
Abstract
Background:
Up to 20% of shoulders with anterior instability are associated with superior labrum anterior-posterior (SLAP) lesions, and they remain untreated after an open Latarjet procedure. SLAP lesions can be responsible for pain and feelings of instability in high-demand patients.
Purpose/Hypothesis:
The aim of this study was to compare the early functional outcomes and return to sport rates in athletes after the Latarjet procedure with versus without associated SLAP lesions. It was hypothesized that untreated SLAP lesions would not influence clinical results.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Inclusion criteria were athletes with anterior shoulder instability treated with Latarjet procedure, a minimum follow-up of 1 year, and an available preoperative computed tomography arthrogram. We recorded patient characteristics; type of sport; bone loss; Rowe, Single Assessment Numeric Evaluation (SANE), and 11-item Disabilities of the Arm, Shoulder and Hand (QuickDASH) scores; 5-point pain and satisfaction scores; reported apprehension; and return to sport. Patients with and without a preoperative type 5 SLAP lesion on imaging were compared.
Results:
Fifty patients were included (mean age, 22 ± 5 years [range, 16-36 years]; mean follow-up, 27 ± 9 months [range, 12-42 months]). Thirty-four patients practiced contact sports, including 20 rugby players. Twelve patients (24%) had a preoperative SLAP lesion. Groups with (+) and without (–) a SLAP lesion were comparable in terms of age, sex, number of instability episodes, type of sport, and glenoid and humeral bone loss. The SLAP+ group had significantly worse outcomes with a lower Rowe score (79 ± 23 vs 91 ± 15; P = .018) and painless rate (50% vs 77%; P = .04). There were no significant differences between the groups in SANE score (SLAP+ vs SLAP–: 80% vs 87%), QuickDASH score (8% vs 8%), return to sport (83% vs 91%), apprehension (79% vs 50%), and reported satisfaction. There was 1 episode of postoperative subluxation in each group.
Conclusion:
Patients who underwent an open Latarjet procedure with an associated SLAP tear more frequently reported postoperative pain than those without a SLAP lesion. Patients with untreated SLAP tears had significantly lower Rowe scores, although SANE score and return to sport were not significantly different between the groups.
The Latarjet procedure is a standard shoulder stabilization technique for the treatment of chronic anterior instability, mainly indicated in cases of off-track lesions, with both glenoid bone loss and Hill-Sachs lesions. 8,10 Clinical results are good, and recurrence rates are low. 20 Indeed, the rate of return to sport is >80%, at 5 months on average, and up to 73% of patients recover before 8 months. 1,21,26 Regarding its effectiveness, some surgeons advocate for Latarjet as the reference technique for all cases of anterior instability, especially in high-risk athletes, even without any bony lesions. 5,11,29
Latarjet is mainly performed as an open surgery. 14,30 A deltopectoral approach is performed, and articular exposure is made through a subscapularis split that provides excellent visibility over the inferior glenoid from 3- to 6-o’clock but limits the access to the superior glenoid. Thus, it does not allow for the diagnosis and treatment of a superior labrum anterior-posterior (SLAP) lesion, so they are usually overlooked and not treated during the procedure.
SLAP lesions, described by Snyder et al 32 in 1990, are a known source of pain and apprehension. 12 A type 5 SLAP lesion is one that is combined with a Bankart lesion. These lesions are present in 20% to 57% of shoulders with anterior instability. 13 When repaired in conjunction with a Bankart lesion, results are comparable to standard Bankart repair without a SLAP tear. 13
The objective of this study was to compare the early functional recovery and return to sports of unstable shoulders with and without SLAP lesions in athletes who underwent an open Latarjet procedure. The hypothesis was that patients with a SLAP lesion would have similar results to patients without SLAP lesions.
Methods
Study Population
This was an institutional review board–approved level 3 retrospective cohort study of patients from a single-surgeon series (A.B.). Patients were included in this study if they (1) had undergone an open Latarjet procedure for unidirectional anterior instability between October 2016 and December 2019; (2) had available computed tomography arthrogram (CTA) Digital Imaging and Communications in Medicine (DICOM) images preoperatively; (3) were high-demand patients practicing at least 1 sport regularly; and (4) had at least 1 year of follow-up. In our institution, we prefer CTA over magnetic resonance imaging, as CTA allows for an accurate evaluation of both bone and labral lesions with thin-slice intervals. Patients were excluded if (1) their native CTA DICOM images were not available or (2) they have had a previous surgery on that shoulder. Two groups of patients, those with versus without a preoperative type 5 SLAP lesion, were created and compared.
