
Abstract
Background:
Management of glenohumeral instability in the adolescent population can be both challenging and controversial. There are no current guidelines for optimal management of glenohumeral instability in this population (unidirectional or multidirectional), and the cutoff ages for transition to adult treatment are not known.
Purpose:
To develop consensus-based guidelines for the management of glenohumeral instability in adolescents.
Study Design:
Consensus statement.
Methods:
A 26-question, multiple-choice survey was developed after 2 rounds of iterations and was submitted to the orthopaedic surgeons of the Pediatric Research in Sports Medicine (PRiSM) Society. The survey comprised 3 sections—demographics, practice setting, and decision-making—and included cutoff ages and management in 5 specific case scenarios. Consensus-based guidelines were generated with 66% response agreement. An indication score was then applied to each response related to more aggressive management to determine if variables related to consensus (or lack thereof) could be identified.
Results:
A total of 54 responses were returned. Of the respondents, 59% were from academic practice, 84% were pediatric orthopaedic fellowship trained, and 46% performed >25 shoulder instability cases per year. In the setting of first-time anterior shoulder dislocation, nonoperative treatment was preferred for boys aged <14 years and girls aged <13 years. Besides age, proximal humerus physeal status, injury mechanism, sport, and presence of bony injury affected treatment selection. The presence of a Bankart lesion was an indication for stabilization in first-time dislocations for contact athletes with a closing or closed physis, but not in patients with an open physis or noncontact injury mechanisms. For recurrent anterior shoulder dislocation, stabilization was preferred irrespective of physis status. Initial nonoperative treatment was preferred for multidirectional instability.
Conclusion:
In the setting of first-time anterior shoulder dislocation in patients with open physes, nonoperative treatment was preferred for boys <14 years and girls <13 years. Future multicenter prospective studies focusing on outcomes would help to validate current practice patterns, especially in scenarios for which no consensus was reached.
Glenohumeral instability is a common source of pain and disability, with an incidence of 11 to 24 per 100,000 person-years in the general population.12,44,46,55 The incidence is approximately 10 times higher in adolescent boys participating in contact sports, at 165 per 100,000 person-years. 33 Management of shoulder instability in the adolescent population is both challenging and somewhat controversial. Patients aged 12 to 18 years are at higher risk for recurrence compared with adult counterparts, with both nonoperative and operative treatment.11,29,42,47
One of the challenges of treating adolescent glenohumeral instability is the relative paucity of high-level clinical outcome data in this age group. Treatment recommendations are in part based on extrapolations from high-quality data in the young-adult population where the role of surgical treatment in recurrent instability is better studied. In skeletally mature patients, both arthroscopic and open stabilization procedures are effective in reducing the risk of recurrent instability, and in some cases early surgical treatment may be more cost-effective.3,9,10,18,22 An Instability Severity Index Score has been validated for use in clinical decision-making regarding surgical treatment.7,38
There is growing recognition that adolescent glenohumeral instability has a distinct risk profile, a higher rate of atypical presentation, and different risk factors for recurrent instability compared with adult counterparts. The role of age in predicting recurrent instability is not clear; early studies suggested that the youngest patients were at highest risk for recurrence, while more recent publications suggest that adolescents aged 14 to 18 years are at higher risk than both older and younger patients.27,35,37,39 Adolescent patients have a distinct profile of risk factors for recurrence, including open physes, decreased glenoid retroversion, and higher rates of atypical injuries such as anterior labroligamentous periosteal sleeve avulsions and off-track Hill-Sachs lesions.11,28,32,54
Despite a growing number of studies published on the subject, no standardized algorithm exists for evaluation and management. Therefore, potential controversy exists regarding the best approach to treat adolescents with glenohumeral instability. The purpose of this study was to establish consensus among age-specific specialists for the management of glenohumeral instability in adolescent patients.
Methods
This study was held in conjunction with the Pediatric Research in Sports Medicine (PRiSM) Society’s Shoulder Instability Research Interest Group (RIG). PRiSM is a health care society based in the United States whose members include athletic trainers, sports medicine physicians, physical therapists, surgeons, researchers, radiologists, nutritionists, nurse practitioners, and sports psychologists. PRiSM’s goal to advance pediatric sports medicine research is achieved primarily through their RIGs, which focus on various disciplines. For the current study, a 26-question, multiple-choice survey was developed after 2 rounds of iterations by 2 members of the PRiSM Shoulder Instability RIG (C.W.N. and S.N.P.). The survey was distributed to the remaining RIG members to complete, and results were then discussed among all members of the RIG to determine which questions needed revision. The process was repeated with the second draft of the survey. After 2 rounds of edits, the investigators were satisfied with the questions and response options and sent the survey to the PRiSM Society at large.
