
Abstract
Background:
The timing of clinical evaluation after pediatric concussion represents an important and potentially modifiable clinical milestone for diagnosis, selection of appropriate treatment pathways, and recovery prognosis. Patient demographics, socioeconomic status, or medical history may affect the time to the initial evaluation and subsequently influence recovery outcomes.
Purpose/Hypothesis:
The purpose of this investigation was to evaluate the association of patient characteristics with the time to specialty evaluation after a concussion. It was hypothesized that patients with a history of concussion, a preexisting relationship with our specialty concussion program, or a higher ZIP code–based income estimate would present for care more quickly after a concussion than patients without these characteristics.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Included were patients with a concussion between 6 and 18 years old who were seen for care at a single sports medicine center between January 1 and December 31, 2019. Patient demographic, socioeconomic, injury, and clinical characteristics were collected through a retrospective review of the medical records. The primary outcome was the number of days between the date of the concussion and the patient’s initial specialty evaluation.
Results:
Overall, 220 patients (mean age, 14.4 ± 2.5 years; 46% female) were seen for care at a mean of 9.7 ± 5.6 days (range, 1-21 days) after concussion. A shorter time to specialty evaluation was associated with a history of concussion (β = –1.72 [95% CI, –3.24 to –0.20]; P = .03) and a prior clinical relationship with the treating clinical department (β = –1.85 [95% CI, –3.52 to –0.19]; P = .03). Referral by a primary care provider was associated with a longer time to evaluation (β = 3.86 [95% CI, 2.39-5.33]; P < .0001).
Conclusion:
A history of concussion and having a preexisting clinical relationship with the deparment were associated with a shorter time to evaluation after concussion. Referral from a primary care physician was associated with a longer time to evaluation. Issues may exist in the propensity to access care after an injury, resulting in delays for initiating early treatment.
A concussion results in pathophysiological disturbances, leading to a variety of symptoms and functional deficits. 11,19 The heterogeneous nature of concussion symptoms and functional impairments can create challenges for clinicians diagnosing, treating, and otherwise managing patients with concussions. 11 It is recommended that patients with a suspected concussion seek care from physicians or other health care professionals with appropriate training, education, and experience soon after the injury. 11 In particular, patients presenting to specialized concussion care centers >7 days after a concussion are at an increased risk of prolonged symptom duration and delayed return to sports. 2,3,7,16,24 Although other factors, such as acute symptom severity, also influence the time to symptom resolution, 13,20 the timing of initial care after a concussion represents a potentially modifiable factor that may influence patient outcomes.
Earlier initiation of treatment by qualified clinicians may contribute to a faster recovery time. 7,9,16 Rehabilitative interventions, including subsymptom threshold aerobic exercise, 18,29 may similarly reduce symptom duration when initiated ≤1 week after a concussion, 17 particularly among those at an increased risk of persistent symptoms. 12 Previous work in adolescents has suggested that each 1-day delay in the initiation of physical activity after a concussion is associated with a progressively smaller likelihood of returning to sports at the same time as patients initiating physical activity on the first day after a concussion. 17 Further, symptom provocation, physiological impairments, and symptom cutoffs for differentiating patients with concussions from healthy controls may differ among those presenting within 7 days of a concussion and those presenting later during recovery, suggesting that patient presentation and subsequent diagnosis and management may be affected by the timing of an evaluation. 8,15 Therefore, the time between the injury and initial evaluation remains an important clinical milestone for diagnosis, the selection of appropriate treatment pathways, and recovery prognosis.
At present, limited research has explored demographic or socioeconomic factors that influence the time to an evaluation among pediatric and adolescent patients with concussions. Previous research has suggested that patients with public insurance or those reporting Hispanic ethnicity may experience difficulties accessing specialized care after a concussion compared to care for other orthopaedic conditions. 5 Similar race-based disparities have been identified in concussion knowledge and symptom recognition 26,27 but not time to a specialty concussion evaluation. 28 Other research has identified sex and injury mechanism (sports vs nonsports injury) as potentially modifying factors in access to care after a concussion, 6,15 although additional research is needed to determine the relationship of these factors and others with time to a specialty evaluation. As such, the investigation of race, ethnicity, and sex is pertinent to our understanding of demographic factors that affect time to an evaluation after a pediatric concussion.
