP and AL is equal to the distance between MAP and the DALA-M. The distance between DALA-D and AL is 1.5 times the distance between AL and DALA-M. AL, anterolateral portal; AP, anterior portal; DALA, distal anterolateral accessory portal; DALA-D, DALA-distal; DALA-M, DALA-middle; DALA-P, DALA-proximal; MAP, midanterior portal; MMA, medial midanterior portal; PL, posterolateral portal.
Surgical Procedure and Suture Anchor Placement
The positions of the acetabulum were described using the clock face, 1 and labral tears were divided into anterior (4, 3, and 2 o’clock), lateral (1, 12, and 11 o’clock), and posterior (10, 9, and 8 o’clock) zones (Figure 2A). 21 A 3-mm anchor was inserted 2 mm from the acetabulum cartilage to simulate the surgical procedure. 7 Safety data were measured in a plane formed by the insertion point, the hip center, and the portal (Figure 2B).

(A) The position of the acetabulum was described using a clock face, with 6 o’clock at the midpoint of the transverse acetabular ligament and 3 o’clock at anterior acetabulum. Labral tears were divided into anterior (4, 3, and 2 o’clock), lateral (1, 12, and 11 o’clock), and posterior (10, 9 and 8 o’clock) zones. (B) A 3-mm anchor was inserted 2 mm from the acetabulum cartilage in the acetabulum model. Safety data were measured in a plane formed by the insertion point (cyan), the hip center (green), and the portal (yellow).
Safety Parameters
The distance from the anchor to the articular cartilage (DAC), which represents the risk of articular cartilage violation, and the distance from the acetabular insertion point to the cortical bone (DCB), which represents the risk of cortical bone penetration, were the 2 major safety parameters. The DAC is the smallest distance between the anchor and articular cartilage (Figure 3), while the DAC was the maximum distance perpendicular to the anchor of the articular cartilage when the anchor has passed through the articular cartilage. Articular cartilage violation occurs when the DAC is <1.0 mm. The DCB is the distance from the acetabular insertion point to the cortical bone of the acetabulum along the direction of the anchor (Figure 3). Cortical bone penetration occurs when DCB is <15 mm.

Safety parameters. The DAC represents the risk of articular cartilage violation. DAC (white arrow) is the shortest distance between the anchor and the articular cartilage. DAC is the maximum distance perpendicular to the anchor when the anchor has passed through the articular cartilage. DAC <1.0 mm was considered articular cartilage violation. The DCB represents the risk of cortical bone penetration. DCB (red arrow) is the distance from the insertion point to the cortical bone of the acetabulum along the direction of the anchor. DCB <15 mm was considered cortical bone penetration. DAC, distance from the anchor to the articular cartilage; DCB, distance from the acetabular insertion point to the cortical bone.
Two supplementary safety parameters, the angle of anchor deviation (AAD) and the length of operating path (LOP), were also used. The AAD (θ) is the angle between the actual direction (d a) and the ideal direction (d i) of the anchor perpendicular to the acetabular opening plane. 13 It was computed from the vector of orientations in the x, y, and z planes:


The LOP is the distance between the portal (A) and the insertion point (B) and was computed using the coordinates the x, y, and z planes:



Smaller AADs represent greater safety, and shorter LOPs have better handling.
Finally, we calculated the success rate of anchor placement according to portal and acetabular zone, in which successful placement was defined as a DAC of ≥1 mm and a DCB of ≥15 mm.
Statistical Analysis
The sample size for this study was determined based on previous studies with similar methodologies. Descriptive statistics were reported as the means and standard deviation. The Kruskal-Wallis method with Bonferroni correction was used to compare the safety parameters (DAC, DCB, AAD, and LOP) of the portals (AL, PL, AP, MAP, MMA, DALA-P, DALA-M, and DALA-D) in the anterior and lateral acetabular zones, and the Mann-Whitney U test was used to compare the safety parameters of the portals in the posterior acetabular zones. Success rates were compared using the Fisher exact test with Bonferroni correction. Statistical significance was determined using a 95% significance level. Statistical analyses were performed using SPSS statistics software (Version 25.0, IBM Corp).