The survey (Supplemental Material) comprised 3 sections: (1) respondent’s demographics and practice setting (5 questions), (2) variables affecting the decision-making process including cutoff ages (1 question), and (3) management of 5 specific case scenarios (20 questions). Case scenarios focused on the consideration of several variables in recommending treatment for anterior glenohumeral instability, including age, physeal status, mechanism of injury, and number of dislocations. Similar case scenarios were included using the same methodology for multidirectional instability (MDI) to discern if this diagnosis itself changed management recommendations. For the purposes of the survey, an open surgery was considered to be open Bankart repair with capsular shift and not inclusive of bony augmentation (Latarjet procedure).
The survey was built in REDCap and was sent via email to orthopaedic surgeons of the entire PRiSM Society (131 surgeon members) on May 24, 2022. A follow-up email was sent July 2022. Based on a previously published study with similar methodology, consensus-based guidelines were generated when at least 66% of the respondents agreed. 34 For survey questions in which no consensus was reached, an analysis of the demographic factors was assessed for any factors that individually contributed to the lack of consensus.
To further analyze the respondents’ likelihood to recommend surgical treatment for shoulder instability or to recommend a specific surgical procedure during operative treatment, 3 subscores were created for each respondent by summing the number of times they recommended surgery: an Open Indication Score, Anterior Indication Score, and MDI Indication Score. These 3 subscores may be considered a measure of the respondents’ willingness to recommend surgery, or to recommend an open surgical procedure instead of an arthroscopic procedure, in clinical practice. The Open Indication Score summarizes the 14 responses to questions based on 6 clinical vignettes for which an open surgical approach was an answer option, taking an ordinal value from 0 (never recommended open surgery) to 6 (always recommended open surgery). The Anterior Indication Score summarizes the 9 responses to the 4 clinical vignettes in the anterior shoulder instability section (cases 1-4), taking an ordinal value from 0 (never recommended surgery) to 9 (always recommended surgery). The MDI Indication Score summarizes the 5 responses to the 2 clinical vignettes in the MDI section, taking an ordinal value from 0 (never recommended surgery) to 5 (always recommended surgery).
Statistical Analysis
Basic descriptive statistics are reported as counts and percentages. When consensus was not reached, responses were compared using demographic data with Pearson chi-square to find associations between respondents and their answers. The Kruskal-Wallis H test was performed to test the indication subscores against survey respondent demographic factors. If there was a significant finding, then a pairwise comparison with Mann-Whitney U test was performed with Bonferroni correction to identify the demographic categories that were different from one another. Statistical analysis was conducted using SPSS (Version 28; IBM Corp). No a priori power analysis was performed. Statistical significance was defined as P < .05.
Results
Survey Respondents
Of the 131 surgeon members of the PRiSM Society who received the survey, 54 (41%) completed it. The characteristics of the survey respondents are summarized in Table 1. All respondents were fellowship-trained orthopaedic surgeons, with most (43%) reporting fellowship training in pediatric orthopaedics, followed by fellowship training in both pediatric orthopaedics and sports medicine (41%). Most respondents (54%) reported performing <25 shoulder stabilization surgeries annually, and most (59%) practiced in an academic setting. The distribution of practices across the United States was even, and no respondents practiced outside of the United States. Ten respondents (19%) had practiced for <5 years, 16 (30%) reported 6 to 10 years in practice, 13 (24%) reported 11 to 15 years in practice, and 15 (28%) reported >15 years in practice.
Characteristics of the Survey Respondents

Factors Associated With First-Time Anterior Dislocation
Respondents were asked whether a range of factors would influence their treatment decision for first-time anterior shoulder dislocations. A majority of respondents indicated that age (70%), presence of bony Bankart lesion (94%), mechanism of injury (70%), and sport/position played (76%) would influence their treatment decision to recommend surgical versus nonoperative treatment for a first-time anterior shoulder dislocation. Consensus was achieved for preferred nonoperative management of first-time anterior shoulder instability in male patients aged <14 years and female patients aged <13 years, with 67% of respondents each. A minority of respondents reported that their treatment decision for first-time shoulder dislocation would be influenced by patient sex (30%) or the presence of open physes (19%).