Quantification of Bone Defects
Glenoid bone loss was evaluated with a 2-dimensional enface CTA view of the glenoid. It was calculated as the ratio of the width of the defect to the diameter of the assumed outer-fitting circle based on the inferior portion of the glenoid contour, as it has been previously described. 15 On the humeral side, the maximum depth of Hill-Sachs lesions was measured on the axial CTA images and classified in 4 categories: grade 0 (no lesion), 1 (cartilage erosion), 2 (≤1 cm), and 3 (>1 cm) as previously described. 27
Evaluation of SLAP Lesion
The presence of a type 5 SLAP lesion was assessed by a junior surgeon (S.P.) and a senior surgeon (A.B.). A labral lesion extending from a Bankart lesion to the insertion of the biceps on preoperative CTA axial view was considered a positive sign of a type 5 SLAP lesion (Figure 1). Any disagreements were discussed between the junior and senior surgeons until consensus was found for each case. Radiologist reports and data mentioning a SLAP lesion were also collected. The reliability between observers, as well as between surgeon and radiologist findings, was calculated.
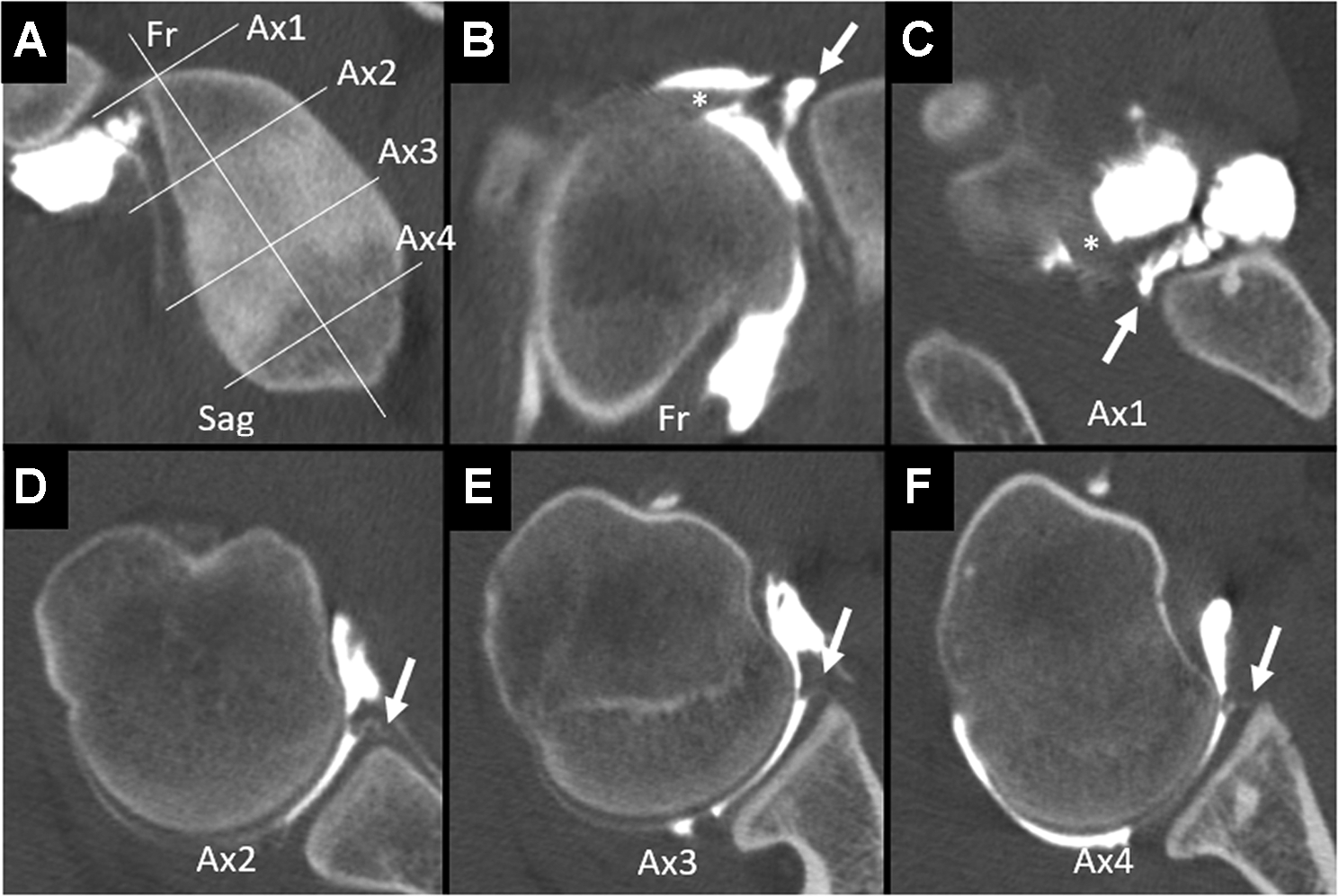
Examples of a type 5 superior labrum anterior-posterior (SLAP) lesion on computed tomography arthrogram with a continuous detachment of the labrum on axial view from the Bankart lesion to the biceps anchor. (A) Sagittal view of the glenoid with location of the frontal and axial slices shown in the examples (B-F). (B) Frontal view centered on the SLAP lesion (arrow) with long head of the biceps tendon (asterisk). (C) Axial view at 12-o’clock showing the long head of the biceps tendon (asterisk) and detachment of the anterior biceps anchor (arrow). (D) Axial view at 2-o’clock showing detachment of the anterosuperior labrum (arrow). (E) Axial view at 3-o’clock showing detachment of the anterior labrum (arrow). (F) Axial view at 4-o’clock showing detachment of the anteroinferior labrum (Bankart lesion) (arrow). Fr, frontal; Sag, sagittal.