Results
Reconstruction of the 3-D Hip Model
Twenty 3-D hip models were reconstructed based on 1-mm CT scans of patients. The 20 participants had a mean age of 67.3 ± 2.56 years (range, 37-82 years), mean height of 174.75 ± 8.16 mm (range, 150-178 mm), mean weight of 69.5 ± 12.52 kg (range, 51-96 kg), and mean body mass index of 25.72 ± 4.75 (range, 18.34-33.25). Acetabular abduction, acetabular anteversion, and femoral neck anteversion were analyzed in the 3-D models; the results showed that they were all within the normal range, with mean values of 48.50° ± 0.53° (range, 43.85°-52.23°), 18.18 ± 0.84° (range, 12.45-23.66°), and 13.95 ± 0.60° (range, 10.30-19.95°), respectively.
Safety Profiles of the Different Portals
Table 1 presents the safety parameters of the portals for anchor placement. The results showed that there was a higher risk of complications in some portals during anchor placement. Smaller DAC values, indicating the piercing of the acetabular articular surface at these positions, were present in the AL at 1 o’clock and 12 o’clock and in the PL at 12 o’clock and 11 o’clock. DCB values of <15 mm, which indicated piercing through the cortex, were present in the DALA-P, DALA-M, and DALA-D at 3 o’clock, in the MAP, MMA, DALA-M, and DALA-D at 12 o’clock, and in the MAP, MMA, DALA-P, DALA-M, and DALA-D at 11 o’clock (Figure 4).
Safety Parameters of Portals at Insertion Positions a

a Data are reported as mean ± SD. Boldface text indicates values with DAC ≥1 mm and DCB ≥15 mm. Dashes indicate areas not applicable. AAD, angle of anchor deviation; AL, anterolateral portal; DAC, distance from the anchor to articular cartilage; DALA-D, distal-anterolateral accessory portal-distal; DALA-M, distal-anterolateral accessory portal-middle; DALA-P, distal-anterolateral accessory portal-proximal; DCB, distance from the insertion point to cortical bone; LOP, length of the operating path; MAP, midanterior portal; MMA, medial midanterior portal; PL, posterolateral portal.