The primary aim of this study was to evaluate patient demographic, socioeconomic, and injury characteristics that may influence the time to a specialty evaluation at a single sports medicine center. Secondarily, we sought a more comprehensive understanding of how these barriers specifically influence the time between the injury and appointment scheduling (ie, propensity to access care) versus the time from appointment scheduling to evaluation (ie, barriers to accessing care after scheduling). We hypothesized that (1) patients with a history of concussion would present sooner after an injury and this shortened time to presentation would be primarily attributed to a reduced time from the injury to appointment scheduling compared to patients without a history of concussion; (2) patients with a prior relationship with our concussion program would both schedule and be evaluated more quickly after a concussion than patients with no prior relationship; and (3) patients living in ZIP codes with a mean household income below the state average would present for care later after a concussion than patients living in ZIP codes with a mean household income above the state average.
Methods
We conducted a retrospective chart review of patients seen for care at a single sports medicine center between January 1 and December 31, 2019. Pediatric patients with a suspected concussion, regardless of the injury mechanism (ie, sports or nonsports injury), were referred for specialty care by local primary care providers, urgent care/emergency departments, athletic trainers working in metropolitan high schools or sports clubs, or through self-referral. The sports medicine center at which patients were seen uses a specialty-based service delivery model, employing a multidisciplinary team of sports medicine physicians and athletic trainers. 25 The sports medicine center has clinics at approximately 7 locations throughout the greater metropolitan area in which study participation took place and is part of a larger regional tertiary care pediatric children’s hospital.
Study inclusion criteria consisted of being 6 to 18 years of age at the time of the evaluation, being diagnosed with a concussion, and undergoing an initial specialty evaluation within 21 days of the injury. Patients were excluded if they demonstrated positive findings on neuroimaging (intracranial hemorrhage, structural abnormality, etc) if performed, presented with a concomitant musculoskeletal injury, or sustained a second head injury before full recovery from their current concussion. The diagnosis was confirmed by board-certified pediatric sports medicine physicians and consistent with concussion guidelines at the time of the specialty evaluation. 11,19 Clinical evaluations consisted of patient-reported measures, physical examinations, and assessments of functional performance, including evaluations of cognition and postural stability, to determine the diagnosis. 19 The local institutional review board approved the study protocol, and all included patients and their parent/guardian provided informed assent or consent, as appropriate.
Primary Outcomes
The primary outcome of interest was the number of days between the concussion and initial clinical visit to the sports medicine center (represented as “time to specialty evaluation”). A visit with a health care professional not part of the sports medicine center (eg, primary care provider, emergency department, urgent care, or other medical care for concussions) was not factored into this calculation, as these data were not available to the study team and could not be accurately assessed. Thus, time to the specialty evaluation was a measure of the days between the injury and initiation of treatment in our concussion specialty program, notwithstanding prior evaluations that may have occurred elsewhere.
Similarly, we examined the time from injury to evaluation in 2 ways. We defined “time from injury to scheduling” as the number of days from the date of the concussion to the date on which a parent or guardian first contacted the clinic to schedule a specialty evaluation. Then, we defined “time from scheduling to presentation” as the time between appointment scheduling and the initial specialty evaluation. Thus, for our secondary aim, we sought to disentangle the patient’s propensity to access care (time from injury to scheduling) from barriers that exist in accessing care (time from scheduling to specialty evaluation).
Independent Variables
A range of demographic and injury characteristics were assessed. Patients reported their sex; race; ethnicity; and history of concussion, learning disabilities, sleep problems, and migraines. Injury characteristics, such as loss of consciousness at the time of the concussion and the setting of injury (competition or practice), were also recorded as part of clinical care.