Radiological Evaluation in First-Time Anterior Dislocation
Respondents indicated a preference for magnetic resonance imaging (MRI) in addition to plain radiographs in the evaluation of first-time dislocation. Overall, 46% indicated a preference for magnetic resonance arthrography (MRA), while 26% preferred MRI scans obtained with a 3-T magnet and 9% preferred MRI scans obtained with a 1.5-T magnet. One respondent (2%) preferred computed tomography (CT) for evaluation of first-time dislocation. Finally, 20% of respondents indicated that they did not routinely obtain advanced imaging for evaluation of first-time dislocation. Respondents were not allowed to choose multiple advanced imaging techniques (eg, CT and MRA).
Treatment Consensus
For first-time anterior dislocation, there was a consensus recommendation in favor of nonoperative treatment for patients with open physes and noncontact injury mechanism (83% of respondents) (Table 2). However, there was no consensus for treatment recommendation in patients with open physes and a contact injury mechanism (40% favoring arthroscopic stabilization and 60% recommending nonoperative treatment) (Table 3). There was no consensus for the 2 scenarios of patients with closed or closing physes and a noncontact injury mechanism. Depending on the scenario, 50% to 57% of respondents preferred arthroscopic stabilization while 43% to 50% favored nonoperative treatment. However, there was a consensus recommendation in favor of operative treatment for first-time dislocation with closed or closing physes and a contact injury mechanism (with 69% of respondents favoring arthroscopic stabilization).
Consensus for Treatment Recommendations for Clinical Vignettes a
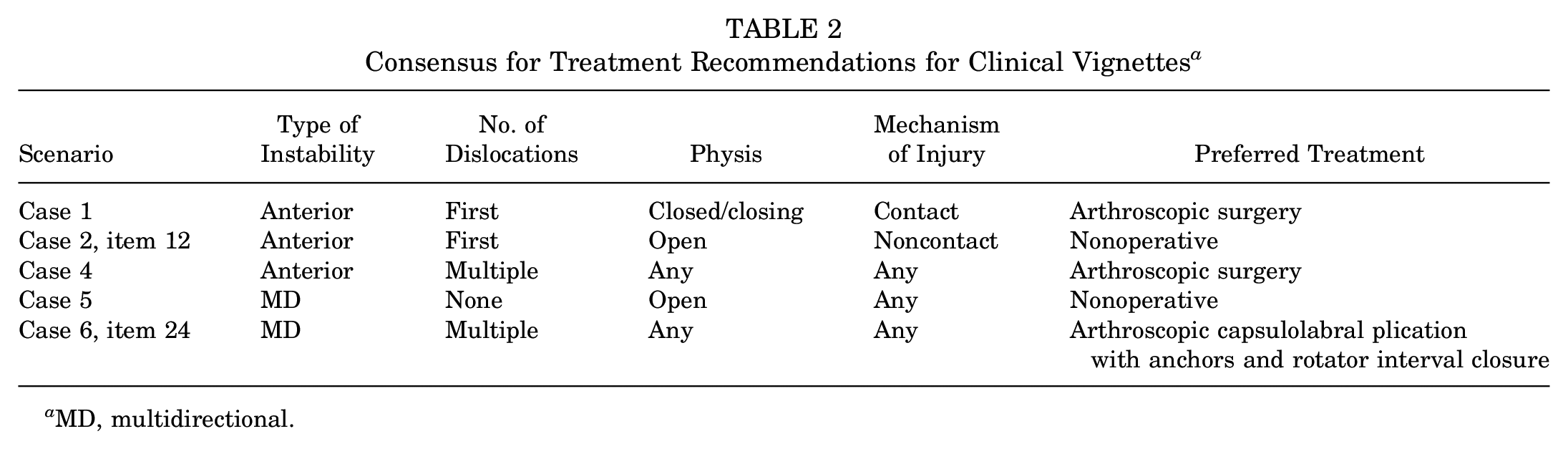
MD, multidirectional.
