
Abstract
Objective:
In this paper, we provide the rationale behind and a description of BrainLevel, a new cognitive rehabilitation intervention for children with acquired brain injury.
Rationale:
Children with acquired brain injury frequently report cognitive problems and consequently problems in participation, psychosocial functioning, family functioning and quality of life. Computerized repeated practice of specific cognitive tasks (so-called ‘brain training’) improves performance on those specific or highly similar tasks, but rarely leads to better daily life functioning. Adding strategy use instruction as an intervention component, with the aim to transfer task-specific effects to other contexts, may yield positive effects on cognitive and daily life functioning of children with acquired brain injury.
Description of the new intervention:
In BrainLevel, computerized repeated practice is offered via the online training programme BrainGymmer. For the strategy use instruction, we developed a protocol to provide and practice function-specific and metacognitive strategies. The intervention period is 6 weeks, during which children train five times per week for 30 minutes per day at home with BrainGymmer. Additionally, they attend a weekly 45-minute strategy use instruction session on the basis of our protocol with a cognitive rehabilitation specialist.
Discussion:
BrainLevel is innovative in combining computerized repeated practice with strategy use instruction as cognitive rehabilitation for children with acquired brain injury. Currently, we are investigating the effectiveness of BrainLevel. In this paper, possible adaptations to tailor BrainLevel to other games or contexts, or to incorporate novel scientific insights, for example regarding optimal intervention duration and intensity, are discussed.
Introduction
Children with acquired brain injury frequently report problems in a variety of cognitive domains, such as attention, working memory and executive functions (e.g. inhibitory control, cognitive flexibility and planning).1 –3 In turn, these cognitive problems negatively impact their participation, family functioning and quality of life.4 –7
Given the cognitive problems of children with acquired brain injury, there is a high need for effective cognitive rehabilitation. Cognitive rehabilitation is a systematic intervention targeting cognitive problems with interventions in the form of repeatedly practicing a specific cognitive task, providing (metacognitive) strategies and/or using external compensatory aids, with the aim to improve patients’ daily functioning.8,9
We have recently developed BrainLevel, a new multi-component cognitive rehabilitation intervention for children with cognitive problems after acquired brain injury. BrainLevel combines computerized repeated practice and strategy use instruction, for which the rationale is discussed below. We are currently evaluating BrainLevel in a multicentre clinical trial. In the present article, the rationale and description of BrainLevel is presented. The Template for Intervention Description and Replication (TIDieR) checklist and guide 10 are used as primary framework for the article, supporting clear reporting of all aspects of the intervention (see Supplemental Appendix 1).
Rationale for BrainLevel
Preliminary evidence suggests that multi-component cognitive interventions combining computerized repeated practice and strategy use instruction are promising for cognitive rehabilitation of children with acquired brain injury.11 –13
A recent systematic review on cognitive rehabilitation for children with acquired brain injury showed that evidence for the use of technology in providing cognitive rehabilitation is increasing. 11 Specifically, cognitive functions are trained with technological interventions such as computerized repeated practice, meaning repeated practice of computer games (also sometimes referred to as “brain training” or “drill-based training”). 11
Computerized repeated practice is a non-invasive training approach in which patients repeatedly play specific computer games that have been specifically developed to improve cognitive functioning. Computerized repeated practice of cognitive tasks underlies the assumption that repeated practice of (cognitive) computer games will improve a wider range of cognitive functions and even other domains of functioning, such as academic performance.
Computerized repeated practice has been indicated to be a feasible cognitive rehabilitation approach for various groups of acquired brain injury patients, for example, adult patients with traumatic brain injury, 14 children with cancer-related brain injuries15,16 with traumatic brain injury. 17 The use of computer games is also often compatible with interests of children and the game-like elements have previously been found to lead to more perseverance and motivation during training. 18 Patients can complete the training with minimal supervision while still receiving immediate feedback on their performance.14 –16 Task difficulty can be automatically adapted to the level of performance of the player.
Improvements after computerized repeated practice are found on cognitive tasks that are practiced during the intervention, but improvements on tasks of cognitive functions other than the trained functions or on daily life functioning are small to non-existent.15 –17,19,20 In other words, there is only very limited evidence for the generalizability of the improvements achieved with computerized repeated practice to daily functioning, across different environments and on the long-term.11,13 Comparable results are found after computerized repeated practice in a wide range of pediatric populations, 21 making other solutions and further research necessary.
A promising development in pediatric cognitive rehabilitation are multi-component interventions, combining technology in the form of computerized repeated practice with instruction concerning the use of strategies. 13
In young, healthy adults, improvements on untrained cognitive tasks after repeated practice of similar tasks were associated with increased use of relevant strategies known to improve performance on these tasks. 22 This suggests that, at least in healthy adults, improvements after repeated practice may underlie implicit and spontaneous changes in strategy use. In contrast, children with acquired brain injury may need explicit instructions on which strategies can be used to improve cognitive performance and other areas of functioning. Specifically, improving the effectiveness of the computerized repeated practice for children with acquired brain injury in terms of transfer to other (cognitive) domains may be achieved by supplementing these kinds of interventions with instruction on strategy use in the form of therapeutic guidance on how to apply what was learned during the computerized practice to various other settings or situations. 8
Strategy use instruction can include provision of function-specific strategies to support one cognitive function, such as mnemonics for semantic memory, as well as explanation of higher-level strategies such as metacognition (i.e. the general ability to oversee how various tasks can be approached) to support application in various settings or situations. However, the availability of interventions combining computerized repeated practice with strategy use instruction for children with acquired brain injury is limited. Moreover, protocols used for these interventions are often not clearly described, making it difficult to clinically implement or scientifically (re-)evaluate them. 10
Description of BrainLevel
BrainLevel consists of the modern, motivating computer-based cognitive retraining BrainGymmer targeting a wide range of cognitive functions combined with a protocol which we developed containing strategy use instruction on how to improve these cognitive functions, both when repeatedly practicing on the computer as well as in daily life situations. Cognitive domains targeted are attention (i.e. selective attention, divided attention and sustained attention), working memory and executive functions (i.e. inhibitory control, cognitive flexibility and planning).