To evaluate the influence of socioeconomic status on accessing care after a concussion, we included insurance type, parent education level, and income estimate. Insurance type was self-reported and categorized as either public or private insurance. The highest level of completed education was collected for each parent, with response options ranging from “some high school without degree” through “doctoral degree.” For analysis, parent education level was grouped as neither parent having completed at least a bachelor’s degree or ≥1 parent having completed at least a bachelor’s degree, mirroring the United States National Institutes of Health guidance on populations underrepresented in sciences. 21 If education level was reported for only 1 parent, then that parent’s educational attainment was used for grouping. To understand patient/family affluence, income tax statistics via the United States Internal Revenue Service website (IRS.gov) were used, consistent with methods utilized in prior research. 1 These publicly available data describe the mean income reported on tax returns for the year 2019, separated by ZIP code. The patient’s home ZIP code was used to determine the mean reported income per tax return for the patient’s community during the year of the study.
To evaluate other factors that may influence access to care, the date of the initial specialty evaluation was categorized as December to February (winter), March to May (spring), June to August (summer), and September to November (fall), in alignment with the typical academic and athletic calendar of our pediatric and adolescent population. Additionally, the distance between the patient’s home ZIP code and the clinic at which they were seen for the initial specialty evaluation was measured in miles. We also categorized the patient's preexisting clinical relationship as: with the hospital system, with the orthopaedics department, or with the specialty concussion program. Before their initial specialty evaluation, patients who recorded an appointment with the pediatric hospital for another injury or condition were considered a patient with a previous visit to the hospital system. Patients seen for care by the sports medicine or orthopaedic clinic (ie, orthopaedics department) for any previous injury or condition were categorized as having a preexisting relationship with the orthopaedics department. Patients with a visit to the sports medicine concussion clinic for treatment of a previous concussion were categorized as having a prior clinical relationship with the concussion program. All patients characterized as having a prior clinical relationship with the concussion program would necessarily have a history of concussions, as establishing care with the program requires prior treatment for a suspected head injury.
Patients reported their symptom burden on the day of the specialty evaluation using the Health and Behavior Inventory (HBI). The HBI is a 20-item self-reported instrument of concussion symptoms commonly used in care after concussions. 10,23 During the clinical visit, patients rated each concussion symptom from 0 (“never”) to 3 (“often”) for a maximum score of 60. The parent or legal guardian attending the visit also completed the parent version of the HBI, reporting his or her perception of their child’s symptoms. For patients aged >7 years, both the patient and parent HBI forms were completed and evaluated in this study. Patients aged ≤7 years did not complete the patient version of the HBI, and thus, only the parent forms were evaluated. 22
Statistical Analysis
The homogeneity of our cohort’s racial characteristics resulted in inadequate sample sizes to test a hypothesis that the primary outcome differed according to the independent variable of race. Thus, racial characteristics were not formally tested and are provided descriptively.
For our primary aim, we assessed the relationship between the time to specialty evaluation and patient demographic, socioeconomic, injury, and clinical characteristics. Independent-samples t tests were used to compare the time to specialty evaluation among binary variables, one-way analyses of variance were used for categorical variables with >2 levels, and Pearson correlation coefficients were used for continuous variables. A multivariable linear regression model was then constructed to assess factors that were associated with the time to specialty evaluation. An alpha level of .10 on univariable analysis was used to identify variables to include in the multivariable model. Statistical significance in the multivariable model was indicated at an alpha level of .05. Inference was drawn from the results of the multivariable model, with univariable analysis conducted for the purpose of model building.
To address our secondary aim, we included only the significant variables from the first multivariable model (α < .05) and used independent-samples t tests to compare variable levels among 2 primary outcomes: time from the concussion to scheduling and time from scheduling to the specialty evaluation. An alpha level of .05 was used to determine significance in this secondary analysis.
Data are reported as the mean and standard deviation for categorical variables and the correlation coefficient with corresponding P value for continuous variables. For categorical variables, the mean difference and 95% confidence interval are provided where appropriate. All statistical tests were 2-sided and performed using Stata statistical software (Version 16; StataCorp).