b-d Superscripts with the same letters indicate a lack of statistical difference on pairwise comparison.
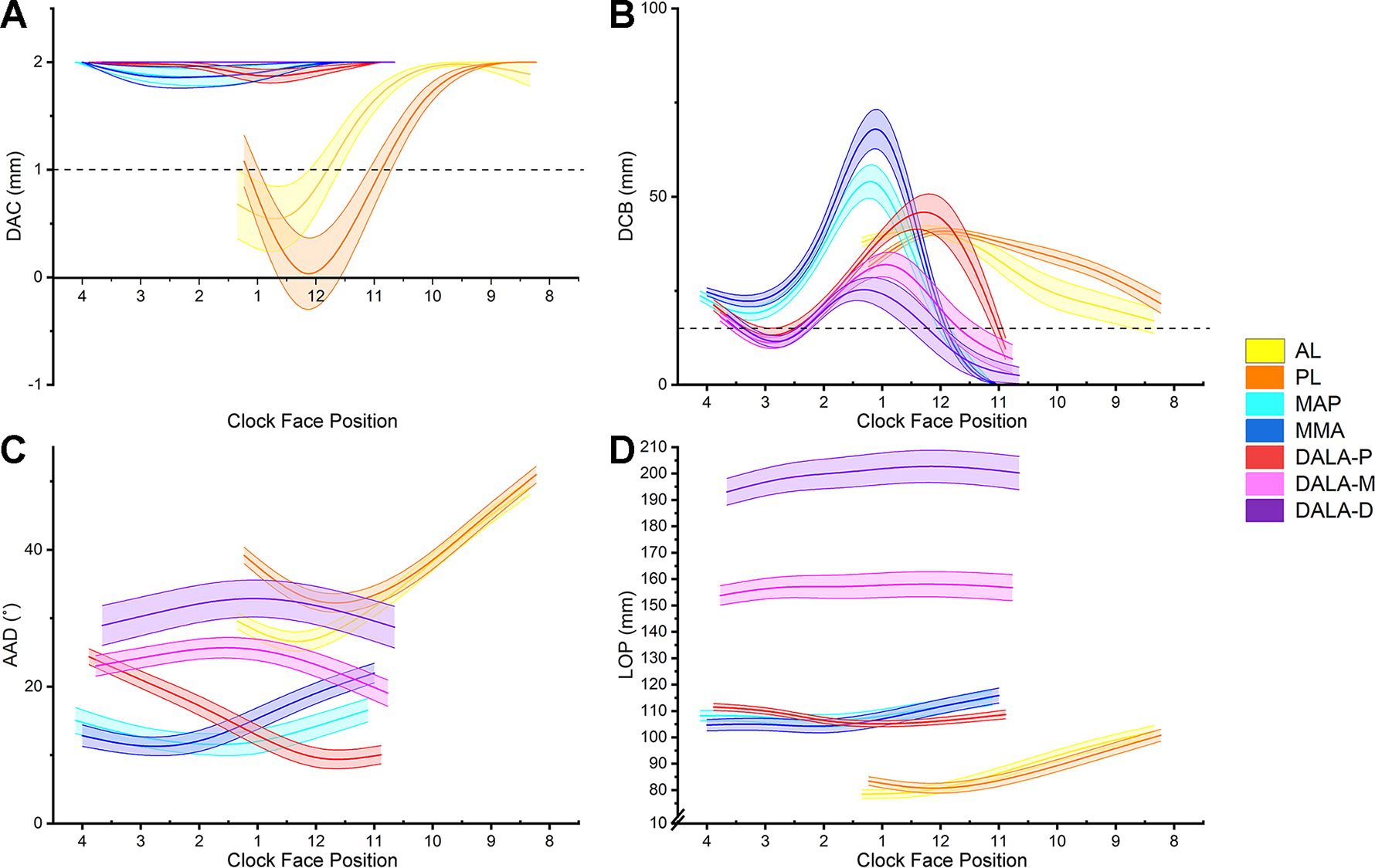
Safety parameters of portals at the insertion position: (A) DAC, (B) DCB, (C) AAD, and (D) LOP. Data are presented as means, with shaded areas representing standard deviations. AAD, angle of anchor deviation; AL, anterolateral portal; DAC, distance from the anchor to the articular cartilage; DALA-D, distal-anterolateral accessory portal-distal; DALA-M, distal-anterolateral accessory portal-middle; DALA-P, distal-anterolateral accessory portal-proximal; DCB, distance from the insertion point to the cortical bone; MAP, midanterior portal; MMA, medial midanterior portal; LOP, length of the operating path; PL, posterolateral portal.
Conversely, there were preferable safety parameters in some portals during anchor placement. MAP and MMA were prominent for anchor placement in the anterior acetabulum. There were longer DCBs in MAP and MMA at 4 o’clock and 3 o’clock. The DCB of the MMA was greater than that of MAP at 3 o’clock, although the difference was not statistically significant. DALA-P was advantageous for anchor placement in the lateral acetabulum between 12 o’clock and 1 o’clock. There was a larger DAC in DALA-P, MMA, and MAP at 1 o’clock. Furthermore, DALA-P was advantageous for anchor placement at 12 o’clock because the DAC of DALA-P was greater than that of AL and PL; in addition, the DCB of DALA-P was greater than that of MMA, MAP, DALA-M, and DALA-D. However, AL was the only portal suitable for anchor placement at 11 o’clock due to greater DAC than for PL and greater DCB than MMA, MAP, DALA-P, DALA-M, and DALA-D (Table 1).
