
Abstract
Background:
Glenohumeral dislocations often lead to glenoid bone loss and recurrent instability, warranting bony augmentation. While numerous biomechanical studies have investigated fixation methods to secure a graft to the glenoid, a review of available constructs has yet to be performed.
Purpose:
To synthesize the literature and compare the biomechanics of screw and suture button constructs for anterior glenoid bony augmentation.
Study Design:
Systematic review.
Methods:
A systematic review was conducted in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. There were 2 independent reviewers who performed a literature search using the PubMed, Embase, and Google Scholar databases of studies published between 1950 and 2020. Studies were included that compared the biomechanical outcomes of fixation for the treatment of anterior shoulder instability with glenoid bone loss.
Results:
Overall, 13 of the 363 studies screened met the inclusion criteria. The included studies measured the biomechanical strength of screws or suture buttons on a cadaveric or synthetic Latarjet construct. Screws and suture buttons were biomechanically similar, as both constructs exhibited comparable loads at failure and final displacement. Screw type (diameter, threading, or composition) did not significantly affect construct strength, and double-screw fixation was superior to single-screw fixation. Additionally, 2 screws augmented with a small plate had a higher load at failure than screws that were not augmented. Unicortical double-screw fixation was inferior to bicortical double-screw fixation, although construct strength did not significantly decrease if 1 of these screws was unicortical. Further, 2 screws inserted at 15° off axis experienced significantly higher graft displacement and lower ultimate failure loads than those inserted at 0° parallel to the glenoid.
Conclusion:
Suture buttons provided comparable strength to screws and offer an effective alternative to reduce screw-related complications. Augmentation with a small plate may clinically enhance construct strength and decrease complications through the dispersion of force loads over a greater surface area. Differences in screw type did not appear to alter construct strength, provided that screws were placed parallel to the articular surface and were bicortical.
Bone loss in shoulder instability is common in up to 22% of those with a first-time dislocation, and up to 90% of patients with recurrent instability have some measure of bone loss. 35,37 Significant glenoid bone loss, greater than 25% of anteroinferior glenoid bone attenuation, should be addressed through bony augmentation. 17,21,35,37 Several common grafts exist for the bony reconstruction of the glenoid: coracoid, iliac crest, distal tibia, and distal clavicle. 28,38,51,52 The Latarjet procedure is considered to be the most common method to address the bone loss of the glenoid, as it predictably restores stability and has favorable clinical and biomechanical outcomes. 5,28,31,32 Complication rates range from 9% to 30% after arthroscopic and open transfer of the coracoid through the subscapularis to the glenoid. 3,14,24,42 While the causes of complications are likely multifactorial, implant selection can play an important role in postoperative outcomes.
The most common fixation method of securing a bony graft to the glenoid involves screws. However, screw fixation has been associated with the following potential complications: nonunion (9.4%-10.1%); bone block resorption (59.5%); intraoperative and postoperative fractures (1.1%-1.5%); screw avulsion, twisting, or breakage (2.4%-6.5%); and soft tissue irritation (2.7%). 12,22,24 In addition, Griesser et al 24 found that of the 7% of cases that required reoperation, approximately 35% were related to symptomatic hardware. As a result, novel fixation methods without the use of screws have gained traction for treating anterior glenohumeral instability. In 2014, Taverna et al 50 first described the use of a suture button construct to secure an iliac crest tricortical bone graft. Since then, this novel suture button construct has shown promising clinical outcomes and excellent graft positioning while dramatically reducing hardware-related complications. 6,9 Despite the favorable results, a recent survey of 242 orthopaedic surgeons found that 98% preferred screw fixation during the Latarjet procedure as opposed to suture button fixation. 47
There are few reports to date that have comparatively assessed the biomechanics of various glenoid bony fixation techniques. As such, the objective of this systematic review was to compare the biomechanics of screw and suture button constructs for anterior glenoid bony augmentation.