Surgical Technique
The coracoid transfer was performed according to Latarjet: bone block was fixated with 2 screws in the lying-down position through a horizontal split in the subscapularis muscle. 34 Capsulotomy was performed horizontally, and the capsule was then repaired with 1 anchor positioned at 3-o’clock, leaving the coracoid graft in an extra-articular position.
Postoperative Rehabilitation
All patients followed a standard rehabilitation protocol and were immobilized in a sling for 4 weeks. Pendulum exercises were allowed from the first postoperative day, and assisted passive motion therapy started at week 2. No active or strength exercises were allowed until full recovery of passive mobility. Return to sport was individualized and permitted between 4 and 6 months after surgery.
Outcome Assessment
Patient-reported outcome measures (PROMs) included the 11-item Disabilities of the Arm, Shoulder and Hand (QuickDASH), Single Assessment Numeric Evaluation (SANE), and Rowe scores. Pain and satisfaction were recorded on a 5-point Likert scale (for pain: 1 = none, 2 = mild, 3 = moderate, 4 = severe, 5 = extreme; for satisfaction: 1 = very unsatisfied, 2 = unsatisfied, 3 = neutral, 4 =satisfied, 5 = very satisfied). Postoperative satisfaction was recorded using a 5-point Likert scale. All postoperative outcomes were collected through an online form filled out anonymously at the final follow-up. Return to sport and level of sports were documented. At the final follow-up, any subjective instability or residual apprehension was also specifically requested.
Statistical Analysis
Statistical analysis was carried out using the R V4.1.1 software (2021; The R Foundation for Statistical Computing). Interobserver reliability for evaluation of SLAP lesions was calculated by Pearson test and reported as intraclass correlation coefficients (ICCs). For evaluation of the study groups, means and standard deviations were reported for continuous variables, and categorical variables were reported as absolute and relative frequencies. The Student t test was used to compare continuous variables. A pooled-variance t test was used to compare functional scores of groups with different sample sizes and increase statistical power. Categorical variables were compared using a pairwise comparison proportion test. P < .05 was considered statistically significant.
Results
Of 116 patients initially reviewed, 62 did not meet the inclusion criteria and were excluded: 58 patients did not have an available preoperative CTA, and 4 patients did not practice at least 1 sport regularly. Four patients, all without a SLAP tear, were lost to follow-up at 1 year. The final study population included 50 patients, 44 men and 6 women. There were 12 patients with a SLAP lesion (SLAP+ group; 11 men) and 38 patients without a SLAP lesion (SLAP– group; 33 men) (Figure 2).