AL and PL are the portals used most commonly for anchor placement at the posterior acetabulum. There were greater safety parameters in PL than in AL, although the difference was not statistically significant.
The results for the supplementary safety parameters, AAD and LOP, were consistent with those of the DAC and DCB between 4 o’clock and 12 o’clock. There were smaller AAD and shorter LOP in MAP and MMA at 4 o’clock and 3 o’clock; AAD and LOP were likewise smaller and shorter, respectively, in DALA-P, MAP, and MMA at 2 o’clock, in DALA-P and MAP at 1 o’clock, and in DALA-P at 12 o’clock. There was a smaller AAD in DALA-P and a larger LOP in AL and PL at 11 o’clock. In the posterior acetabulum, there were no significant differences in AAD and LOP between 10 o’clock and 8 o’clock.
Success Rates of Anchor Insertion From Different Portals
The success rates and the frequencies of intra-articular cartilage damage and cortex penetration are reported in Table 2. MAP, MMA, DALA-P, AL, and PL had favorable success rates for anchor placement from anterior to posterior. At 4 o’clock, the success rates of MMA (100%) and MAP (100%) were higher than those of DALA-P (75%), DALA-M (75%), and DALA-D (70%), although the difference was not statistically significant. At 3 o’clock, MMA had the highest success rate of 65%, which was significantly greater than that of DALA-M (15%) and DALA-D (10%). There were high success rates at 2 o’clock for MMA (95%), MAP (95%), DALA-P (95%), DALA-M (100%), and DALA-D (100%).
Success Rates and Complications of Portals According to Acetabular Zone for 3-mm Anchor Insertion a

a Boldface text indicates success rates of ≥60%. Dashes indicate areas not applicable. ACV, articular cartilage violation; AL, anterolateral portal; CBP, cortical bone penetration; DALA-D, distal-anterolateral accessory portal-distal; DALA-M, distal-anterolateral accessory portal-middle; DALA-P, distal-anterolateral accessory portal-proximal; MAP, midanterior portal; MMA, medial midanterior portal; PL, posterolateral portal.
b -d Superscripts with the same letters indicate a lack of statistical difference on pairwise comparison.
Most portals had satisfactory success rates (85%-95%) at the 1-o’clock position except for DALA-D (50%), AL (55%), and PL (60%) (Table 2). Remarkably, only DALA-P (75%), whose success rate was significantly greater than that of MMA (15%) and DALA-D (5%), had a suitable success rate for anchor insertion at 12 o’clock. AL had the highest success rate of 75% at 11 o’clock, which was significantly greater than that of MAP (0%), MMA (0%), DALA-M (10%), and DALA-D (5%). AL and PL were both suitable for anchor placement at the posterior acetabulum. However, PL (85%, 95%, and 80%, respectively) performed better between 10 o’clock and 8 o’clock compared with AL (60%, 65%, and 60%, respectively).
Figure 5 shows a summary of the success rates for each portal according to acetabular clock face position. The highest success rates for the portals at 4 o’clock, 2 o’clock, 1 o’clock, and 9 o’clock were 100%, 100%, 95%, and 95%, respectively. However, the highest success rates at 3 o’clock, 12 o’clock, and 11 o’clock were 65%, 75%, and 75%, respectively, indicating the difficulty of anchor placement at these positions.

Success rate of the portals for anchor insertion from the anterior 4-o’clock to the posterior 8-o’clock positions. The success rate was proportional to the distance between the portal and the center: 0% near the center and 100% for the portal farthest from the center. The maximum success rate (%) for each position is marked. AL, anterolateral portal; DALA-D, distal-anterolateral accessory portal-distal; DALA-M, distal-anterolateral accessory portal-middle; DALA-P, distal-anterolateral accessory portal-proximal; MAP, midanterior portal; MMA, medial midanterior portal; PL, posterolateral portal.