The computerized repeated practice provides the opportunity to first explain the strategies in a game-like context before linking them to the child’s own daily life situations. Moreover, repeated task practice is thought to facilitate repetition and thereby consolidation of these strategies. The strategy use instruction is hypothesized to promote the use of strategies on cognitive tasks as well as the generalization of the improved cognitive functioning by explicitly relating the newly acquired strategies to relevant daily life areas.
Materials
A detailed protocol for the strategy use instruction was developed, and the clinicians providing the intervention are trained and instructed accordingly in an instruction session with the developers of the protocol. The protocol describes the content of six strategy use instruction sessions (see below). To facilitate the discussion of the strategies in the context of the computer games, we developed hard copy booklets and cards containing visualization of the computer games. These booklets and cards are used during the strategy use instruction sessions to provide an easy, low-key manner of looking, describing and using the different elements of the computer games to practice the strategies. For example, to discuss and practice the working memory strategy in the context of the Digit game (see Figure 1 and Table 1), clinicians and children can use printed cards showing the numbers from 1 to 9 and lay them on a matrix in a specific order, just like it is done in the computer game. Finally, clinicians are provided with a notebook, which can be used to make notes during the strategy use instruction sessions. The notebook is structured in line with the session outline.
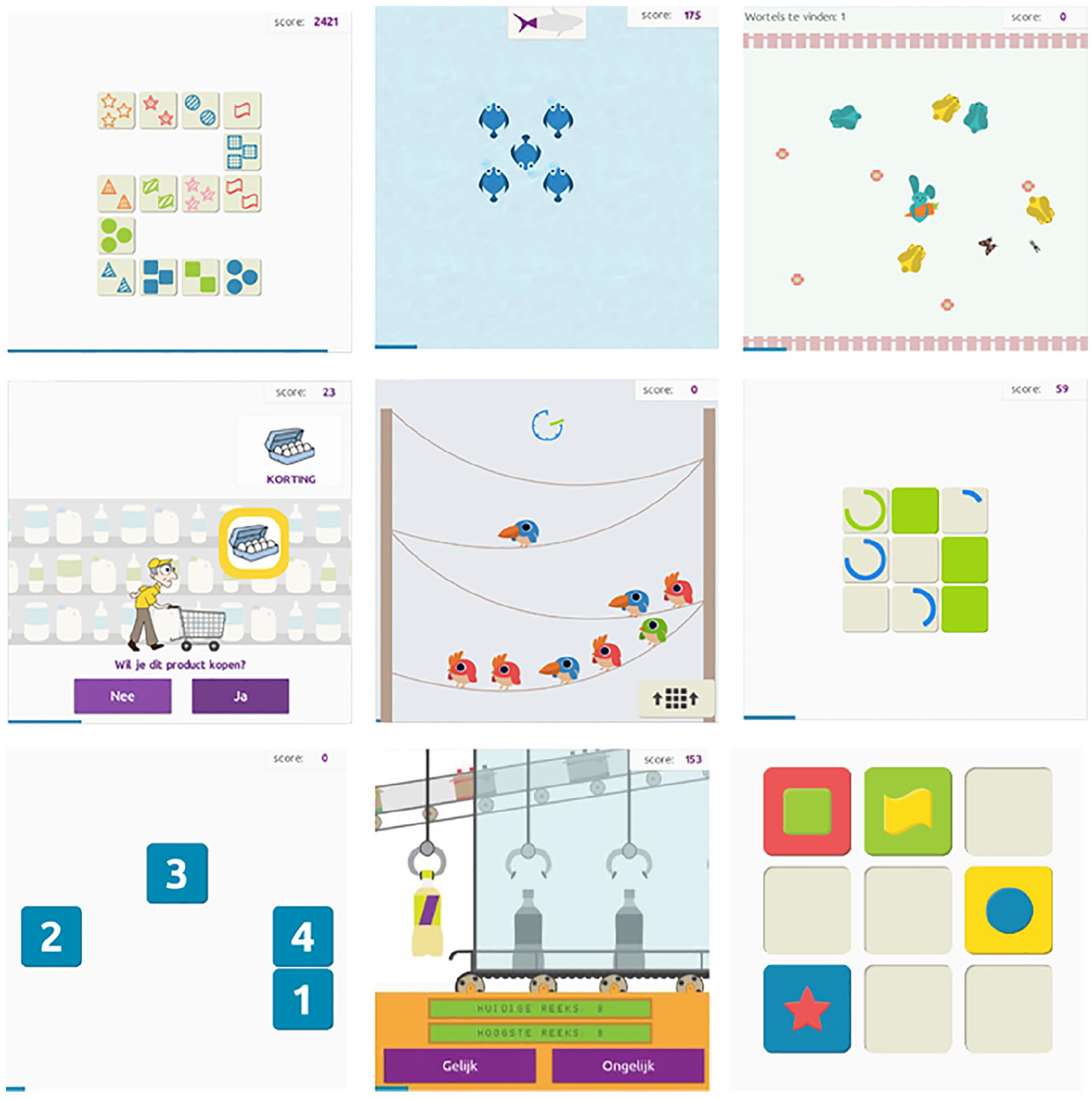
Screenshots of the BrainGymmer games. From top to bottom, left to right: Out of Order, Bait, Tracker, ShopShift, Birds of a Feather, Pay Attention, Digit, N-back and Multi Memory. Reproduced with permission from BrainGymmer (www.braingymmer.com).