Methods
Literature Search Strategy
This systematic review was performed in accordance with the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. An electronic search was undertaken to screen for articles reporting biomechanical data on bone graft fixation for anterior glenoid bony deficiency. The publication databases included PubMed, Embase, and Google Scholar. A targeted search was performed using the following terms: (“Latarjet procedure” or “anterior shoulder instability”), AND/OR (“biomechanical”) AND (“screw fixation” or “suture button fixation”). The reference lists of retrieved articles were analyzed for a review of potentially relevant studies that were not included in the original search.
Selection Criteria
Eligible studies for this review included English-language studies published between 1950 and 2020 that reported on the biomechanics of ≥1 fixation methods for anterior glenoid bony augmentation. Fixation devices included screws (augmented and nonaugmented) and suture-based (endobutton, cortical/suture button) devices. Exclusion criteria consisted of non–English-language studies, clinical outcome studies, case reports, techniques, reviews, expert opinions, abstracts, and conference presentations.
Study Selection
All articles were initially screened by 2 separate authors (J.N.M., J.S.) via the title and abstract. A third reviewer (K.D.P.) was available to review any discrepancies that were not agreed upon. After selection based on inclusion and exclusion criteria, the articles underwent a thorough full-text review. A total of 13 studies were included after a full-text review and cross-referencing (Figure 1).

Study selection flowchart.
All baseline characteristics were recorded along with biomechanical results. The included studies were further divided into the following subcategories: screw versus suture button fixation, screw type, single versus double screws, unicortical versus bicortical purchase, screw insertion angle, and cortical augmentation. Fixation outcomes were classified as the stability of graft fixation determined by the level of axial displacement resulting from an axial force applied directly to the graft or conjoint tendon.
Results
The characteristics of each of the 13 studies are summarized in Table 1. Cadaveric models were used in 8 of the included studies, 1,27,29,36,41,48,53,55 and synthetic materials were used in 5 of the studies. 4,19,40,45,54 A summary of the biomechanical findings of each study is shown in Appendix Table A1.
Characteristics of Included Studies a

a F, female; M, male; NR, not reported.
Screw Versus Suture Button Fixation
Essentially, 2 screws versus suture button fixation exhibited comparable loads at failure according to Provencher et al 36 (double suture button), Kazum et al 27 (single suture button), and Massin et al 29 (single suture button). Kazum et al 27 noted differences in the failure mechanisms between screw and suture button fixation. For specimens fixed with screws, 100% failed by graft fracture. In the suture button construct group, glenoid fractures accounted for 80% of the failures. 27 In addition, Reeves et al 41 recently found that two 3.75-mm titanium cannulated screws versus a double–suture button construct had comparable displacement at all pressure positions. However, when the load applied to the conjoint tendon doubled, the double–suture button construct had significantly greater displacement than screws in the inferior and central portions. 41 Williams et al 55 found that when the graft was directly loaded, 2 screws reached a greater load at failure than double–suture button fixation. However, the failure rate via graft fracture was higher with screw fixation (33%) versus suture button fixation (0%). 55 While there were no implant failures in either group, the mechanism of failure was different for each. Williams et al 55 and Provencher et al 36 found that suture buttons failed by displacement of the graft and formation of a gap between the graft and glenoid as opposed to the catastrophic failure of screws. Screw failure exhibited several types of failure as follows: screw medialization and cutting through glenoid cancellous bone, screw cutout, and graft fracture. Overall, 55% of graft failures in the screw construct group had damaged grafts or glenoid bone. 55 Azoulay et al 4 found that single– and double–suture button fixation exhibited >5 mm of displacement at all pressure positions, which was greater than with single- and double-screw fixation (Appendix Table A1). Individually, displacement with single–suture button fixation was significantly greater under superior and inferior forces than double–suture button fixation. 4 There was no significant difference between these 2 constructs when placed under a central force.