Discussion
The primary finding of the study was that there were significant differences in the success rate of anchor placement using different portals during hip arthroscopic labral repair. The success rates of MAP (100%) and MMA (100%) were higher at 4 o’clock (P = .003). The success rate of MAP (45%) and MMA (65%) were higher at 3 o’clock (P = .001). The success rate of DALA-P (95%), MAP (95%), and MMA (95%) were higher at 1 o’clock (P < .001). The success rate of DALA-P (75%) was higher at 12 o’clock (P < .001). The success rate of AL (75%) was higher at 11 o’clock (P < .001). And the success rate of PL (85%, 95%, and 80%, respectively) was higher at 10 o’clock (P = .157), 9 o’clock (P = .048), and 8-o’clock (P = .177).
Articular cartilage injuries and cortex penetration are complications of labral repair that surgeons seek to avoid during hip arthroscopy. The effectiveness of utilizing various portals in improving success rates and reducing complications during hip arthroscopic labral repairs has previously been documented. Stanton et al 26 reported that placement using DALA rather than MAP and AL improved safety in the anterior acetabulum. However, previous studies either lacked indicators for evaluation or were not designed for investigating commonly used portals. In the present study, we optimized portal selection by quantitatively assessing their safety for suture anchor placement in 3-D hip models.
There was higher safety for anchor placement in MAP between 4 o’clock and 1 o’clock, in DALA-P between 2 o’clock and 12 o’clock, in AL at 11 o’clock, and in PL between 10 o’clock and 8 o’clock. However, the highest success rate was only 45% when the placement was with MAP at 3 o’clock due to articular cartilage damage (1/20) and cortex penetration (10/20). The anchor tended to perforate the medial cortex at 3 o’clock; this perforation could lead to persistent hip pain and reoperation. 4 Therefore, we attempted to modify the MAP by moving 1 cm medially and found a neoportal, MMA, which was a soft spot of the thigh that provided a gap between the rectus femoris and gluteus medius. It was easier to breach the capsule and enter the joint through this gap. This was supported by the finding that there was a longer DCB of 19.55 ± 1.82 mm and a higher success rate of 65% in MMA at 3 o’clock. Thus, MMA may be a better alternative to MAP for labral repairs between the 4-o’clock and 1-o’clock positions to reduce the risk of medial cortex penetration.
There was higher safety for anchor placement in MAP between 4 o’clock and 1 o’clock. This observation was in agreement with the finding reported by Degen et al, 5 who demonstrated that MAP had a higher success rate than DALA at 3 o’clock and 4 o’clock, although the difference was not statistically significant. There were no significant differences between MAP and DALA from the anterior 2-o’clock position to the posterior 9-o’clock position. The alterable distances between the anchor and chondrolabral junction (from 0.1 ± 0.40 to 3.4 ± 1.55 mm) in their study, differing from fixed distances in the present study, may be the reason for reduced difference in success rates. In addition, Foster et al 9 reported that the distance from the thin drill bit (1.4 mm) to the articular surfaces, similar to DAC in the present study, was not significantly different between MAP and DALA at 3 o’clock and 4 o’clock. Their findings were consistent with those of the present study. Moreover, Foster et al 9 demonstrated that PL was safe for anchor placement from posterior 11 o’clock to 8 o’clock. AL (75%) was safer than PL (40%) at 11 o’clock, and PL was safer from 10 o’clock to 8 o’clock in the posterior acetabulum in the present study. This difference may be explained by the underestimation of anchor size and the lack of contrast in the Foster et al 9 study.