Results
A total of 286 patients with a suspected concussion were seen for care at our sports medicine center in 2019, of which 220 (mean age, 14.4 ± 2.5 years; 46% female) met inclusion criteria. Patients were excluded for a nonconcussion diagnosis (n = 22), being younger than 6 years (n = 1), being seen >21 days after the concussion (n = 34), demonstrating abnormalities on neuroimaging (n = 4), or sustaining a second head injury before full recovery from the current concussion (n = 5). Across the sample of included patients, the mean time from the injury to specialty evaluation was 9.7 ± 5.6 days (range, 1-21 days). The mean time from the injury to scheduling was 7.2 ± 5.0 days, and the mean time from scheduling to the specialty evaluation was 2.6 ± 2.3 days.
On univariable analysis, time to the specialty evaluation was not significantly associated with age; sex; or a history of learning disabilities, sleep problems, or migraines (Table 1). A history of concussion was associated with a shorter time to presentation, such that patients with a history of concussion were seen approximately 1.5 days sooner after the injury than those experiencing their first lifetime concussion (Table 1). Patients reporting American Indian/Alaskan Native race demonstrated a quicker time to specialty evaluation after a concussion (Table 1), although a small sample size prevented statistical testing from being performed for this variable. Patient ethnicity was not significantly associated with time to the specialty evaluation on univariable analysis (Table 1).
Time to Specialty Evaluation According to Demographic Characteristics a

a Boldface P value indicates statistical significance (P < .05).Dashes indicate no p-value provided due to small sample sizes.
Among socioeconomic factors, insurance type (private vs public) and ZIP code–based income estimate (below vs above state average) were not associated with time to specialty evaluation (Table 2), while a lower parent education level was associated with a marginally longer time to evaluation and met criteria for inclusion in the multivariable model (Table 2). Injury characteristics, including loss of consciousness and setting of injury (practice vs competition), were not associated with the time to evaluation (Table 2).
Time to Specialty Evaluation According to Socioeconomic and Injury Characteristics a
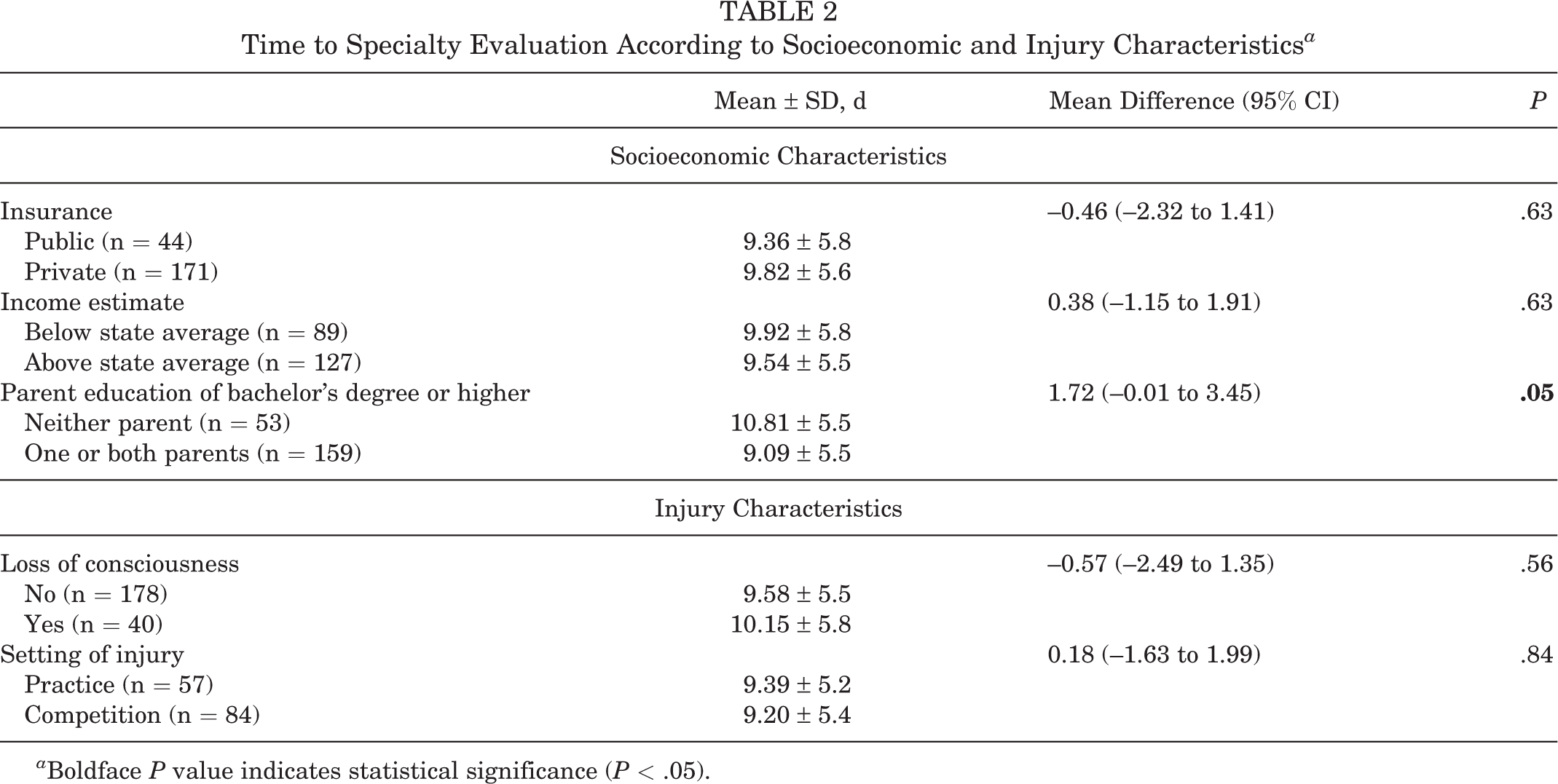
a Boldface P value indicates statistical significance (P < .05).