Screw Type
Studies that examined screw diameter, threading, and composition did not arrive at a definitive conclusion. A recently published systematic review and meta-regression of the biomechanical strength of Latarjet constructs found that each millimeter increase in the screw diameter significantly reduced the ultimate failure load. 25 Alvi et al 1 did not find a significant difference between two 3.5-mm stainless steel cortical screws versus two 4.0-mm stainless steel partially threaded cancellous screws in the final load at failure. Similarly, Shin et al 48 did not find any differences among the screw types tested, all of which consisted of fixation with 2 screws. These constructs included 4.0-mm partially threaded solid cancellous screws (bicortical), 4.0-mm partially threaded solid cancellous screws (unicortical), 3.5-mm fully threaded solid screws (bicortical), 4.0-mm partially threaded cannulated screws (bicortical), and 4.0-mm partially threaded captured screws (bicortical). Lastly, Massin et al 29 found that all groups were comparable in loads at failure when comparing two 4.5-mm malleolar solid screws, one 4.0-mm and one 3.0-mm self-compressive cannulated screws, and two 3.5-mm self-compressive cannulated screws. Specific screw configurations can be found in Appendix Table A1.
Single Versus Double Screws
Azoulay et al 4 showed that under central and inferior pressure at 200 N, the use of two 4.5-mm noncannulated cancellous screws for fixation resulted in significantly less displacement of the coracoid graft versus a single screw of the same type (Appendix Table A1). When under superior pressure at 200 N, displacement did not significantly differ between the use of a single screw or 2 screws. 4 In addition, both Frank et al 19 and Weppe et al 53 found that 2 screws produced significantly greater loads at failure versus a single 4.0-mm partially threaded cannulated screw and a single absorbable interference screw, respectively (Appendix Table A1).
Unicortical Versus Bicortical Purchase
Schmiddem et al 45 found that unicortical screw fixation had a significantly lower median load at failure versus bicortical screw fixation when using two 3.5-mm partially threaded solid metal screws (Appendix Table A1). Unicortical fixation reduced the fixation strength of the coracoid process by 45% compared to bicortical fixation. 45 Willemot et al 54 compared bicortical versus unicortical purchase as well. Screws were placed in the following 3 configurations: (1) both screws placed bicortically, (2) both screws placed unicortically, or (3) one screw placed unicortically and the other screw placed bicortically. In the second and third configurations, 4.5-mm and 3.5-mm screws incurred significantly less displacement versus 3.75-mm screws with a final 200-N axial load. This led the authors to recommend a larger diameter screw when either 1 or 2 screws are placed in a unicortical fashion. In the first configuration, there were no significant differences among screw types. However, Shin et al 48 did not find significant differences between unicortical versus bicortical fixation when using two 4.0-mm cancellous screws (Appendix Table A1).