Detailed description of the selected games.
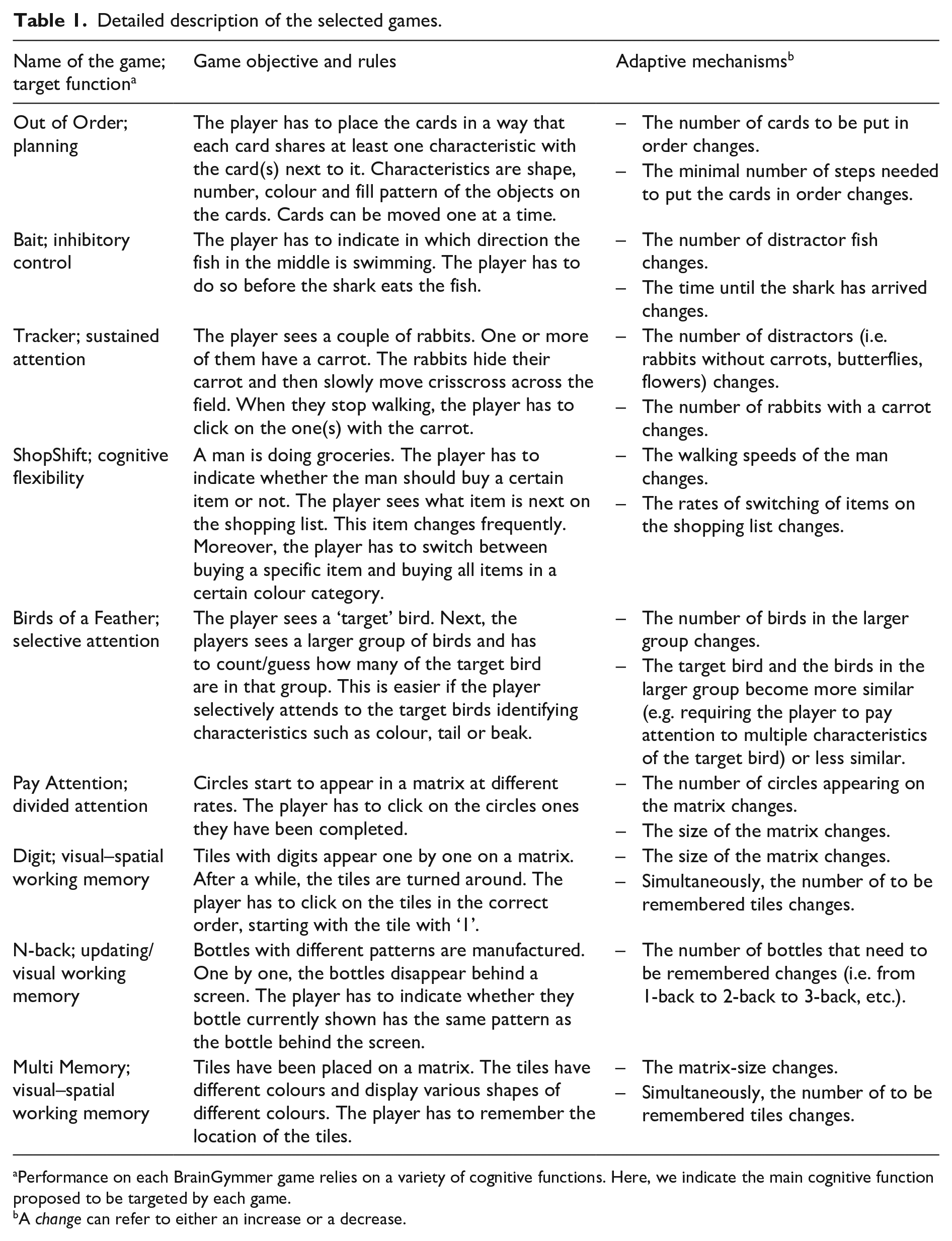
Performance on each BrainGymmer game relies on a variety of cognitive functions. Here, we indicate the main cognitive function proposed to be targeted by each game.
A change can refer to either an increase or a decrease.
At the start of the intervention, each participating child receives a personal BrainGymmer account, which can be accessed via the internet. This account gives access to the environment for the computerized repeated practice. Also, children are provided a workbook with exercises to explicitly apply the strategies learned during the strategy use instruction sessions in their daily living activities. For each strategy, the workbook includes a visualization and description of how this strategy can be applied in the context of the computer games from the computerized repeated practice.
Procedure
Currently, BrainLevel is only offered in the context of the multicentre trial investigating the outcomes of the intervention. If BrainLevel shows to be beneficial for children with acquired brain injury, BrainLevel will be made available for use in rehabilitation centres and specialized schools. Cognitive rehabilitation specialist can offer BrainLevel to patients who meet the description of the target population (see below).