This study has not confirmed the research by Stanton et al, 26 who indicated that DALA was safer than MAP from 2 o’clock to 3 o’clock and AL from 1 o’clock to 12 o’clock on account of the larger distance between the pin and the articular surface, which was similar to DAC in the present study. There are several possible explanations for our seemingly paradoxical result. First, their study compared the distance between the pin and the articular surface at the same depths of insertion. While the smallest distance between the anchor and the articular surface was compared at all depths of insertion in the present study. Second, the DAC at the same insertion point in the present study differed from the average distance from 2 o’clock to 3 o’clock in their research. Finally, there were only 6 cadaveric hip specimens and 4 insertion positions in the study by Stanton et al. 26 Therefore, morphological differences between specimens could account for the conflicting results. In contrast, morphologic differences between the groups were entirely removed using a series of uniform 3-D models in the present study.
In addition to portal selection, researchers in previous studies have attempted to develop guidelines for anchor placement to enhance safety. The results of several studies have suggested that a small anchor is a good alternative due to the larger safe angle of insertion and smaller margin for error regarding articular perforation, 12,25 especially at 3 o’clock. The performance of the small anchor (1.8 mm) was no less than that of the common anchor (2.9 mm) in cyclic load testing and ultimate failure strength. 3,6 We analyzed the success rate of using smaller anchors (1.8 mm) based upon the current data (Supplemental Table S1). The use of small anchors slightly increased the success rate of partial portals. However, the conclusions of the present study were not affected. Furthermore, curved suture anchor drill guides were recommended by Nho et al, 22 who found that curved guides had a greater angle of insertion and longer distance to the articular cartilage at the 1-o’clock position. However, the use of a curved or straight drill guide did not make a statistically significant difference in perforating the subchondral bone and breaching the outer cortex at the 3-, 2-, 1-, 12-, and 11-o’clock positions, which was reported by Dumont et al. 7 Further work is required to establish the value of curved suture anchor drill guides for anchor placement during hip labral repair.
The anatomic characteristics also influenced the safety of anchor placement. 18 The opening direction of the acetabulum, impacted by coxa vara, coxa valga, and acetabular anteversion, is a key factor for locating the portals. The location of portals may change with the opening direction of the acetabulum in patients with abnormal anatomy. In addition, there are some risks of injuring blood vessels and nerves around the hip during hip labral repair procedures. 24 The major risk comes from the AP, which is close to the lateral femoral cutaneous nerve. There is also a risk of injury to the small terminal branch of the ascending lateral circumflex femoral artery, which is close to the MAP and AP. Thus, modifying the MAP by moving 1 cm medially may increase the injury risk of the small terminal branch of the ascending lateral circumflex femoral artery. It is advisable to start an arthroscopic procedure with classic portals and perform complementary portals according to intraoperative requirements. 28 However, hip arthroscopy complications are rare. The rate of complication was 1.4% to 1.6% during hip arthroscopy. In addition, a direct injury to the structures is less reported during hip arthroscopy compared with complication due to distraction. 2,14 There is an anatomic study will be performed in the future to ensure the safety of MMA portals.
The characteristics of the acetabulum itself also pose challenges for anchor placement. The present study demonstrated that inserting anchors at 3 o’clock, 12 o’clock, and 11 o’clock was not uneventful, with maximum success rates of 65%, 75%, and 75%, respectively. This was consistent with previous studies, in which a high risk of complications at the 3-o’clock position was reported. 4,5 Structural characteristics of the acetabulum may contribute to cortical perforation and articular damage. Two depressions were found on the anterior and posterosuperior walls. 16 Furthermore, the anterior acetabulum corresponded to the psoas valley. 29 The thin, low bone walls may increase the risk of complications at the 3-o’clock position during hip arthroscopic labral repair. 4,5,18,25 Notably, the maximum success rates for the portal were 65%, 75%, and 75% at the 3-, 12-, and 11-o’clock positions, respectively, which were lower than those reported by Degen et al 5 (100%, 100%, and 88%, respectively). The anchor was inserted at a point 2 mm from the chondrolabral junction, and, considering the deviation of labral repair operation, a 1 mm safe distance was maintained between the anchor and the articular cartilage in the present study, which may explain this difference. The actual situation in clinical practice may be more optimistic.
