
Abstract
Background:
Upper extremity injuries account for approximately 16.9% of football injuries in the National Collegiate Athletic Association (NCAA).
Purpose:
To determine the epidemiology, management, and outcomes of hand/wrist injuries in collegiate football athletes so as to identify factors associated with surgical intervention and delayed return to play (RTP).
Study Design:
Descriptive epidemiology study.
Methods:
We retrospectively reviewed hand/wrist injuries that occurred within a single NCAA Division I football team from January 1, 2003, to December 31, 2020. Data analyzed included player position, college seniority, injury characteristics, injury management, surgical procedures performed, and timing of RTP. A univariate analysis was performed to identify factors associated with increased risk for surgical intervention and delayed (>21 days) RTP after hand and wrist injury in this cohort.
Results:
Overall, 124 patients with 168 hand/wrist injuries were identified (9.9 wrist/hand injuries per year). Sprain of the thumb metacarpophalangeal (MCP) joint ulnar collateral ligament (UCL) was the most common diagnosis (19.6%). Surgery was required in 22% of injuries, with injury of the UCL of the thumb MCP joint (8/37) being the most common indication. Injuries occurring during competitive games (odds ratio = 4.29; 95% CI, 1.2-15.9) were associated with an increased risk for surgery. Most (70%) injuries did not lead to time missed from football, whereas the remaining 30% resulted in an average of 33 ± 36 days missed.
Conclusion:
Over 17 athletic seasons, the annual incidence of hand and wrist injury in these NCAA Division I football players was 9.9 injuries per year, with 22% requiring surgical treatment. Injury to the UCL of the thumb MCP joint was the most common injury and indication for surgery, and 30% of injuries resulted in approximately 1 month lost. Injuries sustained in games were associated with operative management and delayed RTP.
According to the 2018-2019 National Collegiate Athletic Association (NCAA) sports participation report, a total of 73,712 male student-athletes competed in Divisions I, II, and III collegiate football in the United States. 12 Previous studies have demonstrated that 11% to 81% of collegiate football athletes will sustain an injury over the course of their careers. 1 The NCAA football injury report from 2004 to 2009 showed that upper limb injuries accounted for 16.9% of the approximately 41,000 injuries recorded over this 5-year period. 1
In a recent epidemiological study by Bartels et al 1 using the NCAA Injury Surveillance Program (ISP), the incidence of hand and wrist injuries was higher in games compared with practice (3.6 vs 0.51 injuries per 1000 athlete-exposures [AEs], respectively), and blocking was the most commonly reported mechanism of injury. These authors found that the mean time lost from such injuries ranged from 0 to 8.3 days; however, 48% of the recorded injuries resulted in no time missed. The rate of surgical intervention was 7.4%, and metacarpal fracture was the most common surgical indication. 1
Several studies have examined the type of hand and wrist injuries and treatment outcomes in professional football players; however, there is a paucity of granular clinical data on student athletes. 10,11,14,15 The majority of descriptive epidemiological studies analyzing hand and wrist injuries in collegiate football players use data from the NCAA ISP, which lacks clinical details including specific diagnoses, type, and duration of immobilization, and surgical procedures performed. 1,4,5,13 More detailed clinical data on the management and outcomes of hand and wrist injuries in collegiate football athletes are available mostly through small case series and case reports. 2,3,6,7,9,16,17 In addition, the risk factors for surgical intervention and those related to early or delayed time to return to play (RTP) have not been investigated.
The purpose of this study was to analyze a single institution’s athletics database to determine the epidemiology, management (operative and nonoperative), and outcomes of hand and wrist injuries in NCAA Division I football athletes. For injuries requiring surgical management, we sought to identify factors associated with increased risk of surgical intervention and delayed time to RTP. Our hypothesis was that the epidemiology of hand and wrist injuries in NCAA Division I athletes would follow patterns similar to previous reports using the NCAA ISP. We also hypothesized that certain player and/or injury characteristics would affect the possibility of needing surgical intervention as well as the time to RTP in these athletes.
Methods
Study Design
This was an institutional review board-approved retrospective review of wrist and hand injuries sustained by collegiate football players by a single NCAA Division I football team over a period of 17 athletic seasons. All injuries were retrieved from the institutional web-based data registry (Laserfiche Content Management System). Injuries during organized practices and official games from the first day of preseason to the final postseason competition between the 2003-2004 and 2019-2020 academic years were included. Injuries that were inadequately reported with incomplete data were excluded.