Duration and intensity
The intervention period is set at 6 weeks. During this time, children train (i.e. play the BrainGymmer games) five times a week (i.e. 30 times in total) for approximately 30 minutes per day. The duration of each of the nine games was set to 5 minutes per game. When all training sessions have been completed, all games will have been played 20 times (i.e. 100 minutes per game). Total training time is 900 minutes. If participants have not completed the 900 minutes of training after 6 weeks, the training period is extended to a maximum of 7 weeks.
Players can start one training session per day, which provides them with a pre-determined selection of the games in a pre-determined order which is the same for all participants. Once a player has played the required games of the day, the programme cannot be accessed again until the next day. Thereby, we ensure that the intervention is sufficiently spaced over the intended period of time.
The strategy use instruction is conducted alongside the BrainGymmer training in six weekly, 45-minute sessions at the rehabilitation centre or specialized school with the therapist.
Optimal duration of cognitive rehabilitation training for children with acquired brain injury has yet to be determined, since there is considerable variation in the training periods of previous studies. 16 With the chosen duration and training intensity of the present intervention, we aim to find a balance between the amount of training necessary to elicit changes in cognitive performance as well as daily life functioning, and the feasibility to keep participants motivated and compliant with the training schedule. Duration and intensity of our intervention are comparable to previous studies in various populations, such as children with acquired brain injury, attention-deficit hyperactivity disorder or cancer-related cognitive difficulties.16,23,24 For typically developing children, it has previously been found that sufficient spacing of an intervention over at least 20 days yields the best results in terms of improved cognitive functioning. 25
Target population
BrainLevel is developed for children who are referred for cognitive rehabilitation after acquired brain injury. Both the computerized repeated practice and the strategy use instruction protocol have been developed to be suitable for children aged 8–18 years. From at least age 8 years onwards, children have been shown to be able to benefit from strategy use instruction (including function-specific cognitive strategies and metacognitive strategies) in terms of improved strategy use and application of those strategies to relevant situations.26,27
BrainLevel is only suitable for children who are sufficiently able to understand and potentially apply the instructions on the games and the strategies. Treating clinicians can determine this on an individual basis. It is advised not to use the intervention for children who experience extreme sensibility for visual stimuli and/or have uncontrolled epilepsy. Moreover, children have to be able to control the arrow keys of a keyboard and/or to use a computer mouse. They have to be able to perceive a complete screen and to adequately process the stimuli of the computer games. Finally, to benefit from the strategy use instruction sessions, sufficient understanding of the language in which the session is held, is required.
Intervention provider
The strategy use instruction is provided by a cognitive rehabilitation specialist, in other words, a person with experience in cognitive rehabilitation. This can be the cognitive trainer or occupational therapist who is part of the rehabilitation team or the teaching/support team of the specialized school.
The computer games can be played independently by the children at home. In principle, no involvement of parents or caregivers is required. However, children may benefit from parental or caregiver support to increase persistence with the training, and to encourage application of learned strategies in daily life situations. Parents or caregivers can make use of the child’s workbook to get insight into which strategies have been discussed with the cognitive rehabilitation specialist, and in which situations these strategies may be applicable and useful for their child.
Intervention settings and modes of delivery
Children play the computer games at home, at their preferred time. It is advised to play the games on a personal computer or laptop. Alternatively, the games can be played on a tablet computer. Due to the small screen size, children are discouraged to play the games on a smartphone. The games can be played without supervision of an adult.
The strategy use instruction is offered on the basis of a detailed paper protocol (see ‘Materials’) and provided in a one-on-one setting by the cognitive rehabilitation specialist. In principle, parents or caregivers do not attend these sessions. Strategy instruction sessions take place at the rehabilitation centre or the specialized school for children with disabilities of the participating child.
Individual tailoring
Essential to the effects of the computerized repeated practice is the adaptivity of the computer games. Adaptivity of computerized repeated training to an individual’s level of performance keeps the training stimulating and challenging while keeping the balance with the level of frustration (i.e. the task should not be too difficult).28,29 Difficulty levels of the games are either increased or decreased based on the performance of an individual28,29 In the games used in the current intervention, this can for example be achieved by increasing or decreasing the number of stimuli presented, or by increasing or decreasing the speed of the stimuli presentation. In Table 1, the adaptive mechanisms for each of the nine games used in the current intervention are described.
Participants receive feedback on their performance throughout the game. Feedback varies per computer game and is given in the form of a green check mark for correct responses or a red cross for incorrect responses, positive or negative ‘sounds’, increase in level and/or increase in points achieved. Before the start of each game, a participant is shown his/her average score over previous game sessions and his/her high score for that particular game.
In the strategy use instruction sessions, children and their treating specialist are encouraged to come up with their own examples of relevant life situations in which a certain strategy can be applied, connecting the strategies directly to what is important to them. Moreover, strategies are explicitly linked to a child’s individual goal that they formulate before the first strategy use instruction session. Thereby, we aim to enhance motivation and training perseverance of each individual child and to achieve improvements in the child’s meaningful life areas.
Computerized repeated practice
For the computerized repeated practice, we use existing cognitive games provided by the training software BrainGymmer (www.braingymmer.com). BrainGymmer is an online available so-called ‘brain-training’ programme developed to improve a variety of cognitive functions with the use of game-like cognitive training tasks. This programme has previously been used as an intervention for adult acquired brain injury patients. 30 A separate training environment was developed, tailored to the aims and needs of the new intervention. This was done to ensure that, in the context of BrainLevel, the BrainGymmer games would remain constant, because the commercially available version changes constantly. A selection of nine games was made that are appropriate to target the cognitive functions known to be common targets in cognitive rehabilitation for children with acquired brain injury (see Figure 1). A description of the selected games is presented in Table 1.