Screw Insertion Angle
As the glenoid and the graft are frequently drilled separately, there is the potential for a nonlinear drill path when the bony surfaces are mated (Figure 2). Frank et al 19 found that a single 4.0-mm screw had failure loads at both a 0° and a 15° insertion angle. However, double-screw constructs were significantly stronger than single-screw constructs at 15° of insertion. Further, 2 screws inserted at 15° experienced significantly higher graft displacement and significantly lower ultimate loads at failure compared to 2 screws inserted at 0° (Appendix Table A1). 19
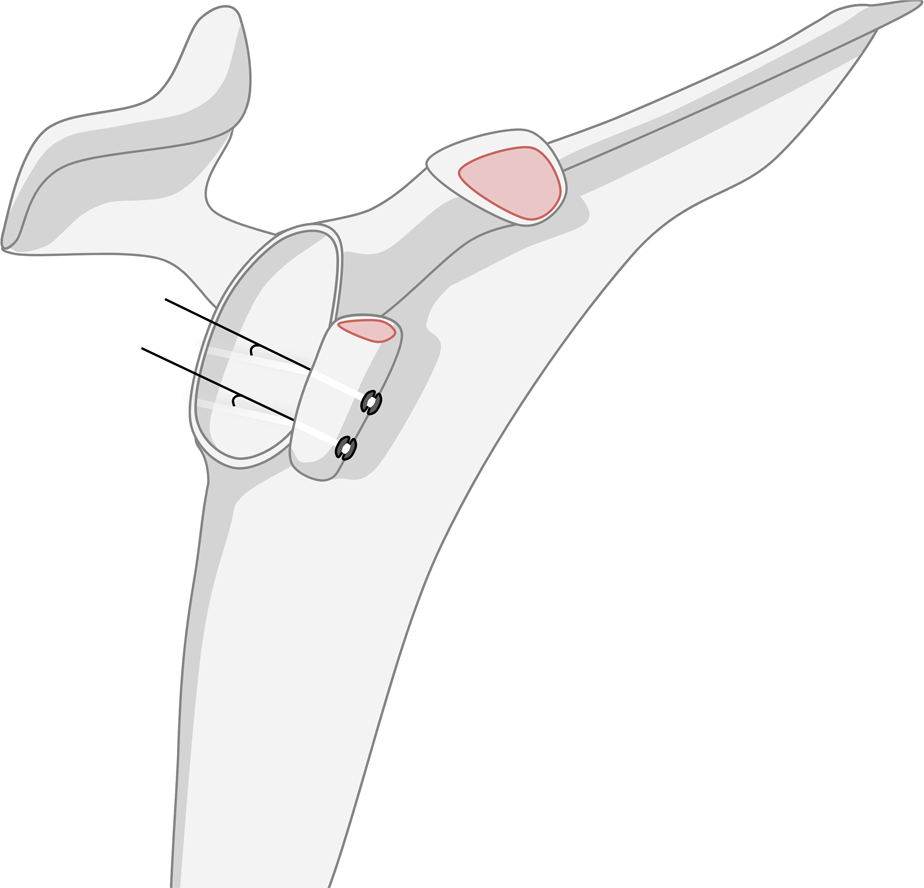
Illustration of a Latarjet construct using suture button fixation. The black line demonstrates the degree of offset at the glenoid-graft interface.
Cortical Augmentation
As the head of the screw contacting the bony graft is responsible for providing resistance to the screw threads within the native glenoid, various methods to augment the graft surface have been studied, including washers, plates, and top hats. Top hats are modified washers with an extended intraosseous collar, penetrating the graft. Overall, 2 such studies have sought to examine these variables. Rabinowitz et al 40 demonstrated that the use of two 3.5-mm partially threaded titanium cannulated screws with top hats or two 3.75-mm fully threaded titanium cannulated screws with a 2-hole wedged-profile plate resulted in a higher mean insertional torque at failure versus two 3.75-mm fully threaded titanium cannulated screws or two 4.0-mm partially threaded stainless steel cannulated screws without cortical augmentation (Appendix Table A1). However, screws with top hats or plates failed by coracoid fracture (50% and 90%, respectively) more so than screws without augmentation (5%). 40 Massin et al 29 recently found that a single 4.5-mm malleolar solid screw with a washer was significantly weaker than two 4.5-mm malleolar screws, a single suture button, and 2 self-compressive screws. Frank et al 19 found that two 4.0-mm screws with a small plate had the highest load at failure, followed by two 3.75-mm screws with a miniplate. While significantly weaker than small plate constructs, all of the double screws with washer groups were significantly stronger than the double screws without washer groups (Appendix Table A1). 19 For failure mechanisms, both groups with a small plate reached the end of testing, while all other constructs experienced a block fracture or crack before test completion. 19
Discussion
The Latarjet procedure is commonly performed for the augmentation of anterior glenoid bony defects and typically utilizes screw fixation to stabilize the graft. Because of complications with screw fixation, alternative nonscrew suture-based constructs have been described with favorable clinical and biomechanical results. 9,20,36 This review found suture button fixation to be biomechanically comparable to screw fixation.