Lack of Consensus for Clinical Vignettes a
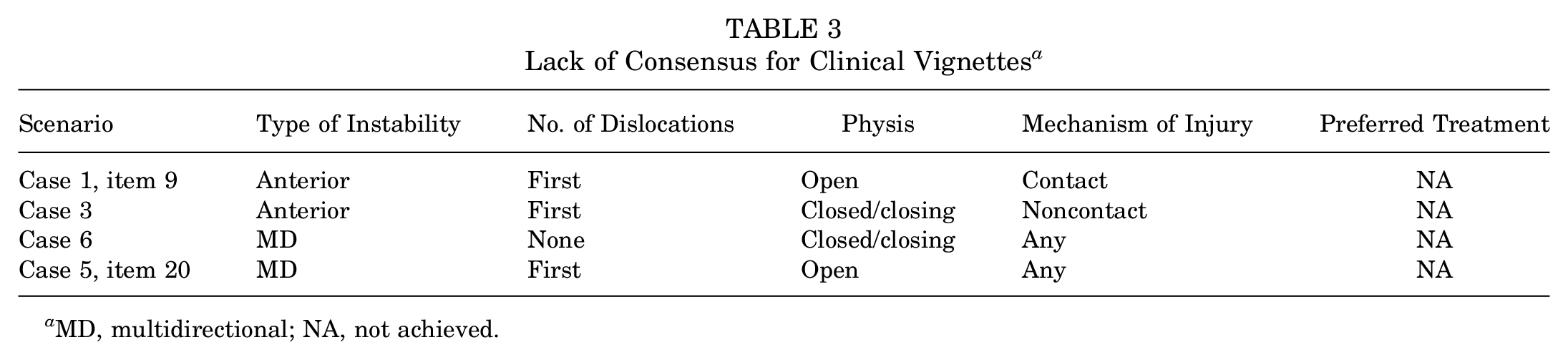
MD, multidirectional; NA, not achieved.
For patients with recurrent anterior dislocations, there was a consensus recommendation for arthroscopic stabilization regardless of physeal status or mechanism of injury. The vignette did not mention the presence or absence of glenoid bone loss. Of the respondents, 88% recommended arthroscopic surgery and 9% recommended open surgery, while only 3% recommended nonoperative treatment.
For MDI, there was consensus based on physeal status and number of dislocation events. There was a consensus recommendation in favor of nonoperative treatment of patients with symptomatic MDI with no history of frank dislocation, open physes, and a normal MRI/MRA scan (with 67% of respondents recommending nonoperative treatment and 31% recommending arthroscopic surgery). However, for patients with symptomatic MDI with no frank dislocations and closed or closing physes, there was no consensus for treatment (56% recommended surgery [50% arthroscopic, 6% open], and 44% recommended nonoperative treatment). This lack of consensus persisted in the scenario with a patient with MDI with a single dislocation episode and open physeal status, as 60% recommended surgery (54% arthroscopic, 6% open) and 41% recommended nonoperative treatment.
For patients with symptomatic MDI and history of multiple dislocations, there was a consensus recommendation for arthroscopic stabilization regardless of physeal status or mechanism of injury. The vignette did not mention the presence or absence of glenoid bone loss. Arthroscopic stabilization was recommended by 83%, open surgery by 13%, and nonoperative treatment by 4%. There was consensus regarding the surgical technique, with 83% recommending arthroscopic capsulolabral plication with suture anchors and 98% recommending rotator interval closure.
Factors Associated With Lack of Consensus
There was a relationship between the treatment recommendations for first-time anterior dislocations in female patients with closing growth plates and the surgeon’s years in practice (P = .042), with 80% of respondents in practice for <5 years opting for nonoperative treatment, as opposed to 77% of respondents in practice for 11 to 15 years recommending arthroscopic stabilization. Surgeons with 6 to 10 years in practice recommended arthroscopic treatment 56% of the time, and surgeons with >15 years in practice recommended arthroscopic treatment 40% of the time. None of the respondents recommended open treatment.
There was a relationship between recommendation for open treatment and recurrent anterior instability in male patients with closed physis and the surgeon’s years in practice (P = .039). Surgeons with >15 years in practice recommended open treatment 27% of the time, while surgeons with <15 years in practice recommended open surgery 3% of the time. There were no other surgeon demographic factors related to treatment recommendations among survey items without a consensus response.
Assessment of Indication Scores
Table 4 shows the distribution of Open Indication Scores according to surgeon characteristics. There were significant differences in Open Indication Scores according to the surgeon’s years in practice or years of experience (YOE) (P = .017); however, this association appeared to be weak, as none of the pairwise comparisons were found to be significantly different from each other (P > .2). Practice type, fellowship type, practice location, and cases per year were unrelated to the Open Indication Score.