“Injury” was defined as an event that required immediate medical attention from the athletic trainer or physician. Wrist injury involved the distal radius, distal ulna, and carpal bones. All injuries involving the metacarpals and/or digits were classified as hand injuries. Data were recorded in the local database by the athletic trainers at the time of the event. RTP was defined as the duration from the time of injury to when the athlete returned to full competition and/or practiced without restrictions (if off-season). Time to RTP was further classified as delayed (>21 days) or nondelayed (≤21 days). Diagnosis for each injury was determined based on the clinical note by the attending physician and review of available imaging studies. Postoperative RTP information was gathered from physical therapy notes and physician clinic notes.
Obtained data included player position [defense (defensive back, defensive lineman, linebacker), offense (offensive lineman, running backs, and receivers, offense unspecified), special positions (kicking specialists, other special team positions, and unknown)], seniority in college (freshman, sophomore, junior, senior), injury laterality, mechanism of injury (blocking, tackling, catching, kicking, throwing, ground-level fall, contact with equipment, weightlifting, overuse, other unspecified contact, other unspecific noncontact), injury setting (game vs practice), injury characteristics (location, recorded diagnosis), treatment (operative and nonoperative), type and duration of upper extremity immobilization for nonoperative injuries (cast, splint, brace, tape), surgical procedures performed, and time to RTP.
Statistical Analysis
Analysis was performed with IBM SPSS Statistics software with the significance level set at P < .05. Demographic data were reported as means with standard deviations or number of players with percentages. A Shapiro-Wilk test was used to assess normality of the data before initiation of further analysis. Incidence rate of injury was reported as number of injuries per 1000 AE hours. Comparison of the RTP based on injury setting and player position was performed using a Mann-Whitney U test or Kruskal-Wallis test, as applicable. The chi-square test or Fisher exact test (if n ≤ 5) was used to compare categorical data. A univariate analysis was performed to identify factors associated with increased risk for surgical intervention and delayed time to RTP. Factors with a P value <.1 in the univariant analysis were included in the multivariant regression model to account for potential confounding between the cohorts. Finally, time to RTP was further classified as delayed (>21 days) or nondelayed (≤21 days). A univariate analysis was performed to identify potential risk factors for delayed (>21 days) RTP after injury to the hand and wrist in elite football players.
Results
During the 17 athletic seasons studied, a total of 124 NCAA Division I football athletes with 168 hand and wrist injuries were identified for inclusion. The annual rate of injury was 9.9 hand and wrist injuries per year, with 55% of injuries occurring during competitive matches and 41% occurring during practice (P = .07). The incidence rate of injury during practice was 1.2 injuries per 1000 AE hours, and the incidence rate of injury during competitive matches was 3.3 injuries per 1000 AE hours.
Injuries were documented for both practice sessions and official games. Table 1 presents a comparison of hand and wrist injuries recorded in practice versus games based on player (seniority and position) and injury characteristics (type, anatomic location). Seniors had the highest number of recorded injuries during both practices and games compared with the other classes of players. Sophomores had the lowest number of recorded hand and wrist injuries during games (5.8%), whereas juniors had the lowest number of recorded hand and wrist injuries during practice (15.2%). Offensive players had the highest number of recorded hand and wrist injuries during practice (57.6%) and competitive games (38.2%) compared with other player positions (P = .021).