Strategy use instruction
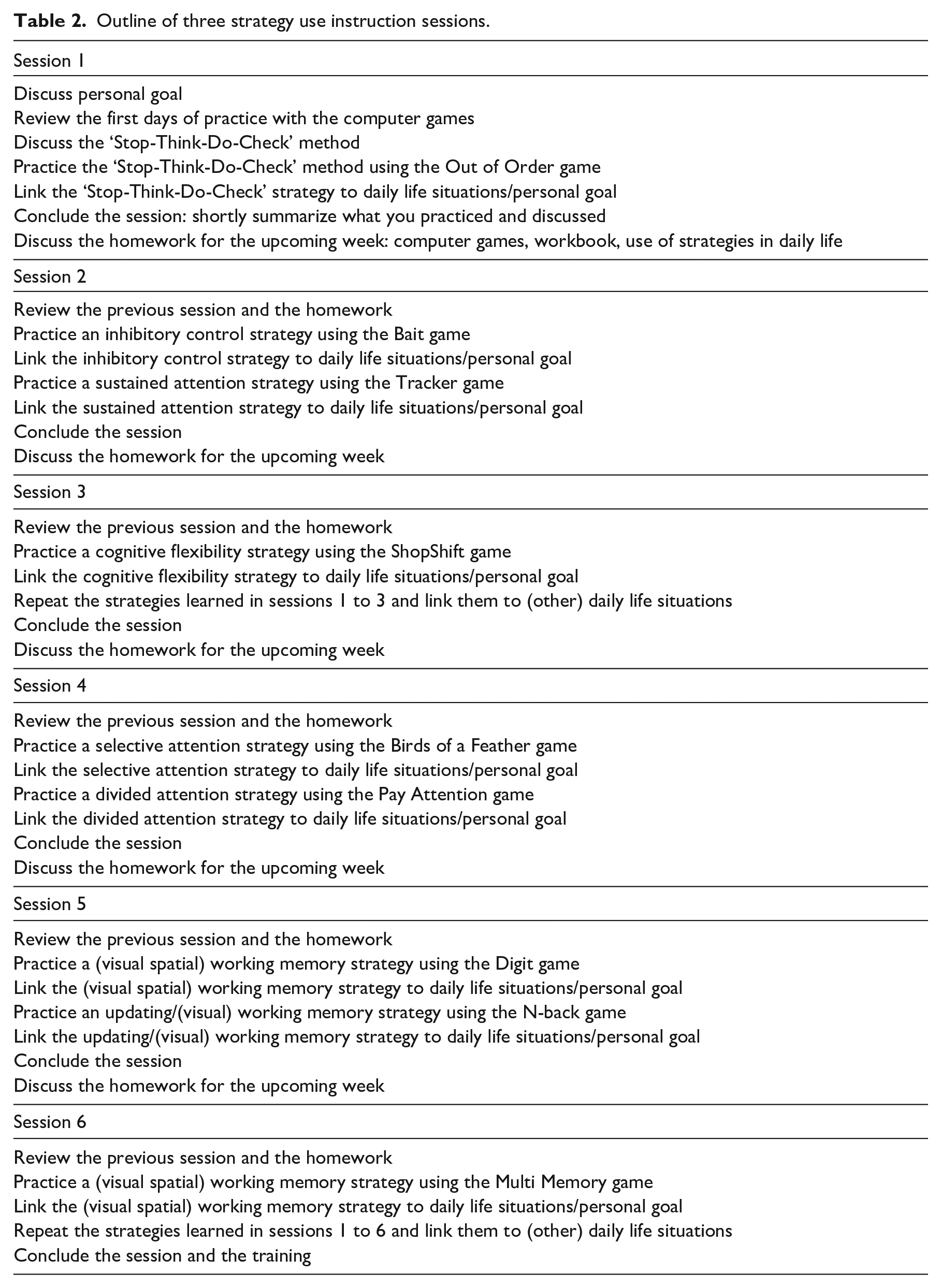
To complement the computerized repeated practice, participants receive six sessions of strategy use instruction. Each strategy use instruction session contains three key elements: (1) explicitly discussing one or two computer games and the accompanying cognitive strategies, (2) linking the strategies to the child’s own daily life situations and the personal goal of the child and (3) discussing how the children can practice these strategies at home within their own context and activities (homework). Across strategy use instruction sessions, all strategies are rehearsed multiple times and repeatedly linked to daily life situations and personal goals. The various elements of the strategy use instruction sessions are following a consistent pattern across sessions. The outline of the six strategy use instruction sessions is presented in Table 2.
Outline of three strategy use instruction sessions.