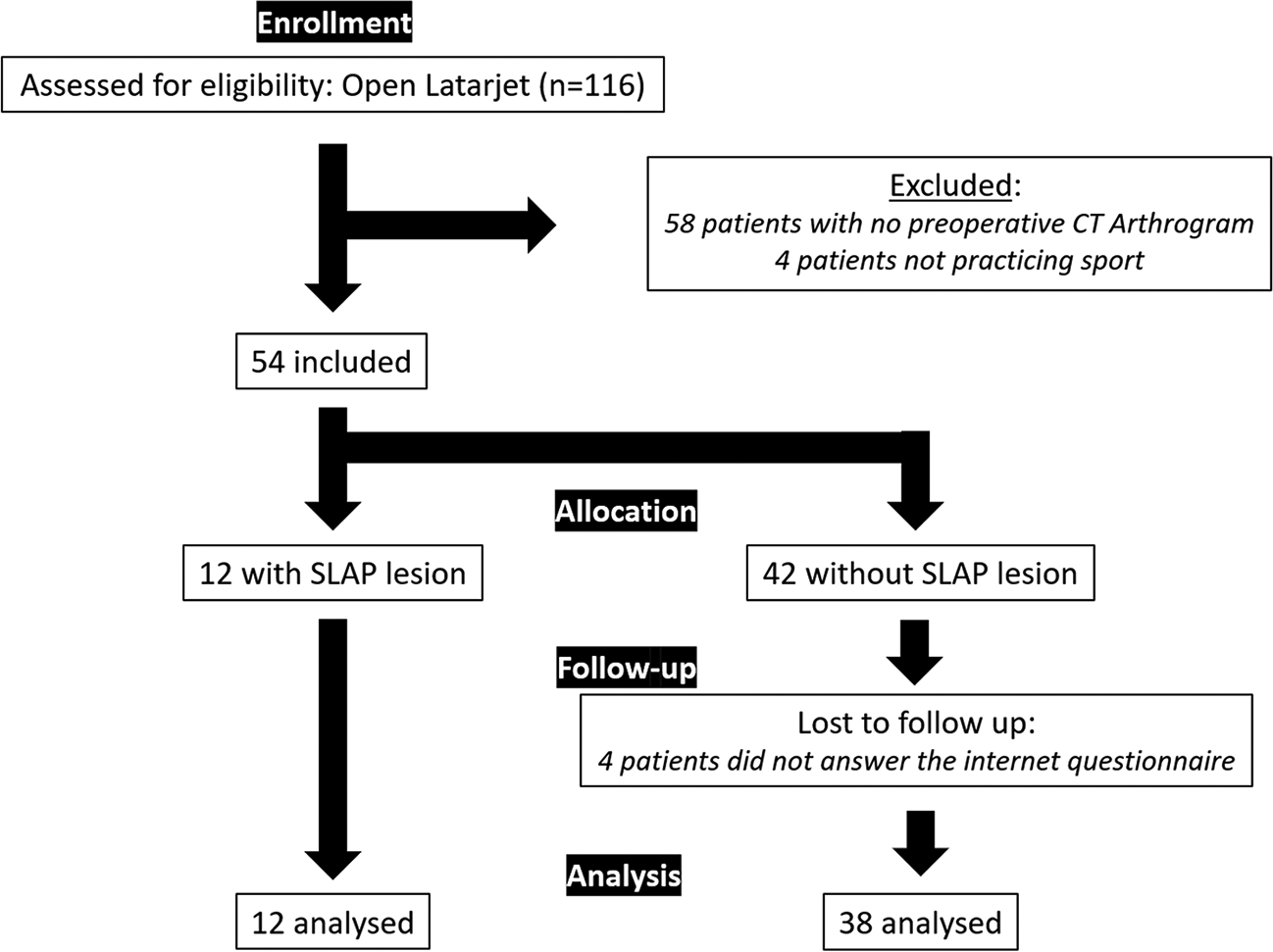
Flowchart of patient inclusion in the study.
The mean age of the overall study population at the time of surgery was 22 ± 5 years (range, 16-36 years). Before surgery, 4 patients experienced 2 dislocations (including subluxations), 28 patients had 3 to 5 episodes, 16 had >5 episodes, and 2 patients had >10 episodes. Mean time to surgery from the first dislocation was 25 ± 27 months (range, 1-131 months). Mean follow-up was 27 ± 9 months (range, 12-42 months). None of the patients required revision surgery. The characteristics of the study population are summarized in Table 1.