We also investigated the relationship between the portal and anchor insertion points. The orientation of the acetabulum, which depends on the abduction and anteversion angles, greatly affects the safety of portals for anchor placement. We set up a Cartesian coordinate system in the opening plane of the acetabulum with its rotational center as the origin. Portal distribution was closely related to the safety of placement positions (Figure 6). For example, MMA was distributed anteriorly in the coordinate system, approximately 3 o’clock, which may account for the maximum high success rate in this position. Meanwhile, DALA-P was distributed superiorly at approximately 12 o’clock, which made it more advantageous in this position. PL was distributed more posteriorly than AL and was advantageous in the posterior acetabulum. However, the underlying mechanisms of anchor placement require exploration in future studies.
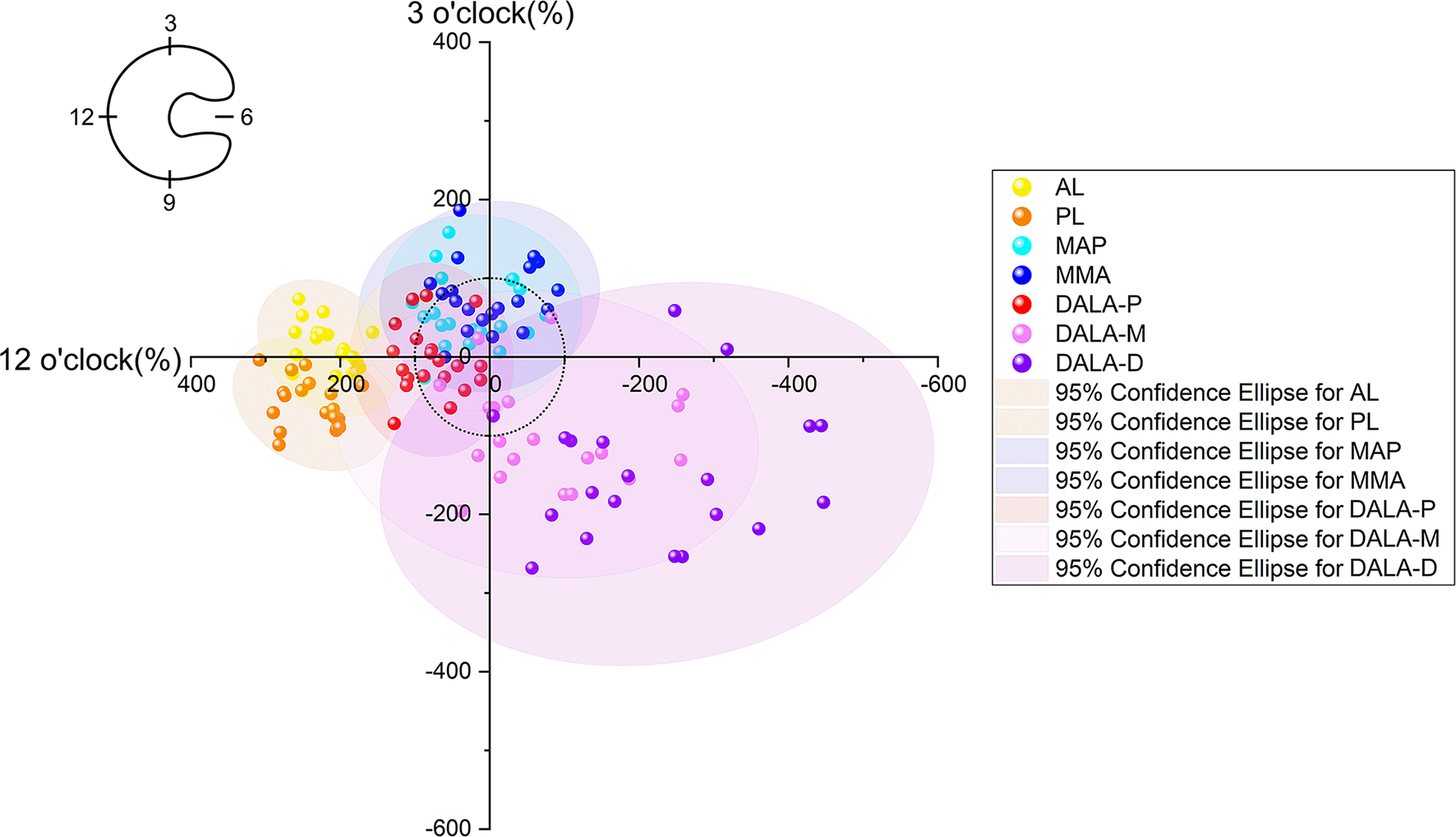
A Cartesian coordinate system was established on the opening plane of the acetabulum in the supine position, with the acetabular rotation center as the origin. The orientation from the origin to 3 o’clock was the positive x-direction (anterior acetabulum), while the orientation from the origin to 12-o’clock was the positive y-direction (superior acetabulum). The radius of each acetabulum was taken as a 100-unit length. The portals were projected onto this plane along the direction of the opening plane. The MMA (blue) was distributed anteriorly in the coordinate system, at approximately 3 o’clock, and the DALA-P (red) was distributed superiorly, at approximately 12 o’clock. AL, anterolateral portal; DALA-D, distal-anterolateral accessory portal-distal; DALA-M, distal-anterolateral accessory portal-middle; DALA-P, distal-anterolateral accessory portal-proximal; MAP, midanterior portal; MMA, medial midanterior portal; PL, posterolateral portal.
Limitations