Key element 1: Explicitly discussing one or two computer games and the accompanying cognitive strategies
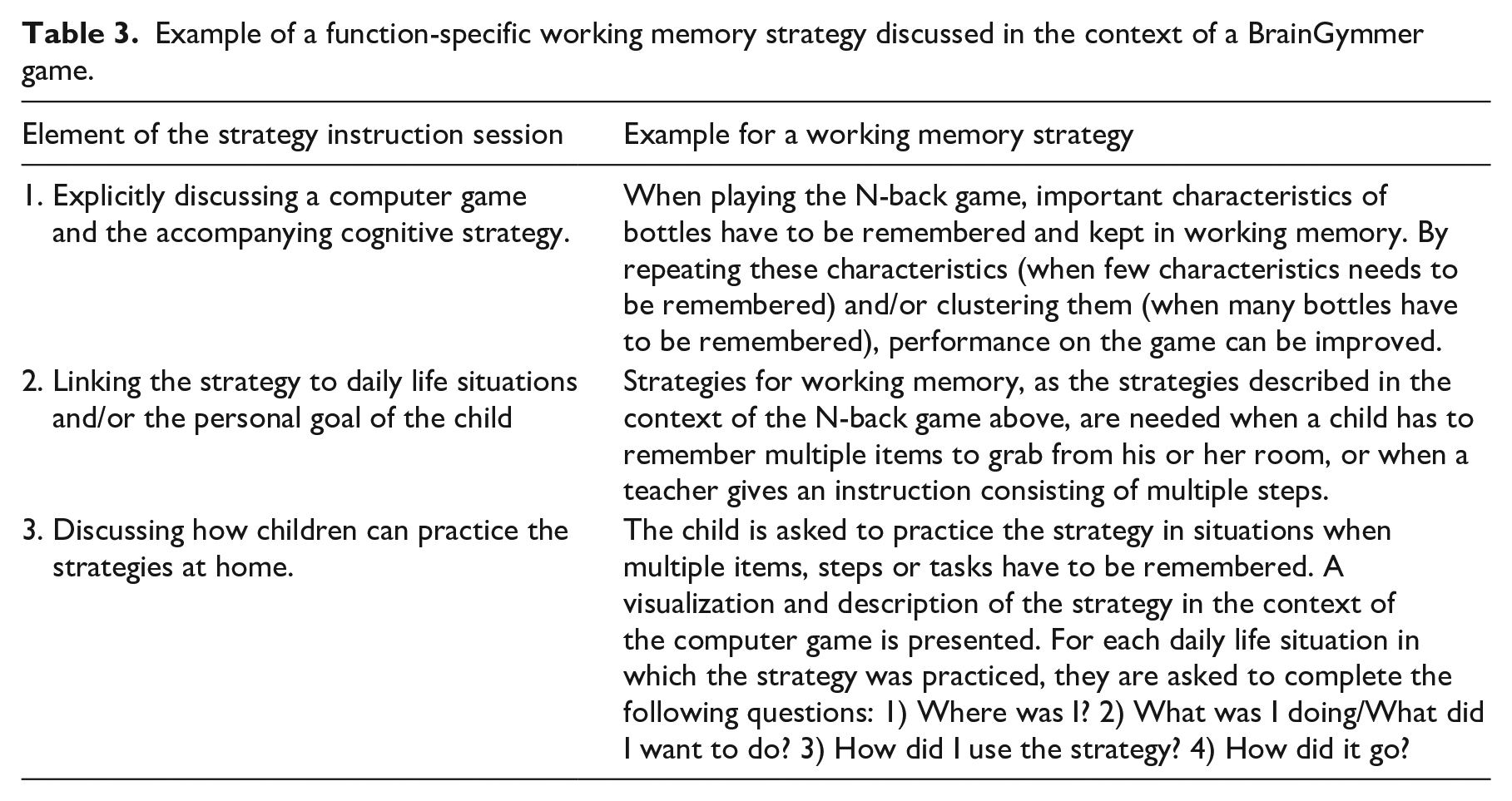
During strategy use instruction, two types of strategies are discussed, practiced and linked to daily life situations and personal goals: function-specific strategies and metacognitive strategies. Function-specific cognitive strategies are strategies that provide specific support for a certain cognitive function, such as working memory (for an example, see Table 3). Metacognitive strategies are task-overarching ways of structuring thoughts. These strategies are aimed at improving children’s ability to select an appropriate (function-specific) cognitive strategy for the context at hand and/or behave in a situational appropriate manner. The metacognitive strategies discussed in the current intervention are based on a ‘Stop – Think – Do – Check’ self-instruction method 31 (see Figure 2).
Example of a function-specific working memory strategy discussed in the context of a BrainGymmer game.