Distribution of the Open Indication Score by Surgeon Characteristics a
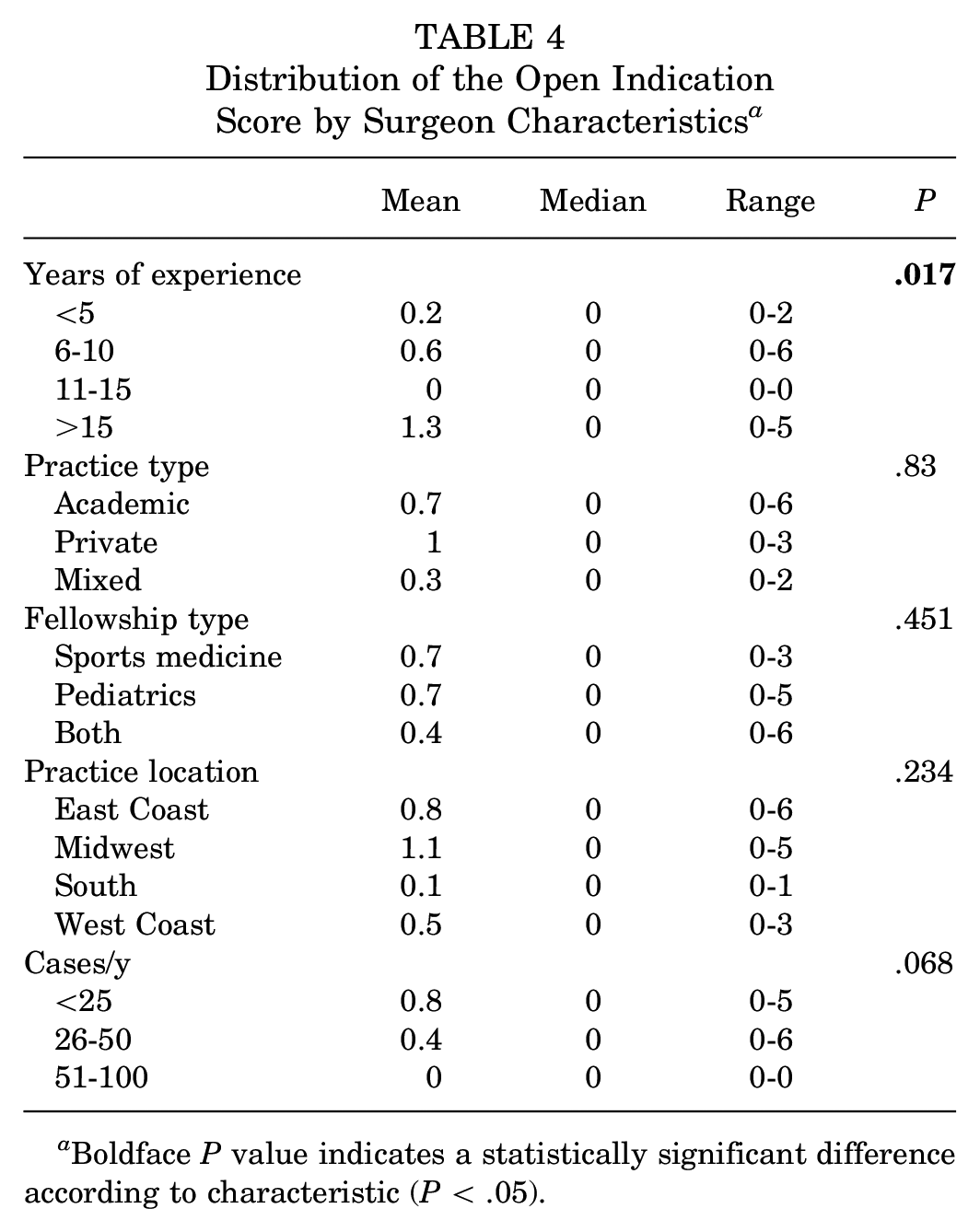
Boldface P value indicates a statistically significant difference according to characteristic (P < .05).
The Anterior Indication Score appeared to be associated with a private practice setting, as private practice had a higher Anterior Indication Score than academic practice types (P = .027) (Table 5). The academic and mixed groups were similar (P = .156) to each other. Because of the low number of surgeons in private practice (n = 3), the private practice and mixed groups were combined, and the analysis was repeated. When combining private practice and mixed practice, the academic practice had a significantly lower Anterior Indication Score than the combined group (P = .013). In contrast to the Open Indication Score, experience seems to be unrelated to the Anterior Indication Score (P = .241).