Patients referred to specialty care by a primary care provider were seen later after a concussion than patients referred from other sources (Table 3). The time of year was associated with time to clinical presentation in this patient sample, such that patients being seen for care in the spring presented earlier than patients seen during the fall (Table 3). Lastly, patients were seen sooner after a concussion if they had a preexisting clinical relationship with the hospital system, orthopaedics department, or concussion program (Table 3). The distance between a patient’s home and the location of the visit was positively and significantly associated with time to presentation, such that patients living further from the visit location were evaluated later after a concussion (Table 4).
Time to Specialty Evaluation According to Clinical Characteristics a

a Boldface P values indicate statistical significance (P < .05). Dashes indicate not applicable.
Association of Demographic, Socioeconomic, Injury, and Clinical Characteristics With Time to Specialty Evaluation a

a Boldface P value indicates statistical significance (P < .05). HBI, Health and Behavior Inventory.
Results from the multivariable model indicated that a longer time to the specialty evaluation was significantly associated with referral from a primary care provider and that a shorter time to the specialty evaluation was associated with a history of concussion and a previous visit to the orthopaedics department (Table 5).
Factors Predicting Time to Specialty Evaluation a

a Negative beta coefficients indicate a shorter time between the injury and specialty evaluation. Boldface P values indicate statistical significance (P < .05). R 2 = 0.24.
b Reference group was time of year: September-November (fall).
On secondary analysis, a history of concussion and a preexisting relationship with the orthopaedics department were associated with a shorter time from the injury to scheduling, while referral from a primary care provider was associated with a longer time from the injury to scheduling (Figure 1).

The relationship between 3 variables predictive of the time to the specialty evaluation, separated into the mean time from the injury to scheduling (dark bars) and the mean time from scheduling to the initial specialty evaluation (light bars). Error bars indicate 95% CIs. P values represent individual comparisons for time from the injury to appointment scheduling and time from scheduling to the initial specialty evaluation.