Comparison of Hand and Wrist Injuries in Football Practices Versus Games Based on Player and Injury Characteristics (N = 168 Injuries) a
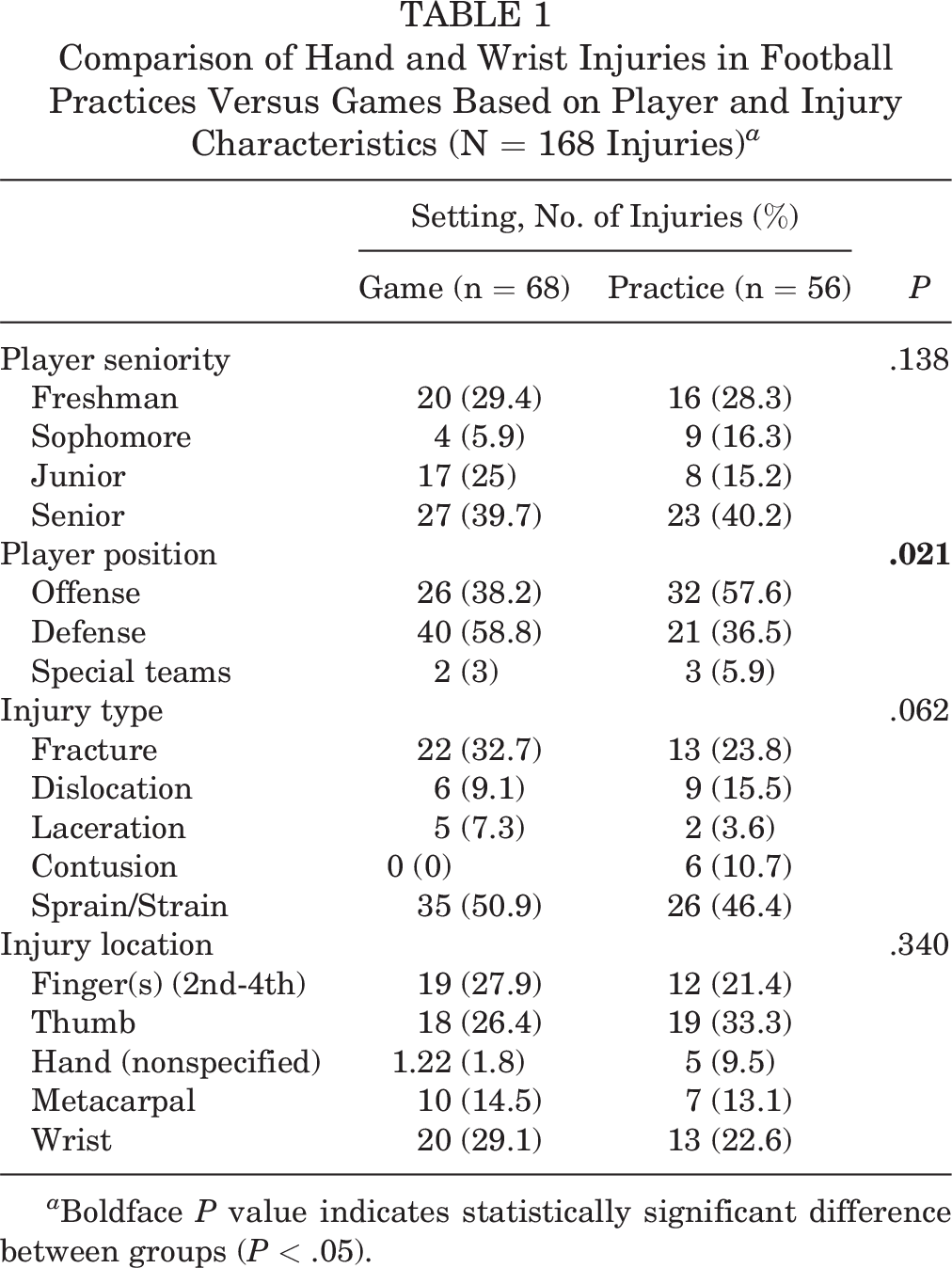
a Boldface P value indicates statistically significant difference between groups (P < .05).
The distribution of hand and wrist injuries based on player position is presented in Table 2. In the defensive player category, backs and receivers had the highest number of recorded hand and wrist injuries (50/168; 29.8%), followed by linebackers (32/168; 19%). The documentation of the mechanism of injury was unclear in 24% (41/168) of the recorded hand and wrist injuries. Among the 127 injuries with a known mechanism of hand and wrist injury, player on player contact was the most commonly recorded mechanism (36/127, 28.3%), followed by tackling (33/127, 26%) and blocking (28/127, 22%) (Table 3).
Hand and Wrist Injuries Based on Player Position (N = 168 Injuries)

a Kick returners, long snappers, holders, etc.