Distribution of the Anterior Indication Score by Surgeon Characteristics a
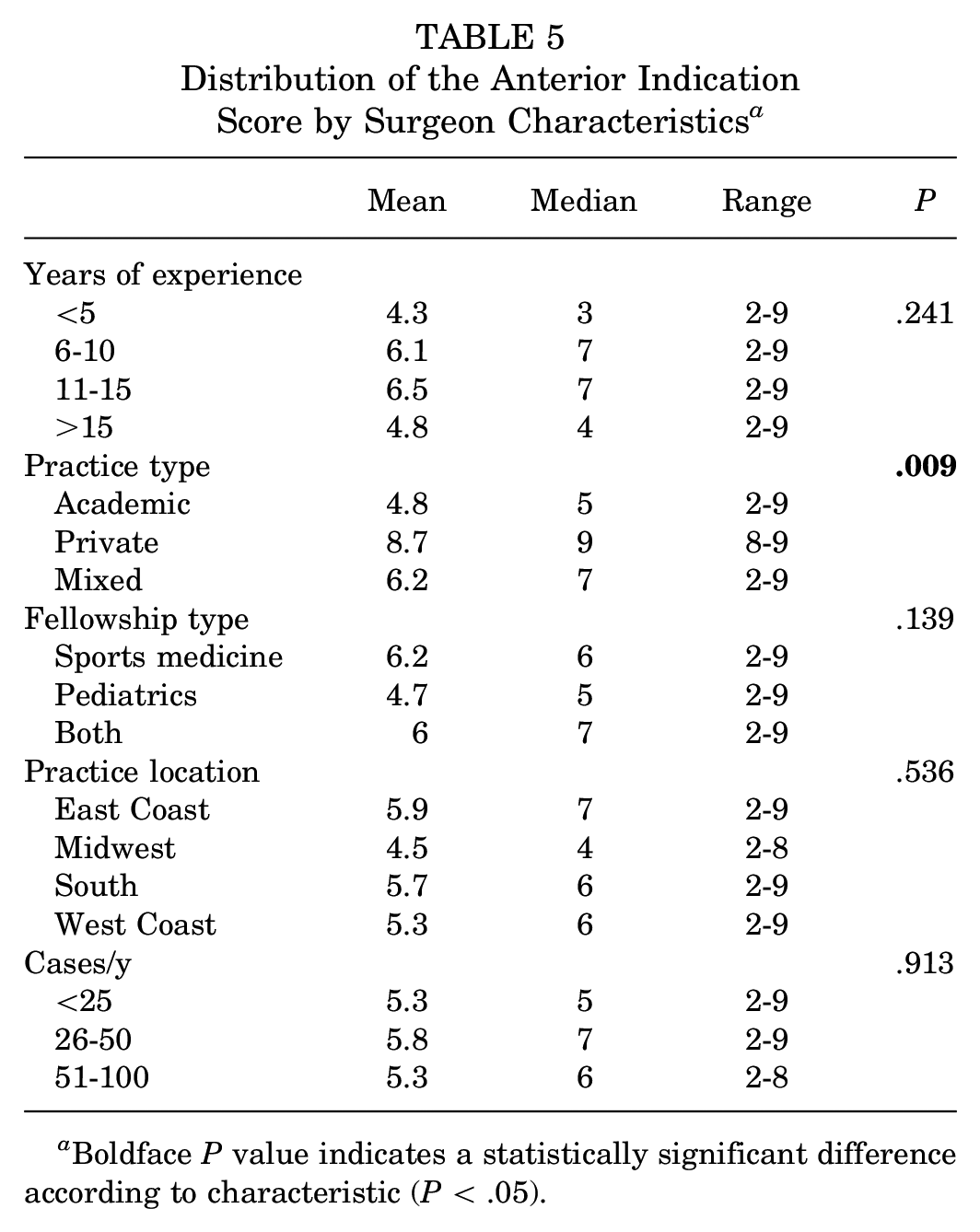
Boldface P value indicates a statistically significant difference according to characteristic (P < .05).
Unlike the Open Indication Score and Anterior Indication Score, the MDI Indication Score was not associated with YOE (P = .081) or practice setting (P = .743) (Table 6). In fact, the MDI Indication Score was not associated with any of the demographic factors we assessed.
Distribution of the MDI Indication Score by Surgeon Characteristics a

MDI, multidirectional instability.