Discussion
A faster time to specialty evaluation for concussion at a sports medicine center was associated with having a history of concussion and a preexisting clinical relationship with our orthopaedics department, while a longer time to specialty evaluation was associated with referral by a primary care provider. We observed that a history of concussion, prior clinical relationship, and referral source were factors associated with the propensity to access care (ie, time to scheduling), while none of the factors studied were identified as barriers to accessing care after scheduling (ie, time from scheduling to the specialty evaluation). Similarly, a majority of the time between the injury and specialty evaluation was spent without an appointment scheduled, indicating that timely access to care is primarily dictated by the propensity to schedule care and/or the ability to identify and navigate scheduling processes soon after a concussion has occurred.
Prior work has emphasized the importance of timely care after a concussion in providing an accurate diagnosis, initiating treatment early in recovery, and contributing to improved patient outcomes. 2,3,7,8,12,15 –17,24 Our study identified a number of areas that may affect time from the injury to a specialty evaluation and subsequently patient outcomes. Specifically, the division of time to the specialty evaluation into 2 sequential time frames, that is, time from the injury to scheduling and time from scheduling to the specialty evaluation, allows for a preliminary understanding of how patient and injury factors specifically influence the process of accessing care after an injury. The number of days between the injury and specialty evaluation provides a global view of accessing care, the distinct time frame between the injury and scheduling could describe the propensity to access care, and the time between appointment scheduling and the initial specialty evaluation could better reflect actual barriers that exist in accessing concussion care after scheduling has occurred (ie, socioeconomic, demographic, geographic, or availability obstacles to attending in-person visits).
Our results indicate that a history of concussion was associated with an increased propensity to access care, as evidenced by shorter times to appointment scheduling. It could be that patients with a prior diagnosed concussion are more experienced at navigating health care systems after an injury and thus are more adept at scheduling specialty care visits early after sustaining a concussion. Conversely, other results from our study indicated that a history of migraines, sleep problems, or learning disabilities, all of which require navigation of complex health care systems to receive a diagnosis, did not influence time to a specialty evaluation after a concussion. A previous study reported that knowledge of concussion symptoms, attitudes, and self-reporting intentions was not affected by a history of recent (<12 months) concussion among pediatric and adolescent athletes. 4 Further, youth female athletes, as well as female parents, have reported greater knowledge of concussion symptom presentation, 4,14 but we did not observe any substantial sex differences in the time to specialty evaluation within our sample. Taken together, this may indicate that concussion knowledge, secondary to injury history, may not be the driving factor in the relationship between a history of concussion and propensity to access care after current injury.
The influence of a patient’s prior clinical relationship with the health care system is particularly relevant to clinical practice. Our multivariable analysis revealed that patients who had a prior clinical relationship with the orthopaedics department for any injury or condition demonstrated a quicker time to scheduling and presented sooner for a specialty evaluation, while receiving any care at the hospital system or prior care within the concussion program did not. Importantly, simply establishing patients in the overall hospital system may not result in patients scheduling or undergoing a specialty evaluation sooner after a suspected concussion. It should also not be assumed that patients with a previous visit to a specialty program for concussion will schedule or present sooner than those without this preexisting relationship. Efforts to reduce the time between the injury and specialty evaluation or to improve the propensity for accessing care may include establishing a clinical relationship between potential patients and the department as a whole, although it should be noted that varying department and clinic-specific factors may limit the generalizability of this finding.
The source of patient referral remains an important factor in clinical presentation time. Patients referred to our concussion program from primary care providers presented approximately 4 days later than patients referred from other sources. This relationship is likely complicated by insurance plan constraints, which may require referral for specialty care visits, presenting an additional barrier to timely access to specialty care after concussions. Although timely access to care after concussions is delayed when patients first consult their primary care provider, considerations should be made regarding the important role that these providers play in managing clinical volumes for specialty care clinics. Primary care providers, when appropriately trained and experienced with concussion care, can help triage those patients who would be better served by specialty providers, particularly among patients whose symptoms do not resolve within typical time frames. However, our data indicate that such a process of referral (ie, primary care provider to specialty care), even if most appropriate for patient triaging, may result in several days’ delay in accessing specialty care, subsequently impacting recovery outcomes.
