
Abstract
Background:
Few studies have evaluated the outcomes of posterior arthroscopic capsulolabral repair in adolescents, especially with regard to outcomes after revision repair.
Hypothesis:
Adolescent athletes who undergo revision arthroscopic posterior unidirectional capsulolabral repair will have similar outcomes and return to play when compared with adolescent athletes who underwent primary arthroscopic posterior unidirectional capsulolabral repair.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Data were reviewed from patients who underwent posterior shoulder stabilization between 2000 and 2019 and had a minimum follow-up of 2 years. Patients <11 and >19 years of age and those with multidirectional instability were excluded. Revision surgery was defined as repeat arthroscopic posterior capsular repair. The ability to return to sport (and level of sport), clinical outcomes scores (American Shoulder and Elbow Surgeons [ASES] and visual analog scale for pain), and patient-reported perception of range of motion, strength, and satisfaction were recorded. Comparisons between the primary and revision cohorts were made using the chi-square or the Mann-Whitney U test.
Results:
Included were 180 adolescent patients (182 shoulders) who underwent a primary unidirectional posterior stabilization, with an average follow-up of 6.1 years. Of these patients, 17 patients required revision surgery (9.3% revision rate). At the final follow-up, patients who underwent revision surgery returned to sport at similar rates to those who did not (70.6% vs 85.9%; P = .095) and were similarly likely to return to their presurgery level of play (41.1% vs 23.7%; P = .10). The no-revision patients had higher ASES scores (76.1 vs 87.1; P = .007) as well as less pain and improved subjective range of motion scores. However, both groups had similar subjective strength scores, and both reported that surgical repair was satisfactory (no revision, 93.2% vs revision, 88.2%; P = .45).
Conclusion:
Adolescent athletes had a low risk of revision surgery and frequently returned to play after arthroscopic posterior capsulolabral repair, often at a lower level of play. Those who required revision surgery had poorer outcome scores but still reported a high rate of satisfaction.
Posterior shoulder instability has become increasingly recognized as an important shoulder pathology, especially in contact and throwing athletes, with current studies suggesting that its prevalence may be higher than anterior instability. 1,2,14,23 Causes of posterior shoulder instability in the athlete include repeated microtrauma to the posterior capsulolabral complex, leading to capsule attenuation and associated labral tears, as well as trauma. 9,13,20 Previous meta-analyses have demonstrated that arthroscopic posterior capsulolabral repair with suture anchors is an effective treatment for athletes, with the rate of recurrent instability reported at 8.1% (range, 0%-25%). Further, improved outcome scores have been reported and overall rates of return to play (RTP) are high at 91.81%. 12,22
Outcomes of posterior stabilization in the adolescent population is of high interest due to a documented higher failure rate than reported in previous studies that combined the adolescent and adult groups. 6,7,17 This may mirror the outcomes from the anterior shoulder instability literature, where it is known that adolescent athletes have a higher risk of recurrent instability after labral stabilization. This is possibly due to their higher physical demand and activity level when compared with the adult cohorts. 18,19,21 Currently, there is only one previous case series of 48 adolescents that aimed to identify risk factors for revision posterior shoulder stabilization in this younger cohort. The authors found that female sex, younger age, and traumatic presentation all led to increased risk of failure in this population. 3
Bradley et al 7 reported that a cohort of both adult and adolescent contact athletes who underwent revision posterior shoulder stabilization returned to sport less frequently than those who only underwent a primary posterior shoulder stabilization and that those who were able to return to sport did so at a lower level. In the current study, we aimed to further elucidate the outcomes of revision posterior shoulder stabilization in the adolescent athlete. We hypothesized that these patients will have outcomes similar to adolescent patients who only required a primary stabilization procedure.
Methods
Patient Selection and Evaluation
Institutional review board approval and informed consent were obtained before initiation of the study. Patient data for patients undergoing arthroscopic posterior shoulder stabilization between 2000 and 2019 were compiled into a database. Any patients identified with multidirectional instability via a positive sulcus test that does not correct with external rotation were excluded from the database. Patients who had scapular dyskinesis as defined by Kibler and Sciascia 15 were also excluded.
Inclusion criteria for this study were adolescent athletes who underwent surgical intervention for unidirectional posterior shoulder stabilization between 2000 and 2019 and had a minimum of 2-year follow-up, timed from date of surgery. Patients <11 and >19 years of age were excluded. All patients included in this study had a failed course of preoperative physical therapy for strengthening and motion. The timing of surgery was based on patient preference, sport, level of competition, and desire to return to competitive athletics.