Hand and Wrist Injuries According to Recorded Mechanism (n = 125 Injuries)

Diagnosis, Management, and Risk Factors for Surgical Intervention
Sprain of the ulnar and/or radial collateral ligament of the thumb metacarpophalangeal (MCP) joint (33/168, 19.6%) was the most commonly reported injury, followed by fractures of the second to fifth metacarpal bones (20/168, 11.9%) and proximal interphalangeal joint dislocations (19/168, 11.3%). Table 4 presents the distribution of reported diagnoses in athletes with injuries to the hand or wrist. Of the 168 injuries, 131 (78%) were treated nonoperatively, while 37 (22%) of the injuries required surgery. The vast majority of nonoperative injuries (121/131, 92.4%) required some type of immobilization. For injuries that were managed nonoperatively, the most common immobilization modality was a removable plaster splint to the wrist or finger (49%), followed by short arm casts (30%), taping (17%), and soft braces (4%).
Distribution of Wrist and Hand Injury Diagnoses a

a MCP, metacarpophalangeal.
The most common indication for surgical intervention was injury of the ulnar collateral ligament of the thumb (8/37, 21.6%). Univariate analysis showed that hand and wrist injuries sustained during competitive games were more likely to require surgical intervention compared with injuries sustained in practice (P = .012, Table 5). Player grade level was also associated with surgical intervention, with sophomores needing surgery in 47.4% of cases as compared with 16.7% for freshmen, 23.5% for juniors, and 18.2% for seniors (Table 5). Multivariate analysis showed that injuries sustained during a competitive game were 4 times more likely to receive surgical intervention compared with practice sessions (odds ratio [OR] = 4.29; 95% CI, 1.2-15.9) (Table 6). Sophomores were 16 times more likely to require operative management as compared with freshmen (OR = 16.4; 95% CI, 2.3-116.4).
Univariate Analysis on Factors Associated With Higher Risk of Surgical Intervention a
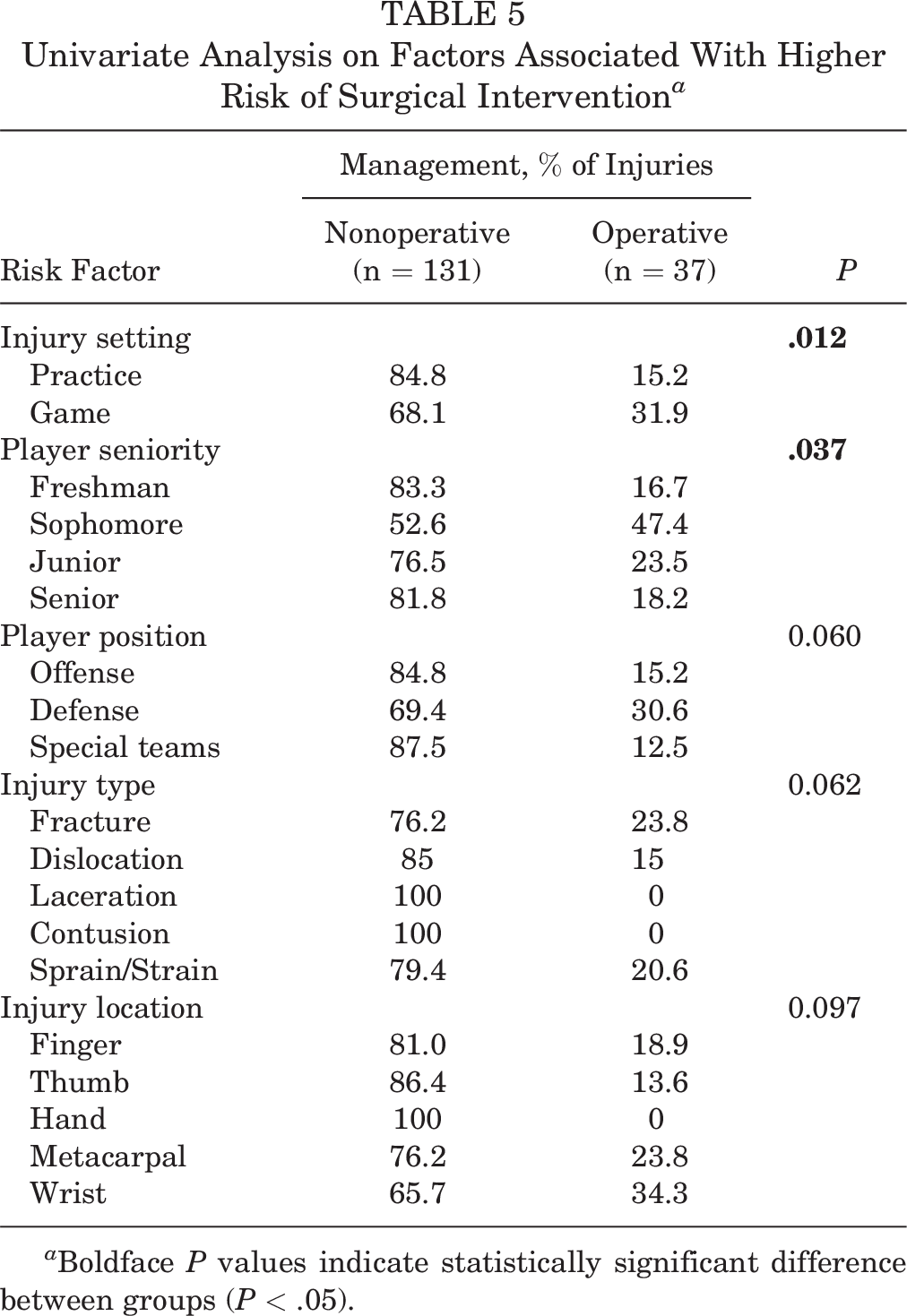
a Boldface P values indicate statistically significant difference between groups (P < .05).
Multivariate Logistic Regression Analysis of Factors Associated With Higher Risk of Surgical Intervention in Football Athletes Who Sustained Injuries to the Hand and Wrist a

a OR, odds ratio; Ref, reference. Boldface P values indicate statistical significance difference versus reference variable (P < .05).
RTP Time and Factors Associated with Delayed RTP