Important to address is the clinical significance of our results. The time to an evaluation was delayed by approximately 4 days after referral from a primary care provider, reduced by approximately 1.5 days among patients with a history of concussion, and reduced by approximately 2 days for patients with a previous visit to the orthopaedics department. Patients presenting to specialized concussion care centers >7 days after a concussion are at an increased risk of prolonged symptom duration and delayed return to sports 2,3,7,16,24 ; however, no research has investigated the relationship between time to a clinical evaluation as a continuous variable and treatment outcomes. Thus, it is unclear how a 1.5- to 2-day delay in the time to an evaluation specifically affects recovery outcomes. Previous research has suggested that each successive day of delay in the initiation of physical activity after a concussion is associated with worse recovery outcomes, including an increased time to return to sports and return to school/work. 17 The initiation of aerobic activity at 5 versus 8 days after a concussion is associated with a hazard ratio for return to sports of 0.41 versus 0.22, respectively, compared to patients beginning aerobic activity on the first day after a concussion, 17 thus demonstrating that a few days’ delay in an evaluation and subsequent delay in clinician-initiated treatment, namely, aerobic exercise, may result in significant changes in patient outcomes, although further research should be conducted in this area.
A number of demographic, medical history, injury, and other patient factors were not significantly predictive of the time to clinical presentation, despite prior literature supporting their association with clinical recovery. 13,20 Most notable is the patient- and parent-reported symptom burden at the time of clinical presentation. Patients with a higher symptom burden after the injury did not schedule or present for a specialty evaluation sooner than patients with fewer symptoms. This is particularly curious, as delays in clinical presentation would provide patients with additional time for symptoms to resolve in comparison to patients who present for the evaluation within days of the injury. The time of year was also not significantly predictive of the time to an evaluation in this concussion clinic, although it is unclear how varying clinical volumes associated with the beginning and end of high school sports seasons affected this finding. Age, sex, and other demographic characteristics, such as race, ethnicity, and estimated income level, were not significantly associated with time to the initial specialty evaluation. There was a notable underenrollment of racial and ethnic minority participants in this study, which creates additional complexity in interpreting our findings. For example, only 1.4% (n = 3) of the total sample (n = 220) reported American Indian/Alaskan Native race, leading to an inability to perform statistical testing for this variable. This may also have implications for the generalization of our results to more diverse patient populations. Further, although a range of socioeconomic indicators, including parent education level, insurance type, and income estimate, were analyzed, these measures may not provide the level of granularity necessary to identify subtle differences between socioeconomic classes in their ability to access timely concussion care. The retrospective nature of this study does not allow for an investigation of more accurate or granular data.
Limitations
Our results should be interpreted within the context of specific limitations. Most important is that our sample was composed only of patients who were seen in our specialty concussion program. As such, while time to a specialty evaluation may be one measure of the ability to access concussion care, other important metrics such as the ability of a patient to access any care after a concussion were not collected as part of this study. Secondarily, this study sample was examined at a sports medicine center with clinical locations in the greater metropolitan area of a single city. Thus, the results of our study may not translate to other populations or geographic areas, such as young adults or more rural communities, as well as other clinical programs with different scheduling procedures. Further research may be necessary to understand how our results generalize to other care settings, such as urgent, emergency, or primary care clinics, as well as among other service delivery models, such as telehealth. The results of this study may best generalize to clinics employing a specialist-based service delivery model.