Operative Procedure
Patients who had history, physical examination, and advanced imaging consistent with isolated posterior shoulder instability and a failed course of nonoperative treatment were selected for surgery. All procedures were performed by the senior author (J.P.B.).
Before each operation, an examination under anesthesia was performed. Patients underwent a dynamic stability examination before the start of surgery and the sulcus test was repeated. At the start of each operative procedure, a diagnostic arthroscopy was performed to identify pathology within the posterior capsulolabral complex. This included capsular laxity, capsular tears, labral fraying, labral tears, as well as any bony injury. In addition, the size of the capsulolabral pathology was normalized to clockface hours. The procedure was then tailored to the specific injury pattern, and 1 of 3 procedures was performed: (1) capsulolabral plication without suture anchors, (2) capsulolabral plication with suture anchors, or (3) capsulolabral plication with suture anchors and additional plication sutures. 8 In revision cases, the labrum was elevated and knotless fixation was utilized, with upsized anchors after overdrilling the anchors from their previous surgery.
Patients underwent physical therapy postoperatively, with RTP typically at 6 months as described previously. 9,17
Outcome Evaluation
Patient data were reviewed retrospectively by blinded authors (E.A.W., J.W.A.). Patient age, sex, sport, position, type of sport, physical examination, level of competition, length of follow-up, return to sport, and level of return were recorded. Physical examination at the time of initial evaluation included quantification of active and passive range of motion (ROM), tenderness to palpating, strength testing, and instability testing. Posterior instability testing included the Kim test, the jerk test, the posterior load and shift test, and the posterior stress test. 10 Standard magnetic resonance imaging (MRI) was performed on all patients to aid in the evaluation and diagnosis of capsulolabral pathology. Intraoperative findings and surgical repair constructs were also recorded for each patient. Finally, patient satisfaction with the surgery, either the primary procedure or the secondary procedure for revision cases, was recorded.
Outcome Scores
Patient outcome scores were collected preoperatively and at the latest follow-up using REDCap, hosted by the University of Pittsburgh Medical Center. According to University of Pittsburgh Medical Center protocol, patients were contacted by letter, email and then a telephone call. Equal weight is given to the cumulative activity of daily living (ADL) score and the amount of pain reported by the patient. In addition, subjective, patient-described ROM (graded from 0 to 3: 0 = poor, 1 = limited, 2 = satisfactory, 3 = full) and strength (graded from 0 to 3: 0 = none, 1 = markedly decreased, 2 = slightly decreased, 3 = normal) were obtained at the latest follow-up.
MRI Measurements
MRI measurements of glenoid bone width, labral width, cartilage version, labral version, and glenoid version were performed at index assessment as described previously by Mauro et al. 16 Labral width and labral version were calculated as described previously. 7,16 These measurements were compared between the adolescent athletes who only underwent a primary surgery and those who underwent a revision surgery.
Statistical Analysis
Patients within this cohort who underwent revision and those who only had a primary stabilization were compared. Statistical analysis was completed using Student t test for scaled data, the chi-square test for nominal data, or the Mann-Whitney U test for ordinal and nonparametric data. Statistical significance was set at P < .05. All statistical analysis was completed using IBM SPSS statiststical software (Version 27.0, IBM Armock, NY).
Results
Patient Characteristics
Of 718 initial patients who were reviewed, 180 patients (182 shoulders) met the inclusion criteria. The additional 538 patients were outside of our age parameters or had evidence of multidirectional instability. Of the 182 included shoulders, 17 subsequently underwent revision surgery, for an overall revision rate of 9.3% at overall mean follow-up time of 74.2 months. The age of the patients was comparable in each group, though there were significantly more females in the revision group (P = .002). Patient characteristics, intraoperative findings, and level of sport are listed in Table 1. The primary sport at the time of surgery is listed in Table 2.