RTP information was available for 161/168 (96%) of the injuries. The RTP rate was 100% of these injuries; 70% of the recorded injuries were not associated with any time loss from football participation. For the remaining 30% of hand and wrist injuries, the mean time lost was 33 ± 36 days. The mean time loss was 2 ± 8 and 44 ± 39 days for nonoperative and operative injuries, respectively (Table 7). Hand and wrist injuries sustained by defensive players were associated with longer time for RTP compared with injuries sustained by offensive players (12 ± 25 vs 7 ± 23 days, respectively P = .035). No significant differences were noted with regard to RTP time and injury type (fracture, dislocation, sprain, etc) or location (hand vs wrist), although injuries to the metacarpals resulted in longer time missed from football compared with injuries in other anatomic regions of the distal upper extremity (13.4 ± 36 days, P = .073). Hand and wrist injuries sustained during matches (vs practice) were associated with delayed RTP (P = .01) (Table 7).
Hand and Wrist Injuries Managed Operatively and Associated RTP a

a RTP, return to play.
b Standard deviation was not reported due to limited number of patients included in each diagnosis category.
Discussion
The major findings of our study demonstrated an incidence of 9.9 hand and wrist injuries per year noted in this retrospective analysis of distal upper extremity injuries in NCAA Division I football athletes from a single institution over a period of 17 athletic seasons. A total of 168 hand and wrist injuries were analyzed in 124 athletes, with 55% of these injuries occurring during a competitive match. Sprain of the ulnar and/or radial collateral ligament of the thumb MCP joint was the most commonly recorded diagnosis, followed by fracture of the second to fifth metacarpal bones (20/168, 11.9%) and proximal interphalangeal joint dislocation (19/168, 11.3%). Of the 168 injuries, 37 (22%) required surgical intervention, with injury of the UCL of the thumb (8/37, 21.6%) being the most common indication.
Injuries occurring during competitive games and those occurring in sophomores were associated with an increased risk of surgery. All players were able to return to football with both operative and nonoperative injuries, and 70% of the hand and wrist injuries were not associated with any time missed from football participation. For the remaining 30%, the mean times missed from participation in football were 2 days for nonoperative and 44 days for operative injuries. No significant differences were noted with regard to RTP time by type or anatomic location of injury, but injuries to the metacarpals resulted in longer time missed compared with injuries in other anatomic locations of the distal upper extremity (13.4 ± 36 days, P = .073). Hand and wrist injuries sustained in competitive games (vs practice) were associated with delayed (>21 days) RTP (P = .01).