There were some limitations to this study. First, the normally developed acetabulum was involved in the present study. The results may be discrepant in patients with hip deformities, which include pincer lesions, acetabulum defects or abnormal acetabular anteversion. Second, there were 20 samples tested in each group. Using a larger number of samples is likely to provide results that are close to the actual situation. Third, the impact of body shape and soft tissue anatomy were not analyzed in the present study. The results of this study may not apply to patients who are extremely obese or thin. Fourth, the mean age was significantly greater than that of patients who generally undergo arthroscopic labral repairs. This may limit the generalizability of these results. Finally, the 3-mm anchor and an error distance of 1 mm were used for anchor placement in the hip model although smaller anchors and lesser error distances were available.
Conclusion
The present study provides an appropriate portal for anchor placement, which may reduce the risk of complications. The primary finding was that MAP, DALA-P, AL, and PL are suitable for anchor placement in the anterior 4- to 1-o’clock, anterosuperior 2- to 12-o’clock, posterosuperior 11-o’clock, and posterior 10- to 8-o’clock positions, respectively. In addition, MMA may be a risk mitigation alternative for MAP at the 3-o’clock position.
Supplemental material for this article is available at https://journals.sagepub.com/doi/full/10.1177/23259671231189729#supplementary-materials
Supplemental Material
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671231189729 - Portal Selection for Suture Anchor Placement During Hip Arthroscopic Labral Repair: A Study Based on 3-Dimensional Model Reconstruction
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671231189729 for Portal Selection for Suture Anchor Placement During Hip Arthroscopic Labral Repair: A Study Based on 3-Dimensional Model Reconstruction by Qi Chen, Jiyang Zou, Fusheng Wang, Kai Qiao, Han Li, Weiguo Zhang and Kang Tian in Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted March 29, 2023; accepted April 26, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by the National Natural Science Foundation of China (No. 81601901) and the Natural Science Foundation of Liaoning, China (No. 2019-MS-079). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from First Affiliated Hospital of Dalian Medical University (approval No. PJ-XJS-2022-83).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.