Other variables potentially affecting the timeliness of concussion care, such as provider availability, clinical schedules, ease of scheduling processes, flexibility in parent work schedules, patient school schedules, issues affecting transportation reliability (eg, weather, public transportation options, etc), and other related factors, were not assessed. This may explain why after univariably analyzing a comprehensive list of all available variables, our multivariable model only explained 24% of the variability observed in the time to a specialty evaluation (R 2 = 0.24). A comprehensive understanding of approaches to reduce the time between a concussion and the initiation of treatment may require future research to investigate variables beyond those assessed in the present study. Clinic-specific factors, such as provider availability or scheduling processes, as well as family/patient perceptions, knowledge, or familiarity of specialty care, may provide greater insight into issues that exist in scheduling and attending clinical visits earlier in concussion recovery.
Further, limitations exist within retrospective research. Information on patient behavior before the initial evaluation was not available to the study team. Thus, it is unclear if patients were seen for care by other practitioners (athletic trainers, emergency or primary care physicians) before the initial evaluation, and the treatment recommendations that patients received before presentation at our specialty clinic are unknown. This limitation may be particularly relevant for patients referred to a specialty clinic by a primary care physician. The time between an injury and initial evaluation by a primary care provider or the time from the evaluation by a primary care provider to presentation at the specialty clinic was not collected in this study.
Our secondary analysis described issues that may exist in the process of scheduling and attending clinical visits after a concussion. Patients and families contacted our program for clinical scheduling a mean of 7.2 days after the occurrence of a concussion. This is particularly important, given the emphasis of previous research on the 1-week time frame to initiate early aerobic exercise after a concussion for improved patient outcomes. 12,17,18 Only 61% of patients seen for care in our sample had contacted the clinic for appointment scheduling within 7 days of a concussion. Patient factors such as a history of concussion, referral source, and a preexisting clinical relationship demonstrated an association with time to scheduling but not with time from scheduling to the specialty evaluation. Efforts to reduce the time between the injury and initial specialty evaluation may include a focus on increasing patient/family propensity to access concussion care, such as ensuring that patients without a history of concussion are knowledgeable of available medical resources, establishing clinical relationships with patients before the occurrence of an injury (such as through community partnerships), and strengthening referral processes with local primary care providers. Other possible approaches to decrease the time to an evaluation include continuing education for coaches, parents, and other patient-facing clinicians regarding the importance of early evaluations after a concussion as well as expanding specialty clinic hours or outreach programs in rural or underserved areas; however, these strategies have not been thoroughly researched, and it is not clear, based on the results of this individual study, if such approaches would necessarily contribute to a reduced time to an evaluation among patients with concussions.
Patients attended clinical visits quickly after scheduling (mean, 2.6 days), which may indicate that not undergoing timely evaluations after a concussion is primarily attributed to patient/family propensity to contact care centers and not in the ability to attend in-person visits at specialty care clinics. This may have implications for future research seeking to increase the accessibility of acute or subacute medical care for patients after a concussion and may affect the clinical feasibility of future studies attempting to evaluate, diagnose, or initiate treatment early after a concussion in the specialty care setting.
Conclusion
A history of concussion and having a preexisting clinical relationship were associated with a shorter time to evaluation after a concussion. Referral from a primary care physician was associated with a longer time to evaluation. Issues may exist in the propensity to access care after an injury, resulting in delays for initiating early treatment. This investigation identified several areas for consideration to improve the timeliness of a specialty evaluation after a concussion. This may be of relevance for clinicians seeking to intervene with rehabilitative strategies earlier in concussion recovery.
Footnotes
Final revision submitted March 27, 2023; accepted April 14, 2023.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto. Unrelated to this study, Dr. Howell has received research support from the Eunice Kennedy Shriver National Institute of Child Health & Human Development (R03HD094560, R01HD108133), the National Institute of Neurological Disorders And Stroke (R01NS100952, R43NS108823), the National Institute of Arthritis and Musculoskeletal and Skin Diseases (1R13AR080451), 59th Medical Wing Department of the Air Force, MINDSOURCE Brain Injury Network, the Tai Foundation, the Colorado Clinical and Translational Sciences Institute (UL1 TR002535‐05), and the Denver Broncos Foundation. The remaining authors declare no conflicts of interest. This study did not receive any financial support.
Ethical approval for this study was obtained from the University of Colorado (No. PAM002-1).