Several studies have sought to address the biomechanical effectiveness of suture button fixation compared to traditional screws. While the biomechanical results are mixed, early clinical outcomes with suture button fixation demonstrated reliable graft placement (90%), similar union rates to screw fixation (>90%), and low intraoperative (3.3%) and postoperative complication (6.8%) rates. 6,10 The displacement rates of suture button constructs presented in this study were greater than those of screw constructs according to 2 of the included studies, which may lead to the conclusion that suture buttons provide less rigid fixation with a greater range of micromotion. 4,41 In addition, a recent systematic review found that screws produce significantly greater ultimate failure loads than suture buttons when under shear forces. 25 Even though these biomechanical findings may suggest otherwise, clinical studies have reported similar union rates when the 2 constructs are compared, and the same review found suture buttons and screws to be comparable under tensile forces. It is possible that the preservation of bone and maximization of the cancellous contact area with the suture button technique, which may be lost because of greater micromotion, increase union rates. 6,46 With these results, it is surprising that a recent survey of fixation methods for glenoid bony augmentation found that only 0.8% of orthopaedic surgeons chose suture button fixation as their preferred method. 47 Although screws are the gold standard of fixation, the benefits of increased construct strength and rigidity must be weighed against hardware complications, leading to revision surgery, which is technically demanding. 54
However, suture button fixation is not without limitations. Suture button fixation, as part of the arthroscopic Latarjet technique, has been associated with a difficult learning curve, with 30 cases that must be performed before reaching an optimal operative time of 76 ± 12 minutes. 10 It is important to note that there have been no reported cases of intraoperative complications after the 10th case, and there have been no postoperative complications reported after the 20th case. 10 If surgeons do elect to proceed with suture button fixation, the use of 2 suture buttons has biomechanically shown to be stronger under inferiorly and superiorly directed forces, which may improve rotational stability. 4 It should not be understated that the traditional use of screws in the Latarjet procedure has served as an important tool for surgeons to address glenoid bone loss. However, it is important to acknowledge new developments in the Latarjet procedure. Suture button constructs have the potential to produce similar, if not improved, outcomes with a lower risk of complications. Future clinical and biomechanical studies should aim to justify these modifications while, at the same time, accounting for both the learning curve and operative time.
Screw position and length are paramount to the success of glenoid reconstruction, as proper coracoid fixation is necessary to withstand forces on the glenohumeral joint and promote graft union. 11 Inaccuracy in screw positioning has been associated with higher complication rates. 2 Surgeons should also take into account screw diameter when performing screw fixation, as increases in the screw diameter can significantly reduce ultimate failure loads. 25 In addition, studies have reported that up to 42% of screws are too long, potentially placing the suprascapular nerve at risk for injuries. 7,23,26 Alternatively, short screws may compromise the stability of graft fixation, which may lead to graft migration or nonunion. 6,7 Nonunion rates of 1.5% to 9.1%, which are associated with continued shoulder instability and technically challenging revision surgery, have been reported with the Latarjet procedure. 18,24,31
This systematic review confirms that 13 commonly used screw types with variable lengths and screw designs (major diameter, shaft diameter, threading, material composition, cancellous/cortical, and solid/cannulated) were able to consistently resist physiological loads when 2 screws were used. This implies that surgeons may choose any screw design of their choice to produce effective biomechanical stability, as long as it is not an absorbable interference screw. 1,29,48,54 To prevent complications associated with posterior screw protrusion, surgeons must consider that unicortical fixation minimizes the risk of soft tissue impingement, but the screw type will determine whether sufficient graft stability is achieved. Screws should be placed at 0° of angulation, as is recommended practice. This technique is easily accomplished with adequate exposure in an open procedure. If 0° is difficult to achieve, 2 screws should be used for fixation, as they performed significantly better compared to a single screw when both were inserted at 15°. 19