Patient Demographics and Intraoperative Findings a
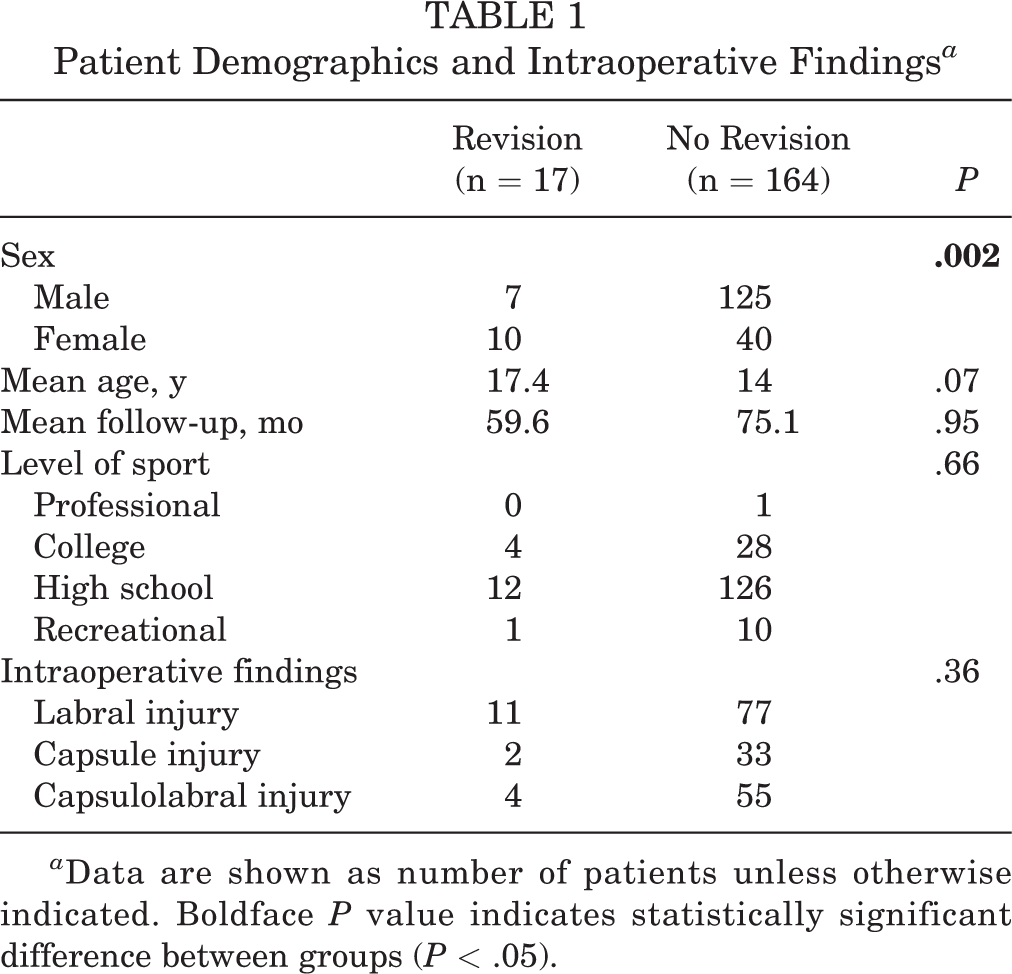
a Data are shown as number of patients unless otherwise indicated. Boldface P value indicates statistically significant difference between groups (P < .05).
Primary Sport at Time of Injury a

a Data are shown as number of patients.
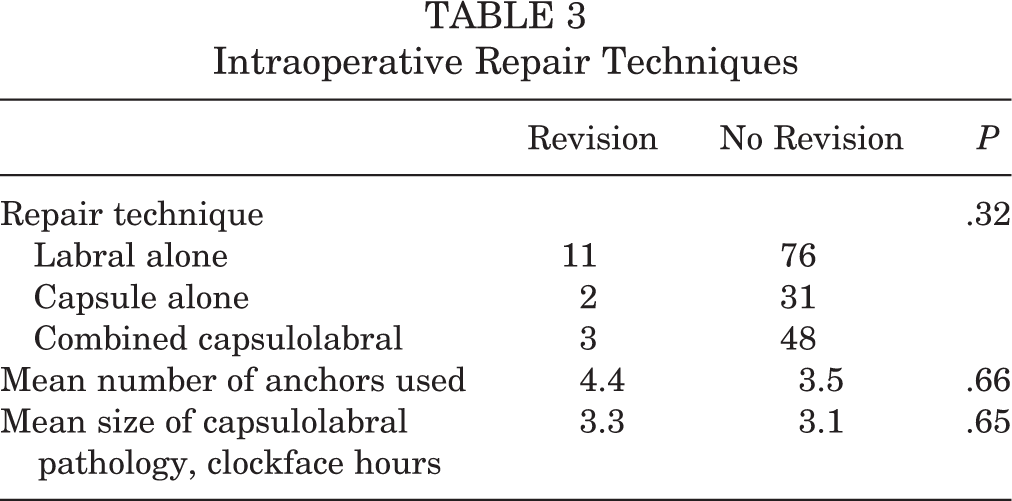
Repair techniques during the primary repair for the no-revision cohort and during the secondary repair for the revision cohort as well as number of anchors and size of the capsulolabral pathology are listed in Table 3.