Patient Characteristics a
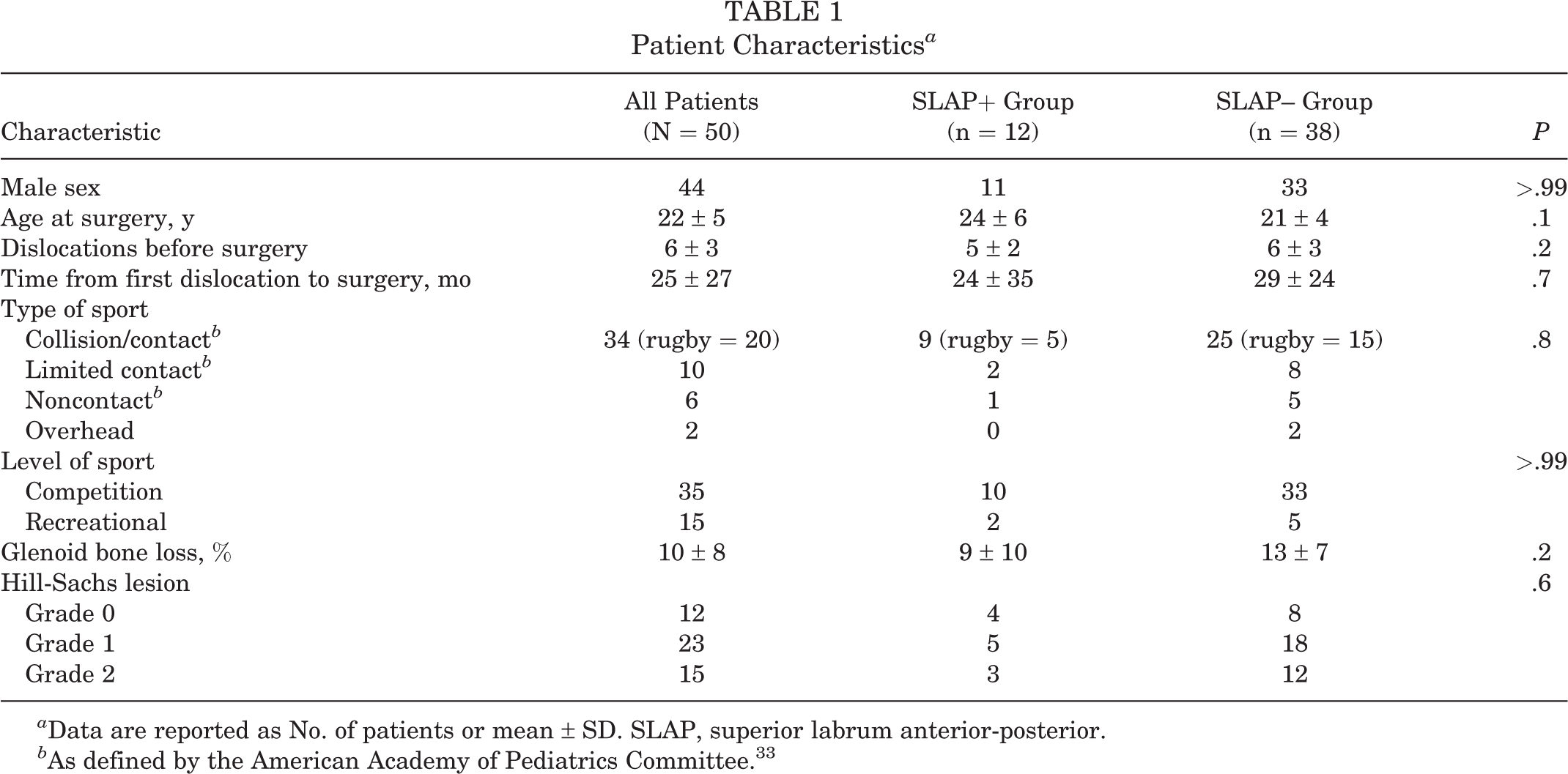
a Data are reported as No. of patients or mean ± SD. SLAP, superior labrum anterior-posterior.
b As defined by the American Academy of Pediatrics Committee. 33
The ICC values indicated 89% agreement between the junior and senior surgeons’ diagnosis and 83% agreement between the radiologists’ and surgeons’ diagnosis. Twelve patients (24%) were diagnosed with a type 5 SLAP lesion on preoperative CTA by surgeons’ agreement, of which 8 cases only had been previously reported by radiologists. Both study groups had comparable demographics for age, number of dislocations before surgery, and time to surgery from the first episode. Thirty-four patients practiced a collision/contact sport (SLAP+: 9 patients, SLAP–: 25 patients; P = .8), and 20 were rugby players (SLAP+: 5, SLAP–: 15; P > .99). One failure (subluxation, no dislocation) was reported in each group at the final follow-up.
Mean glenoid bone loss was 10% ± 8% (range, 0%-30%): 9% in the SLAP+ group and 13% in the SLAP– group (P = .2). Hill-Sachs lesion was reported in 37 cases (23 grade 1, 15 grade 2). The SLAP+ group included 8 Hill-Sachs lesions (5 patients with grade 1, 3 patients with grade 2) and the SLAP– group 30 lesions (18 grade 1, 12 grade 2). There was no statistical difference between groups for number of Hill-Sachs lesions (P = .6).