Discussion
The management of anterior shoulder instability in adolescent patients continues to evolve. In our survey of providers who manage adolescent glenohumeral instability, there was a demonstrated consensus seen in the following scenarios:
Overall, 83% recommended nonoperative treatment for first-time anterior instability in patients with open physes and a noncontact injury.
Overall, 69% recommended arthroscopic stabilization for first-time anterior dislocation with closed/closing physes and a contact injury mechanism. This is a slight consensus, as it only just reaches the 66% threshold and would fail to be consensus if just 2 respondents changed their answers.
Overall, 97% recommended surgical treatment of patients with recurrent anterior dislocations regardless of physeal status or mechanism of injury.
Overall, 67% recommended nonoperative treatment of patients with MDI, no history of dislocation, open physes, and normal MRI/MRA scans. This is a slight consensus, as it only just reaches the 66% threshold and would fail to be consensus if just 1 respondent changed their answer.
Overall, 96% recommended surgical treatment of patients with MDI with multiple dislocations regardless of physeal status or mechanism of injury.
Despite consensus for these scenarios, disagreement remains for many common presentations of shoulder instability in patients regardless of provider. However, via the development of indication scores, there was an indication that years in practice (ie, YOE) influenced an interest in recommending open surgical procedures, and a private practice setting (including mixed-practice setting) influenced an interest in managing anterior shoulder instability with surgery.
The majority of respondents (80%) preferred an MRI scan in the evaluation of a first-time dislocation, with most preferring an arthrogram study. MRA can highlight more subtle intra-articular changes and has been shown to improve sensitivity for diagnosis of anterior and posterior labral tears compared with MRI alone.2,45,53 Respondents did not frequently order CT scans as the first-line advanced imaging, but CT scans may be useful to more accurately quantify acute or attritional bone loss and the need for adjunct procedures to a Bankart repair. 40
Consensus was achieved for preferred nonoperative management of first-time anterior shoulder instability in male patients aged <14 years and female patients aged <13 years. A systematic review and meta-analysis of risk factors for recurrent shoulder instability supports this consensus. 37 In evaluating 6 studies, the rate of recurrent shoulder instability was 73% in adolescent patients, with children aged 14 to 18 years being 2.4 times more likely to experience recurrent instability than those aged ≤13 years (93% vs 40%). 37 In evaluating 17 studies comparing nonoperative and operative management, patients <14 years in the primary nonoperative group were less likely to experience recurrence compared with those aged ≥14 years. 56 This may suggest a difference in outcomes between children and teenagers that could be further studied or a need to follow children longer to see if this risk changes when they become adolescents.
When consensus for surgical intervention was achieved, the majority of respondents preferred arthroscopic stabilization versus open repair. These findings are in line with the recent and predicted future national trends. In a large review of a national insurance database, arthroscopic stabilization (87%) was the most frequently utilized technique, far surpassing open Bankart repair (7%) in cases between 2007 and 2015. 41 In another large review, the number of open Bankart procedures decreased by 65% between 2009 and 2018, with future modeling predicting a further continued decline over the next 8 years. 1 This shift coincides with advancements in arthroscopic technique, instrumentation, and training over the past 20 years. 20 In the current study, only 3% of surgeons with ≤15 YOE recommended open repair compared with 27% of surgeons with >15 YOE. While prior studies had demonstrated superior results with open repair, more recent studies have shown no significant difference in the rate of recurrent instability or patient-reported outcomes between arthroscopic and open Bankart repair.13,17,19,21,26,49 While several small case series have shown good results with open stabilization in adolescent patients, arthroscopic stabilization additionally has been shown to have a shorter operative time, improved postoperative range of motion, and decreased cost.4,8,23,24,36 This represents another area of potential future study to determine if surgical approach (open vs arthroscopic with newer technologies) may change outcomes in this younger cohort.
MDI is a separate clinical presentation of pathological laxity characterized by instability in at least 2 directions. 6 MDI frequently has different physical examination and radiological findings compared with anterior instability. Features of MDI including high-grade laxity can be present in up to 20% of asymptomatic children and have a higher prevalence among swimmers and gymnasts.4,16,25 Advanced imaging is more likely to show a patulous inferior capsule or be normal.15,31 Nonoperative management with a minimum of 6 months of therapy and rehabilitation is often the first-line treatment for patients with MDI and can significantly improve functional outcomes.30,50-52 Consensus for nonoperative management was noted in the current study for patients with MDI with open physes and was inconclusive for those with closed physes.5,52 When nonoperative management fails, surgical management is often recommended. The present study shows consensus, with 96% of respondents recommending surgical intervention for patients with MDI with recurrent instability regardless of age or physeal status. While historically the treatment included open inferior capsular shift, similar to anterior instability, the trend has shifted to arthroscopic stabilization.6,43,48 In the current study, 83% recommended arthroscopic capsulolabral plication with suture anchors and 98% recommended complete rotator interval closure. Further study is needed to determine the role and benefit of surgical intervention in these patients.