Intraoperative Repair Techniques
Outcome Scores
Patients in both study groups saw significant improvement in American Shoulder and Elbow Surgeons (ASES) scores after surgical intervention. Although there was no difference in preoperative ASES scores between the groups, the no-revision patients had a significantly higher ASES score at most recent follow-up (P = .007). Patients who underwent revision surgery had significantly higher visual analog scale (VAS) pain scores (P = .01) as well as decreased ROM (P = .03). However, perceived strength was similar in both groups (Table 4).
Patient Outcome Scores a

a Boldface P values indicate statistically significant difference between groups (P < .05). Abbreviations: ASES, American Shoulder and Elbow Surgeons; Preop, preoperative; Postop, postoperative; ROM, range of motion; VAS, visual analog scale.
MRI Findings
MRI measurements of glenoid bone width, labral width, cartilage version, labral version, and glenoid bone version are compared in Table 5. None of the parameters measured or calculated were found to be significantly different between the revision and no-revision groups.
Glenohumeral MRI Measurements a

a MRI, magnetic resonance imaging.
Return to Sport
Table 6 presents the rates of return to sport and the subjective determination of satisfaction following either the primary procedure or the secondary procedure in the revision group. Both groups were able to RTP, and they returned at the same level at a similar, though relatively poor, rate.
Return-to-Play and Satisfaction Rates

Discussion
In the current study, adolescent patients underwent revision arthroscopic posterior capsulolabral repair at a rate of 9.3%. The cohort of patients who underwent revision posterior shoulder stabilization had significant improvements in their postoperative outcomes scores as compared with their index scores, though they were lower than those of the primary cohort. The revision patients reported increased pain scores and decreased ROM compared with those who did not undergo revision; however, they were able to RTP at a comparable level to those who had a primary posterior stabilization surgery and were similarly satisfied with their outcomes.
Much of the current literature regarding posterior shoulder instability does not isolate the adolescent population from the adult population. 6 –9,12 Adolescents represent a unique cohort due to their high frequency of sports participation, with many athletes playing multiple sports year-round. Currently, there are 3 studies that specifically analyzed the adolescent population, though each of these focused on either outcomes of or risk factors for failure of a primary repair. 3,17,25 As determined in this study, both Wooten et al 25 and Asturias et al 3 found that female sex is a risk factor for failure of primary arthroscopic capsulolabral repair in adolescence. While we did not report scores of generalized laxity in our cohort, adolescent female athletes are known to have higher rates of laxity than their male counterparts and have been shown to have higher rates of revision in another study. 24 In addition, in our cohort, there were sex differences with respect to participation in sports. Cheerleaders were female and had a 43% revision rate, whereas football players were male and only had a 4.9% revision rate. It is unclear if the difference in revision rates was due to the sex differences in participation or the sport itself.
Currently, no studies have determined the outcomes of adolescent patients that require revision posterior shoulder stabilization. In this study, adolescent athletes who underwent revision posterior shoulder had satisfactory outcome scores. This is similar to the previously reported outcomes of adolescents undergoing a primary posterior capsulolabral repair, as well as being comparable to this study’s primary revision cohort. 17 In addition, these outcomes are comparable to those reported in a recent study that included a mix of both adolescents and adults. Bradley and colleagues found that patients who underwent revision posterior capsulolabral repair had postoperative ASES scores that, while improved from their preoperative score, were significantly lower than those of patients who did not have failed primary repair. 6 This was also found in the current study but may be confounded due to adolescent athletes aging out of sports as they graduated high school. However, high levels of return to sport, although at a lower level than before surgery, and satisfaction with surgery was seen.
In this adolescent cohort, there was an overall revision rate of 9.3%. This rate is similar to rates previously reported for the adolescent population in the literature (range, 8.5%-12.5%). 3,17 Adolescent athletes have been shown to have a high risk of recurrent instability in the anterior stabilization literature, likely due to their higher activity level and physical demands. 5,11 This higher risk is possibly mirrored in the posterior instability literature, as a 2015 meta-analysis by Delong et al found a 6.18% recurrence rate in their review of 178 shoulders from 6 studies in patients of all ages. 12 Thus, adolescents may undergo revision posterior capsulolabral repair at slightly higher, though comparable, rates to those of their adult counterparts.