Outcome data are shown in Table 2. At final evaluation, mean Rowe score was 88 ± 18 (range, 25-100): 79 in the SLAP+ group versus 91 in the SLAP– group (P = .018) (Figure 3A). The power of the 2-samples t test was estimated at 63%. The mean QuickDASH score was 8% (0-55 ± 12) and was similar in both groups. Mean SANE score was 85% (30-100 ±15): 80% in the SLAP+ group versus 87% in the SLAP– group (P = .15) (Figure 3B). Mean satisfaction was 4.6 of 5 and similar in both groups.
Assessment of Outcomes a
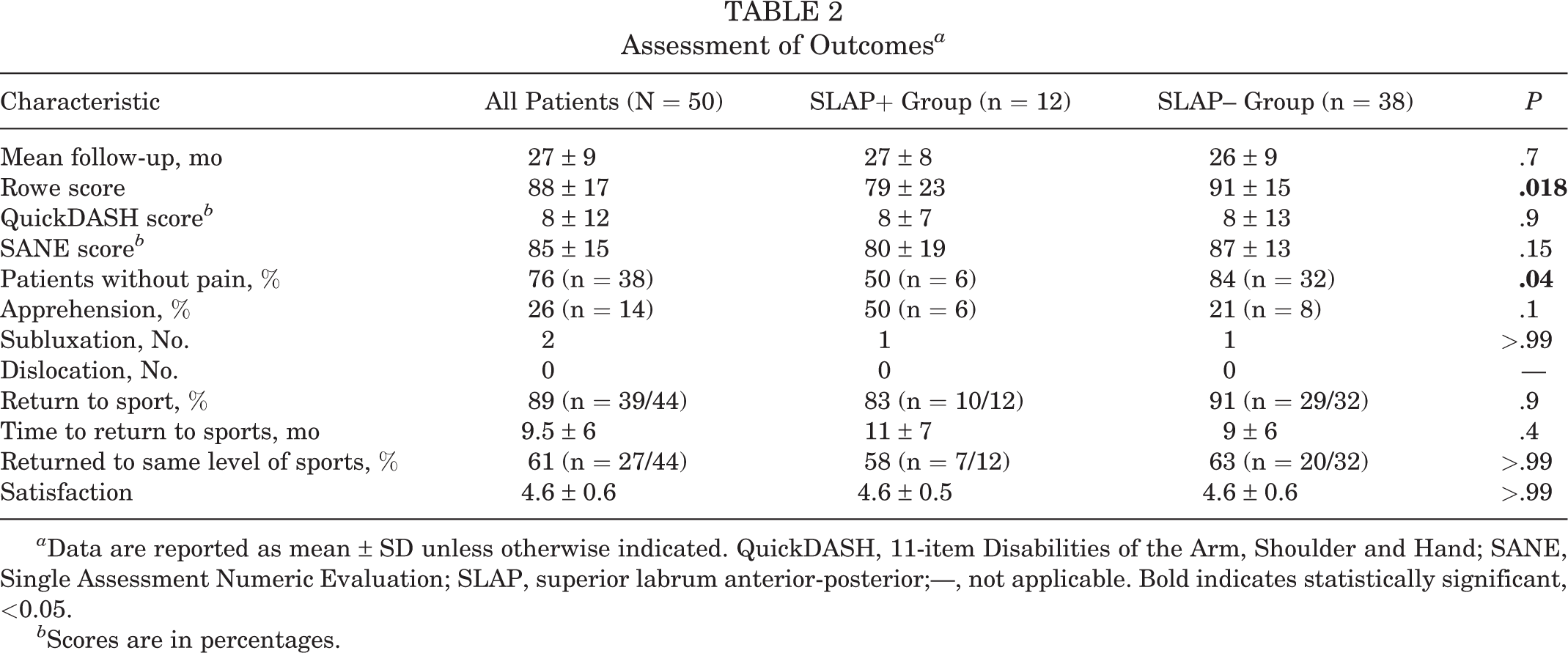
a Data are reported as mean ± SD unless otherwise indicated. QuickDASH, 11-item Disabilities of the Arm, Shoulder and Hand; SANE, Single Assessment Numeric Evaluation; SLAP, superior labrum anterior-posterior;—, not applicable. Bold indicates statistically significant, <0.05.
b Scores are in percentages.

Comparison of (A) Rowe scores and (B) Single Assessment Numeric Evaluation (SANE) scores between patients with a superior labrum anterior-posterior (SLAP) lesion (SLAP+) and those without a SLAP lesion (SLAP–). The black line indicates the median value, and the circles are outliers. The whiskers indicate minimum and maximum, shaded box indicates fisrt and third quartiles. The Rowe score was significantly lower in the SLAP+ group (P = .018). The SANE score was not significantly different between the groups (P = .15).