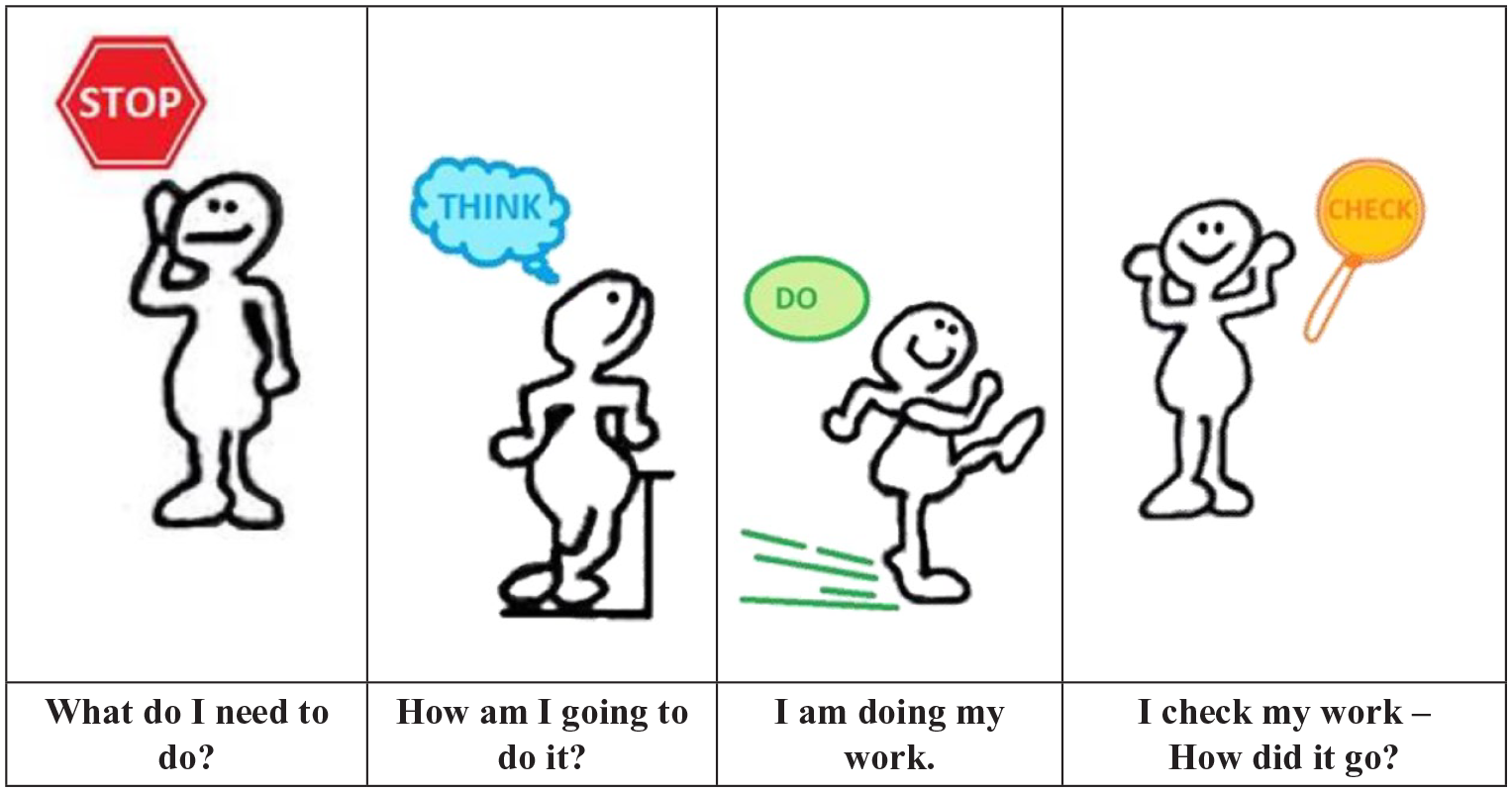
The ‘Stop-Think-Do-Check’ method as used in BrainLevel.
The computer games provide an easy, motivating context to discuss and practice the strategies. The games that are discussed in the sessions are Out of Order targeting planning in session 1, Bait targeting inhibitory control and Tracker targeting sustained attention in session 2, ShopShift training cognitive flexibility in session 3, Birds of a Feather directed at selective attention and Pay Attention targeting divided attention in session 4, Digit training visual-spatial working memory and N-back training updating/visual working memory in session 5, and Multi Memory directed at visual-spatial working memory in session 6 (see Table 1 for a description of the games). Children are already familiar with these games before the strategy instruction sessions, because they have been practicing them at home on their computer.
Children are asked to shortly describe what the goal is of a specific game. Together with the cognitive rehabilitation specialist, they discuss a cognitive strategy that can be used to improve their performance on the specific game. Children are first asked to come up with their own strategy. By thinking about the strategies themselves, we aim to activate their own knowledge of possible strategies. If the child cannot come up with a strategy, or if the strategy presented by the child is not relevant for the game at hand, the clinical professional can provide the strategy as described in the strategy instruction protocol.
The metacognitive strategy of the ‘Stop – Think – Do – Check’ method (see Figure 2) is introduced in the first strategy instruction session in the context of the Out of Order game. The game presents a challenging context to practice planning abilities. This provides an excellent context to discuss the different steps as posed by the ‘Stop – Think – Do – Check’ method. First, you need to stop other activities to focus on the game at hand (‘Stop’ step). Second, think about what you have to do in this task, and how you will approach the task (‘Think’ step). Third, take the steps that you planned in the ‘Think’ step. Fourth, check whether you performed the task correctly (‘Check’ step). If so, you can move on to the next task. If not, go back to the ‘Think’ step and reconsider your approach to the task. This method teaches children for example, to first make sure they understand the instructions of a certain task or the requirements of a certain situation completely, before engaging in the task or situation.
The ‘Stop – Think – Do – Check’ method is used as a basic framework for the different computer games and daily life contexts discussed throughout all sessions of the strategy use instruction. In contrast, function-specific strategies are discussed in the context of one specific computer game. Table 3 shows an example of how a function-specific working memory strategy is discussed in the context of a computer game.
Key element 2: Linking the strategies to the child’s own daily life situations and the personal goal of the child
For each strategy, the protocol provides various examples of life situations to which the strategy can be linked. By explicitly discussing the strategies not only in the context of the computer games but also in relation to other cognitive tasks and daily life situations (such as completing homework, behaving in class, or reacting to friends or family), we aim to enhance generalization of the use of these strategies. Specifically, for each strategy, it is discussed in which daily life situation the strategy can be relevant, and how it can be applied there.
The metacognitive strategy based on the ‘stop – think – do – check’ method can be linked to all of the daily life situations mentioned above, as it provides an overarching strategy for approaching tasks or (complex) situations. Table 3 provides an example of how a function-specific strategy for working memory can be linked to daily life situations. For strategies for other cognitive functions, other life situations are relevant. For example, function-specific cognitive strategies for inhibitory control can be linked to situations in which a child has to wait for his or her turn in class. Strategies for cognitive flexibility are relevant for situations in which out-of-the-box thinking is required, or when something does not go as planned.