Previous studies have reported the epidemiology of hand and wrist injuries in NCAA football players. 1,2,5,13 Bartels et al 1 reported the epidemiology of hand and wrist injuries in collegiate football players over 5 athletic seasons (2009-2010 to 2013-2014), using data from the NCAA ISP. The authors reported a significantly higher incidence rate of hand and wrist injuries during competitive matches compared with practice (3.6 vs 0.51 injuries per 1000 AEs, respectively) in football players competing in all 3 NCAA Divisions. 1 In our cohort, we reported the incidence of hand and wrist injuries in NCAA Division I athletes only. The injury rate in the current study was reported as the number of injuries per 1000 hours of AE, unlike the study by Bartels et al, 1 who calculated the incidence rate of injury based on the number of hand and wrist injuries per 1000 AEs, thus making a direct comparison between the 2 studies challenging. Our study demonstrates a higher incidence rate of hand and wrist injuries during official games as compared with practice (3.3 vs 1.2 injuries per 1000 hours of AE) in NCAA Division I football athletes, which corroborated the findings of Bartels et al. 1 Discrepancies in the methodologies used to report the incidence rate of upper extremity or other injuries across the various sports precludes the possibility of combining the existing data to provide more accurate estimates of injury incidence rates and makes it difficult to draw conclusions on the necessity of implementing prevention protocols. 8
The incidence rate of hand and wrist injuries in collegiate football players was higher in Division I (0.61 injuries per 1000 AEs) compared with Division II (0.11 per 1000 AEs) and Division III categories (0.36 per 1000 AEs), based on previous studies. 1 The current study only included hand and wrist injuries sustained by NCAA Division I football players, and therefore, we were unable to examine whether the incidence rate varied according to the level of competition. More research is necessary to identify factors that may contribute to higher rates of hand and wrist injuries in Division I athletes compared with Division II and III players in collegiate football. 1
Based on our findings, the most commonly reported diagnosis of hand and wrist injuries in high-level football players were sprains of the ulnar and/or lateral collateral ligament of the thumb MCP joint, followed by fractures to the second to fifth metacarpal bones and proximal interphalangeal joint dislocations of the second to fifth fingers. In the study of Bartels et al, 1 wrist sprain/strains were the most commonly recorded injury followed by fractures and contusions. A key difference between institutional studies and studies using large data repositories (such as the NCAA ISP) is the level of detail. Although the NCAA ISP system provides large datasets of athletes and is ideal for the presentation of gross epidemiologic data, there is a lack of surgical data on collegiate athletes that can carry considerable clinical value in the field of sports medicine. For example, in a surgical case series of NCAA Division I football players who underwent surgical repair of thumb UCL, Bernstein et al 2 highlighted the risk of adjacent joint dislocation with the use of thumb spica casts for the protection of the surgical repair site. The authors suspected that the cast may act as a stress riser for adjacent joints contributing to joint dislocation during football participation. 2 In addition, the clinical course of musculoskeletal injuries, as well as the postoperative recovery and outcomes in young athletes may differ from that of an older athlete or a nonathlete undergoing the same type of procedure, which further highlights the value of data obtained from institutional studies.
A total of 22% of the recorded hand and wrist injuries in our study required surgical intervention, almost 3 times higher than the 7.4% reported by Bartels et al. 1 As shown in Table 4, thumb UCL injury was the most common indication for surgery in our cohort. In contrast, metacarpal fracture was the most common surgical indication in the study of Bartels et al. 1 With regard to management of ulnar collateral ligament injuries of the thumb in football athletes in our institution, injuries are evaluated acutely, and complete ligament avulsions are treated surgically. In nonthrowing athletes, complete injuries are commonly splinted during the season and operated on during the offseason. Surgery typically involves a direct ligament repair with the use of an internal brace. If performed during the season, RTP commonly occurs once soft tissue healing has been achieved. For metacarpal fractures, metacarpals that are amenable to stable internal fixation are fixed with anatomic reduction and an absolute stability construct. Implants are commonly a plate and screws or an intramedullary nail. RTP commonly occurs once soft tissue healing is complete and full motion is achieved, between 2 and 4 weeks.