Overall, painless rate was 76% (n = 38), and persistent apprehension was reported in 28% of cases (n = 14). Patients without a SLAP lesion more frequently reported no pain (84% in the SLAP– group vs 50% in the SLAP+ group; P = .04) (Figure 4A). In the SLAP+ group, 6 patients reported no pain, and 6 stated mild pain. In the SLAP– group, 32 patients reported no pain, 8 had mild pain, and 4 had moderate pain. Six patients (50%) felt residual apprehension or instability in the SLAP+ group and 8 patients (21%) in the SLAP– group (P = .1) (Figure 4B).

Comparison of (A) residual pain and (B) residual apprehension between patients with a superior labrum anterior-posterior (SLAP) lesion (SLAP+) and without a SLAP lesion (SLAP–). The difference in proportion of residual pain between the SLAP+ and SLAP– groups was statistically significant (50% vs 16%, respectively; P = .04). The difference proportion of residual apprehension between the SLAP+ and SLAP– groups was not significant (50% vs 21%, respectively; P = .1).
Five patients (2 [17%] in the SLAP+ group and 3 [7%] in the SLAP– group) were not able to return to sports because of their shoulder, and 6 patients in group 2 did not return to sports for other reasons. Excluding patients who did not return to sports for other reasons than their shoulder, overall return to sport rate was 89% (n = 39/44). It was lower in the SLAP+ group (83%, n = 10/12) than in the SLAP– group (91%, n = 29/32) without statistical difference (P = .9). Return to sport occurred on average at 9.5 months postoperatively (2-31 ± 6): 11 months (3-21 ± 7) in the SLAP+ group and 9 months (2-31 ± 6) in the SLAP– group (P = .4). General rate for return to sport at the same level was 61% (n = 27/44): 58% in the SLAP+ group (n = 7/12) and 63% in the SLAP– group (20/32) without statistical difference (P > .99).
Discussion
Patients with SLAP had significantly lower Rowe scores and less often reported a painless shoulder after Latarjet. Other outcome measures were not statistically significant. The Latarjet procedure does not allow for visualization and treatment of SLAP lesions, which are usually overlooked. To our knowledge, this is the first study to investigate the consequences of an associated SLAP lesion after open Latarjet. There are few reported cases of revision for treatment of SLAP lesions after open Latarjet. 9,16 Therefore, our initial hypothesis was that an untreated SLAP lesion would not worsen outcomes after Latarjet. Surprisingly, our results suggest that an untreated SLAP lesion is a risk factor of lower Rowe scores and a less frequent pain-free shoulder.
The Rowe score is a specific score for shoulder instability, including pain, apprehension, mobility, and activities. It was lower in the SLAP+ group by 12 points, which is a larger difference than the minimal clinically important pre- to postoperative difference for the Rowe score of 9.7 points. 28 Other outcome measures, such as SANE score, QuickDASH, apprehension, satisfaction, and return to sport, were not significantly different.
Patient characteristics and results (age, number of instability episodes, time before surgery, and bone lesions) were comparable to other publications in anterior shoulder instability. 20 There was no statistical difference between our 2 groups for these parameters. This suggests that the presence of a SLAP lesion in unstable shoulders is independent of these risk factors. Sports type was not statistically associated with the presence of a SLAP lesion, and there were no more overhead athletes in the SLAP+ group than in the SLAP– group. The overall Rowe score was 88, which is comparable to other publications in the literature. 20 Residual apprehension was reported in 28% of our cases. Other studies based on patient-reported outcomes described also high apprehension rates, from 20% to 41%. 5,19 Thirty-four percent of the patients of the current study had some kind of residual pain, mild in almost all of them. Bessiere et al 5 also observed a high 38% rate of pain after Latarjet. Hardy et al 17 and Baverel et al 4 also reported frequent pain, with a mean visual analog scale pain score >1 after Latarjet. However, this rate rose up to 50% in our SLAP lesion group. Recurrence rate in our case series was 0% for dislocation and 4% for subluxation, which is low compared to the literature, but it may increase with longer follow-up. Overall return to sport rate was 89%, which is good and comparable to other publications. 21
Arthroscopy is considered the gold standard for SLAP lesion diagnosis. Clinical examination offers poor predictive values for the correct diagnosis of SLAP lesions. 23 Imaging studies show satisfactory performances, especially imaging with articular opacification, such as CTA with a sensitivity and specificity of nearly 90%. 2,3,24 Along with anterior labrum tear, reported SLAP incidence ranges from 27% to 50% 13 and is comparable to our study, with 12 SLAP lesions out of the 54 patients initially selected (22%). Radiologists’ reports described a SLAP lesion in 8 of the 12 cases; they were all obvious cases of SLAP lesions. For the other 4 cases, imaging was more subtle, and they remained unreported even though radiologists specialized in musculoskeletal disorders. There are no precise criteria for diagnosing type 5 SLAP lesions on CTA imaging. In this study, the diagnosis of these lesions was considered positive whenever a labral detachment was seen continuously from the Bankart lesion to the long biceps insertion. We reported on radiologist findings because frequently, patients ask what a SLAP lesion is after reading their report and how it will be treated. Also, the surgeon has to explain that it will remain untreated after Latarjet, even though imaging often has false-positive diagnoses, especially when contrast is used. 31