Screw breakage and graft fractures are complications of screw fixation with the Latarjet procedure, often resulting in poor clinical outcomes. 7,8,13,49 A biomechanical study included in this review found that, when screw constructs failed, they did so with considerably more damage to the glenoid and graft compared to suture button constructs, resulting in graft fractures and screw cutout. 55 In addition, the failure to apply adequate compression impacts stability and can lead to coracoid osteolysis. 30,33,44 Similarly, osteolysis with the Latarjet procedure may also be the result of the proximal screw shielding from the distal screw because of stress. 43 To avoid these complications, plates and washers have been employed to help distribute the pressure of screw fixation across the graft. The use of such devices led to significantly greater biomechanical strength in terms of contact pressure and loads at failure while avoiding graft fractures or cracks before failure. 19,29,39 Several studies found fixation with 2 screws to be significantly stronger than that with a single screw. 4,19,53 In cases in which there is a lesser degree of bone loss, the use of a cortical augmentation implant may not prevent osteolysis. Di Giacomo et al 15 identified that, in cases with <15% of glenoid loss, the use of a plate had a rate of coracoid osteolysis of 65% compared to only 40% in patients with >15% glenoid loss. 22 This indicates that, aside from the greater biomechanical features and graft protection, cortical augmentation may be more likely to result in graft osteolysis in patients with a lesser degree of glenoid bone loss. Ultimately, the use of cortical augmentation, particularly a small plate with two 4.0-mm screws, has the potential to increase biomechanical strength and clinically allow for earlier rehabilitation. Surgeons should be cautious of fracturing the graft during screw tightening while also being aware of the degree of bone loss.
Limitations
This study is not without limitations. Testing models were composed of variable materials, as studies utilized either synthetic or cadaveric specimens. Among the studies that used synthetic models, the density of materials varied widely from 17 to 30 lb/ft3. For those that used cadaveric specimens, the mean age was older than patients who are typically seen for glenoid reconstruction. 16,34 As a result, the biomechanical data of cadaveric studies may not be generalizable to patients undergoing glenoid reconstruction.
In addition, biomechanical testing protocols varied across studies. During construct assembly, the torque applied to screws was not consistent. Of the 13 studies included in this review, 7 (54%) tightened screws based on “2-finger tightness,” and 3 (23%) did not state how screws were tightened. While “2-finger tightness” is a common practice and appropriate in the operating theater, the torque applied is a subjective measure and introduces another variable to consider. Furthermore, preloading of the construct, axial forces during testing, and the definition of failure varied between protocols. These inconsistencies limited the opportunity to perform a quantitative meta-analysis. A more standardized approach to the measurements would make comparing study results and conclusions more reliable; otherwise, data interpretation becomes convoluted.
Future studies are recommended that clarify fixation strength by creating and utilizing uniform methodology. These studies should focus on undervalued aspects of the Latarjet procedure, such as insertional torque, tensioning of suture-based constructs, screw insertion angle, and bone quality, which are not well established in the literature to date.
Conclusion
Multiple fixation techniques exist for anterior glenoid bony augmentation in the setting of shoulder instability. The present study suggests that a suture button construct can provide comparable strength to screws and serve as an effective alternative, as it may clinically limit hardware-related complications. If screws remain the preferred method, augmentation with a plate may enhance construct strength and avoid graft failure, given that bicortical screws are placed parallel to the articular surface. While these basic science studies provide valuable insights into the biomechanics of graft fixation in the setting of anterior shoulder instability, it is nevertheless important to interpret these results with caution against the inherent variability in study methodology.
Footnotes
Final revision submitted March 28, 2023; accepted April 11, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: E.W.B. has received education payments from Prime Surgical and consulting fees from LinkBio. A.M.M. has received grant support from DJO; education payments from Arthrex, Peerless Surgical, and Prime Surgical; honoraria from Fidia Pharma; and hospitality payments from Smith & Nephew. B.A.P. has received education payments from Prime Surgical; consulting fees from Acumed, DePuy, Smith & Nephew, Stryker, and Wright Medical; royalties from Smith & Nephew, Stryker, and Wright Medical; and honoraria from Fidia Pharma. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethics approval was not required as there were no human subjects requiring informed consent in this article.