Key element 3: Discussing how children can practice the strategies at home
Children are asked to use the strategies discussed in the sessions in their daily life. Their workbook (see ‘Materials and procedure’) provides examples of situations in which the strategy is relevant. Children are asked to write down in which situations they practiced the strategies and whether it helped them improve or support their performance or functioning in that situation. Practicing the learned strategies in their own daily life is thought to be essential to achieve generalization of strategy use and thereby improvement in cognitive and daily life functioning. Table 3 provides an example of how children can practice strategies at home and how they use their workbook.
Discussion
BrainLevel fills the need for a modern, motivating cognitive intervention for children with acquired brain injury that has the potential to reach wide-ranging improvements in cognitive functioning beyond trained tasks in daily living areas.13,32,33 BrainLevel incorporates the element of so-called “brain training” through existent software for computerized repeated practice. However, instead of relying on the assumption that repeated task practice alone will lead to improvements on these computer games and tasks in daily life that depend on cognitive functioning that are not similar to the practiced tasks, BrainLevel explicitly provides a novel strategy use instruction protocol to enhance transfer effects.
The effectiveness of BrainLevel is currently being investigated in a multicentre clinical trial (Protocol IDs: NTR5639, NL54523.068.15). Participants are children with acquired brain injury who are referred for cognitive rehabilitation at one of eight parti-cipation rehabilitation centres or specialized schools for children with disabilities in the Nether-lands (Adelante Zorggroep, Valkenburg; Basalt Revalidatie, Den Haag; Brein Support, Arnhem; Heliomare, Heemskerk; De Hoogstraat Revalidatie, Utrecht; Libra Revalidatie & Audiologie, Eindhoven; Merem Medische Revalidatie, Hilversum; Revant, Breda). Results of the intervention study will be published when the trial is completed.
We expect that the effects of combining both repeated task practice and strategy use instruction will elicit greater and more wide-ranging effects than if both of these components were presented separately or sequentially. However, if found to be effective, the multi-component nature of BrainLevel prevents us from pinpointing which of the underlying mechanisms, or which interaction between them, is the main cause of the effectiveness of the intervention. 34
Possible adaptations to BrainLevel
BrainLevel was developed for children with cognitive problems after acquired brain injury for whom cognitive rehabilitation is indicated. However, during the intervention, no emphasis is put on the medical or psychological origin of the cognitive problems. Specifically, the intervention as described above now targets children with cognitive problems due to acquired brain injury, but the intervention may also be suitable for other pediatric populations who report cognitive difficulties, for example children with cerebral palsy, attention-deficit hyperactivity disorder or learning disabilities.
Duration and intensity of our intervention are comparable to previous studies in children with acquired brain injury and other populations such as children with attention-deficit hyperactivity disorder and cancer-related cognitive difficulties.16,23,24 In case future research shows that optimal training duration and intensity is shorter or longer than offered in the present intervention, the intervention protocol (including both the computer games and the strategy use instruction sessions) can easily be adapted based on these emerging insights.
In its current form, our intervention includes a selection of games from BrainGymmer targeting specific cognitive functions. The selection of games could be extended to incorporate an even more diverse array of games, or it could be tailored to include games targeted other cognitive functions. Other computerized cognitive retraining software, such as Cogmed, can also be suitable to combined with a protocol of strategy use instruction.
Our strategy protocol is now tailored to the games we selected from BrainGymmer. The computer games are used to explain and practice the strategies. The strategies are related to the cognitive domains which are targeted with the game, and not the game itself. Therefore, with minor adaptations, the chosen strategies and instructions can also be used for other games or software.
Currently, the protocol for strategy use instruction is written in Dutch. For future application in other countries, the strategy use instruction protocol can be translated to other languages.
Finally, the protocol is developed to have the strategy use instruction sessions at a rehabilitation centre or specialized school. With minor adaptations, it can be possible to hold the sessions online, in a digital one-on-one setting with the child and a cognitive rehabilitation specialist.
Clinical messages
There is currently no evidence-based preferred or recommended cognitive intervention for children with acquired brain injury.
Combining repeated task practice of various cognitive functions with strategy use instruction seems promising to achieve wide-ranging improvements in cognitive functioning and other life areas.
Our intervention combines repeated task practice in the form of computer games with strategy use instruction as a promising, modern, motivating cognitive rehabilitation programme for children with acquired brain injury.
Supplemental Material
sj-pdf-1-cre-10.1177_0269215521989652 – Supplemental material for Rationale and description of BrainLevel: Computerized repeated practice with strategy use instruction for children with acquired brain injury
Supplemental material, sj-pdf-1-cre-10.1177_0269215521989652 for Rationale and description of BrainLevel: Computerized repeated practice with strategy use instruction for children with acquired brain injury by Christine Resch, Petra Hurks, Arend de Kloet and Caroline van Heugten in Clinical Rehabilitation
Footnotes
Acknowledgements
We would like to thank Roeli Wierenga from Basalt Rehabilitation and Rachel Houtackers for their help with the development of the intervention protocol and materials.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The development of the interventin was funded by Johanna Kinderfonds (Project ID: 2014/0039-1552), Cornelia-Stichting (Project ID: 2014/0039-1552), and Stichting Rotterdams Kinderrevalidatie Fonds Adriaanstichting (Project ID: 14.09.30-2014/0039).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.