Limitations
This study has several important limitations. First, consensus recommendations are based on expert opinion. The results presented here are intended to identify current management trends and determine where to best direct future research. Second, an anonymous survey method with a limited number of scenarios may oversimplify the problem and produce basic recommendations. Future research should be able to further detail factors that contribute to the lack of consensus. Third, while our survey response rate of 54 surgeons (41%) compares favorably to similar published response rates, there were low absolute numbers of respondents in some subcategories of practice settings.14,34 Fourth, only surgeons from the United States were included in the survey. Fifth, survey respondents were not asked to provide rationale for their answers or what additional factors might change their answers. Sixth, consensus was barely reached for 2 responses, which makes those consensus statements fragile. Those 2 responses included (1) operative management of first-time dislocators with anterior instability, closed/closing physes, and a contact injury mechanism; and (2) nonoperative management of MDI without history of dislocation, normal MRI/MRA scan, and open physes. The survey was sent to the entire surgeon membership of PRiSM, some of whom may not actually manage anterior shoulder instability; thus, the limited response rate needs to be understood with that information as well.
Conclusion
Adolescent patients with shoulder instability are a unique and challenging group of patients who require treatment informed by the type of instability, number of dislocations, skeletal maturity, and mechanism of injury. While consensus was able to be reached on recommended treatment for certain clinical scenarios, including age cutoffs for nonoperative management and surgical intervention for recurrent instability, the study also demonstrates disagreement among experts in the treatment of numerous common clinical scenarios. Further research and understanding are needed for developing optimal treatment for many subsets of these patients.
Supplemental Material
sj-pdf-1-ojs-10.1177_23259671241271735 – Supplemental material for Evaluation and Management of Glenohumeral Instability in Adolescent Patients: An Expert Consensus Statement
Supplemental material, sj-pdf-1-ojs-10.1177_23259671241271735 for Evaluation and Management of Glenohumeral Instability in Adolescent Patients: An Expert Consensus Statement by Paul M. Saluan, Matthew C. Beran, Charles M. Chan, Frank A. Cordasco, Jeremy Frank, Michael McClincy, Matthew D. Milewski, Lauren H. Redler, Pat Riley, Robert G. Tysklind, Drew E. Warnick, Jonathan Riboh and Nirav K. Pandya in Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted February 1, 2024; accepted February 13, 2024.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.T.F. has received education payments from Evolution Surgical. E.W.E. has received education payments from Elevate Surgical and nonconsulting fees from Arthrex. A.C.E. has received education payments from Arthrex and Smith+Nephew. S.N.P. has received education payments from CDC Medical and consulting fees from Pfizer. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.
Authors
PRiSM Shoulder Research Interest Group collaborators: Paul M. Saluan, MD (Cleveland Clinic Foundation, Cleveland, Ohio, USA); Matthew C. Beran, MD (Nationwide Children’s Hospital, Columbus, Ohio, USA); Charles M. Chan, MD (Stanford Medicine Children’s Health, Palo Alto, California, USA); Frank A. Cordasco, MD (Hospital for Special Surgery, New York, New York, USA); Jeremy Frank, MD (Joe DiMaggio Children’s Hospital, Miami, Florida, USA); Michael McClincy, MD (Children’s Hospital of Pittsburgh, Pittsburgh, Pennsylvania, USA); Matthew D. Milewski, MD (Boston Children’s Hospital, Boston, Massachusetts, USA); Lauren H. Redler, MD (Columbia University Medical Center, New York, New York, USA); Pat Riley, MD (Akron Children’s Hospital, Akron, Ohio, USA); Robert G. Tysklind, MD (Riley Children’s Health, Indianapolis, Indiana, USA); Drew E. Warnick, MD (Children’s Orthopaedics and Scoliosis Surgery Associates LLP, Tampa, Florida, USA); Jonathan Riboh, MD (Ortho Carolina, Charlotte, North Carolina, USA); and Nirav K. Pandya, MD (University of California, San Francisco, San Francisco, California, USA).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.