Given the relatively long mean RTP time after UCL surgery in our cohort (46 days), surgeons can consider bracing the injury while the athlete is in season and pursue surgical management upon the season’s conclusion. Bartels et al 1 reported the time missed from football participation for the different hand and wrist injuries recorded but did not differentiate between athletes who had operative versus nonoperative management as well as the time missed for each specific injury diagnosis. Our data agreed, however, that approximately 70% of the recorded hand and wrist injuries resulted in no time lost from football. 1 Based on our results, the mean time lost for nonoperative injuries was 2 days and the mean time missed for operative injuries was 44 days (∼6 weeks). Table 7 shows the mean time to RTP based on the injury diagnosis. Aside from one athlete who had surgical repair of a perilunate dislocation, the mean time missed for other hand and wrist injuries that were managed operatively ranged from 25 to 67 days.
We sought to identify factors that were associated with a higher likelihood of undergoing surgery in football players with injuries to the hand and wrist. The findings support our hypothesis that hand and wrist injuries in NCAA Division I athletes follow patterns similar to previous reports, and that player and injury characteristics affect the possibility of needing surgical intervention and time to RTP. Based on our multivariate analysis model, injuries sustained during competitive games were 4 times more likely to necessitate surgical intervention than injuries sustained during practice. Although the clinical interpretation of the observed elevated risk of surgical intervention in sophomore football players with injuries to the hand and wrist is challenging, it is worth mentioning the lack of literature investigating the differences in musculoskeletal injury patterns among collegiate grade levels. Bartels et al 1 noted that freshmen sustained the highest number of hand and wrist injuries during practice and juniors during game, whereas we found that seniors had the highest number of recorded injuries in both practice and games.
Limitations
This study was limited by several factors, due mainly to its retrospective nature. The analysis of various surgical diagnoses and their clinical courses in this study is limited by the relatively low number of patients, similar to previous studies that used data from the NCAA ISP. 1 Larger datasets will allow for more accurate clinical observations and improve clinical practices in the management of collegiate athletes who undergo surgical treatment of musculoskeletal injuries. Although we analyzed a variety of hand and wrist injuries in football players, all the included athletes were male players who competed in the NCAA Division I category and these findings may not apply to female football athletes or those competing in high school, NCAA Division II and III, or professional categories. In addition, we were only able to analyze data from a single institution, which may influence treatment decisions based on provider preferences. We attempted to retrieve data related to the time and duration of distal upper extremity immobilization, physical therapy for hand and wrist injuries that were treated nonoperatively, and any modifications to the postoperative rehabilitation protocol; however, these data were available in <70% of the included athletes and further analysis was precluded. Improved documentation of the clinical course of nonoperative injuries can yield valuable information for clinicians regarding the necessity of immobilization and the optimal duration of immobilization.
Conclusion
This study provided data regarding expected RTP times based on injury and player parameters in a single NCAA Division I football team over 17 athletic seasons. The annual incidence of hand and wrist injury in Division I football players was 9.9 injuries per year with 22% of these injuries requiring surgical treatment. Injury to the UCL of the thumb MCP joint was the most common indication for surgery. The RTP rate was 100%, with 70% of hand and wrist injuries not associated with any time missed from football, whereas 30% of injuries resulted in approximately 1 month lost. Injuries sustained in competitive matches more often required operative management and were associated with delayed RTP (>21 days) versus those sustained in practice. Characteristics that were independently associated with the likelihood of requiring surgery after a hand or wrist injury were also identified.
Footnotes
Acknowledgment
The authors acknowledge The Cappo Family Research Fund.
Final revision submitted March 8, 2023; accepted April 24, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: L.T.N. has received education payments from Micromed and hospitality payments from Axogen. A.E.W. has received education payments from Arthrex, consulting fees from Stryker; and nonconsulting fees from Arthrex. J.E.T. has received nonconsulting fees from Arthrex and hospitality payments from Stryker. S.S. has received education payments, consulting fees, nonconsulting fees, and royalties from Arthrex. S.C.G. has received consulting fees from Exactech and Zimmer Biomet, nonconsulting fees from Arthrex, and royalties from Zimmer Biomet. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Southern California Health Science Campus (proposal No. HS-15-00063).