Both the revision and no-revision groups in the current study were able to RTP at high rates. In a meta-analysis of patients who underwent unidirectional posterior instability, DeLong et al 12 found that 89% of athletes were able to RTP at any level and 72% were able to return at the same level. However, a 2018 study by Bradley et al demonstrated that only 15.4% of nonthrowing athletes that underwent revision surgery were able to RTP at the same level, though 61.6% of the revision group were able to RTP at any level. 7 The current study’s adolescent revision cohort followed the same trend, in that while 71% were able to RTP, only 41% of patients were able to RTP at the same level. This finding was not significantly different than the RTP rates of the primary cohort in which only 1 in 4 patients returned to play at the same level. This adolescent revision cohort came from a multitude of different sports, including throwing and overhead sports, and while the athletes all identified a primary sport, many were multisport athletes. This creates a unique challenge for the operating surgeon, as the intraoperative goals for a throwing athlete may be different from those of a contact athlete regarding balancing soft tissue stability and laxity. It is also important to note that in the adolescent cohort, return to sport could also be due to other factors, such as high school graduation or a change in sport.
MRI measurements of a smaller glenoid bone width and a higher labral width weight for bone have been identified as risk factors for revision posterior capsulolabral surgery in previous studies. 6,16 However, in this study, none of the parameters measured were significantly different. Our revision cohort did trend toward a smaller anterior to posterior glenoid bone width, associated with increased percentage of bone loss, though this was not statistically significant. 4 While this study’s revision group was larger than that previous study (17 vs 8 shoulders), revision surgery was still relatively rare. 6 Further evaluation with a larger number of revisions would provide greater power.
In the current study, 88.2% of the revision group considered their surgery worthwhile, which was not significantly lower than the no-revision group (93.2%). In a 2018 study in which Bradley et al evaluated 297 nonthrowing athletes, 15.8% of their revision group were not satisfied with their primary posterior capsulolabral repair whereas 100% of their no-revision cohort were satisfied. 7 This is similar to the lower rate of satisfaction with the primary surgery in their revision group that Bradley et al 6 found in their 2020 study of contact athletes. In the current study, adolescent athletes reported high rates of satisfaction with their revision surgery, suggesting that even if the primary surgery fails, revision surgery is worthwhile and will produce favorable outcomes.
Limitations
Limitations of this study include subjective scoring systems, such as ASES and VAS, which may underestimate the true outcomes of athletes. This may be particularly the case in this young adolescent group. Other validated scoring systems, such as the Disabilities of the Arm, Shoulder and Hand and Single Assessment Numeric Evaluation were not included as the data collection for this cohort began in the 2000s, before these were validated. In addition, since the data do date back to the early 2000s, some parameters, such as microtrauma to the shoulder, as well as scores of generalized laxities, were unable to be collected. Revision was also our main measure of failure and may not capture those patients with recurrent instability who did not undergo a revision surgery. In addition, there were no formal clinical examinations at final evaluation, so strength and ROM parameters were self-reported. Unfortunately, a validated posterior shoulder specific scoring system for evaluation of athletes does not currently exist, making optimal evaluation of these athletes difficult. In addition, while a patient population of 182 is large for a single surgeon, it only yielded 17 revisions for analysis, making type II error possible, especially for RTP rates and subjective strength. Thus, a larger, multicenter patient population may improve the current study, especially regarding the MRI measurements.
Conclusion
At a minimum follow-up of 2 years, adolescent athletes underwent revision arthroscopic posterior capsulolabral repair at an incidence of 9.3%. The cohort that did undergo revision arthroscopic posterior capsulolabral repair, despite having lower outcome scores at the final follow-up, were able to RTP at a similar rate to patients who did not have a secondary procedure, and all patients reported a high rate of satisfaction with their surgery.
Footnotes
Final revision submitted March 26, 2023; accepted April 14, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.W.A. has received grant support from Arthrex and DJO and hospitality payments from Arthrex and Smith & Nephew. J.P.B. has received consulting fees from Arthrex and DJO and hospitality payments from Inspire Medical Systems. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from University of Pittsburgh (no. PRO12100277).