Regarding treatment of the SLAP lesion combined with instability, data are missing about untreated SLAP lesions. All Bankart repair series report good results after combined treatment of the SLAP lesion, 13 being similar for patients with treated SLAP lesions and patients without SLAP lesions. Only Hogan et al 18 describe a lower return to sport at the same level for combined SLAP and Bankart repair. To our knowledge, no study has yet evaluated the role of an untreated SLAP lesion after shoulder stabilization. Ideally, unstable patients with treated and untreated SLAP lesions should be prospectively compared for stronger evidence. In this study, all SLAP lesions were untreated due to the surgical technique characteristics. In addition, we cannot compare our results with other published series on type 5 SLAP lesions because none of them use the Latarjet procedure. More research should be conducted on this topic.
Finally, it is unclear if revision should be performed on patients with SLAP lesions who have residual feelings of pain or instability after an open Latarjet. Our study was not designed to answer this question. To date, no patient has been revised, but it is reasonable to believe that treatment of a neglected symptomatic SLAP lesion will improve the outcomes. Future studies are required to answer this question. However, based on these findings, author recommendations are now to privilege arthroscopic Bankart repair over Latarjet in the presence of a combined SLAP lesion if possible (on-track lesions) or to look for an untreated SLAP lesion for patients with residual pain or apprehension after an open Latarjet. Patients scheduled for Latarjet with a SLAP lesion on CTA are also warned of possible residual pain or instability feelings. Arthroscopic Latarjet for trained teams or a combined procedure with arthroscopic SLAP repair and open Latarjet could be other alternatives.
Limitations
There are several limitations to our study: (1) SLAP tears were not confirmed by arthroscopy or direct visualization. CTA has shown good reliability as mentioned above, but we disagreed with the radiologist interpretations on one-third of the SLAP tears. This suggests that we may have false positives. (2) The SLAP lesion group is limited in number, but the pooled-variance t test increased statistical power for different-size group comparison. Group standard deviations were close, and global Rowe score mean and standard deviation were comparable to data in the literature. 4,22,25 Therefore, a pooled-variance t test seemed appropriate. Statistical power is estimated at 63% in our study. Power calculation to reach 80% showed that inclusion of 80 patients would be required considering a 1:3 ratio of SLAP lesions. (3) In addition, this study is a retrospective study based on PROM, and some questions were based on patients’ memory, so subjectivity and loss of precision may be possible. An advantage of PROM is that all patients went through the same protocol and online questionnaire, reducing evaluator bias. (4) Our inclusion criteria included only unstable athletes playing at least 1 sport regularly. We limited inclusion to high-demand patients in whom persistence of pain or apprehension would be disabling. More research on patients with less demanding characteristics should be conducted. (5) We included patients with a minimum of 12 months’ follow-up. Several other studies with shoulder instability also included patients with a minimum of 12 months’ follow-up, 21 because this period is long enough for giving early functional results and return to sports data, which was our first objective; however, it is insufficient to evaluate recurrence rates, but this was not our main concern in this study. Latarjet is known to provide early recovery within the first year, 1,6 and bone graft consolidation rate ranges from 70% to 100% within 6 months postoperatively. 7 After 12 months, persistence of pain or difficulties is usually a major concern for high-demand patients and worth being analyzed at this stage.
Conclusion
Patients undergoing an open Latarjet procedure with an associated SLAP tear more frequently reported postoperative pain than those without a SLAP lesion. Patients with untreated SLAP tears also had significantly lower Rowe scores, although SANE score and return to sport were not significantly different.
Footnotes
Final revision submitted January 30, 2023; accepted February 13, 2023.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Clinique du Sport (No. 02-2020.5).