
Abstract
Background:
There are no studies on the nonoperative treatment of traumatic partial anterior cruciate ligament (ACL) graft rupture.
Purpose/Hypothesis:
The purpose of this study was to compare the clinical and radiological outcomes and failure rates between nonoperative treatment and revision ACL reconstruction for traumatic partial ACL graft rupture. We hypothesized that the outcomes and failure rates would be comparable and that nonoperative treatment of traumatic partial ACL graft rupture can produce satisfactory outcomes.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
We retrospectively evaluated 2114 patients treated for isolated ACL rupture between January 2000 and June 2020. Patients with traumatic partial graft rupture after ACL reconstruction with minimum 2-year follow-up data were included. Patients who met all the following conditions were candidates for nonoperative treatment: (1) Lachman or pivot-shift grade 0 or 1 at 6 months after ACL reconstruction, (2) ACL graft with low to intermediate signal intensity on 1-year postoperative magnetic resonance imaging (MRI), and (3) MRI after reinjury showing definite evidence of trauma, some fibers remaining in continuity of the ACL graft, and no anterior tibial subluxation in the sagittal plane. The patients were divided into 2 groups according to treatment method: nonoperative treatment (group A) and revision ACL reconstruction (group B). Clinical scores, laxity test results, radiological outcomes, and graft failures were compared between the groups.
Results:
In total, 47 patients had traumatic partial graft rupture (group A, n = 10; group B, n = 37). There were no significant differences between the 2 groups in terms of clinical scores, laxity tests, radiological outcomes, or graft failure.
Conclusion:
The clinical and radiological outcomes of nonoperative treatment of traumatic partial graft rupture after ACL reconstruction were comparable with those of revision ACL reconstruction. Nonoperative treatment of traumatic partial ACL graft rupture can produce satisfactory outcomes in selected patients.
Anterior cruciate ligament (ACL) reconstruction is a commonly performed operation and has shown favorable clinical outcomes. 4 –6,10 However, the failure rate after ACL reconstruction has been reported to be 0% to 14%. 15,27,29,30 Because ACL deficiency can cause cartilage injury, meniscal injury, and degenerative arthritis, surgical reconstruction is mainly performed in patients with ACL rupture. 17,24 Revision ACL reconstruction is still challenging for orthopaedic surgeons, and it is reported that the clinical outcomes are worse than those of primary ACL reconstruction. 34 Furthermore, bone tunnel defects, damage to cartilage and meniscus, and changes in anatomic landmarks due to prior surgery make surgery more difficult. 8,19,22,32,37
According to the patient cohort studied by the Multicenter ACL Revision Study (MARS) group, 32% of ACL reconstruction failures were caused by trauma, 24% by technical problems, 7% by biological problems, and 37% by a combination of these cases. 35 In cases of technical and biological failure, for example, because of an inappropriate tunnel, bone tunnel defect, or failure of the graft to incorporate, revision ACL reconstruction is usually performed. In a case of traumatic graft rupture, nonoperative treatment may be attempted if the ACL graft is partially ruptured.
To our knowledge, there are no studies on the nonoperative treatment of failed ACL reconstruction. Thus, the aim of this study was to compare the clinical and radiological outcomes and failure rates between nonoperative treatment and revision ACL reconstruction for traumatic partial ACL graft rupture. We hypothesized that the outcomes and failure rates would be comparable and that nonoperative treatment of traumatic partial ACL graft rupture can produce satisfactory outcomes.
Methods
Study Design
We retrospectively evaluated the records of 2114 patients treated for isolated ACL rupture between January 2000 and June 2020. All primary and revision ACL reconstructions had been performed at the same institution by the same experienced orthopaedic surgeon (K.H.Y.). Included in the study were patients with traumatic partial graft rupture after ACL reconstruction with a minimum follow-up of 2 years. Exclusion criteria were as follows: (1) failure with a nontraumatic mechanism, (2) ipsilateral fracture around the knee joint, and (3) insufficient medical records. The protocol for this study received institutional review board approval, and all included patients provided written informed consent.
Revision ACL reconstruction is offered for patients with totally displaced graft rupture or anterior tibial subluxation on magnetic resonance imaging (MRI) after reinjury. For eligible patients, a 6-month nonoperative treatment protocol was offered. To implement 6 months of nonoperative treatment in young and active patients, we needed a more specific definition of traumatic partial graft rupture and set the following narrow indications: (1) Lachman or pivot-shift grade 0 or 1 at 6 months after ACL reconstruction, (2) ACL graft with low to intermediate signal intensity at 1 year postoperatively on MRI, and (3) MRI after reinjury showing definite evidence of trauma (bone bruise of the lateral femoral condyle and lateral tibial condyle, hemarthrosis, etc), some fibers remaining in continuity of the ACL graft, and no anterior tibial subluxation in the sagittal plane (Figure 1).
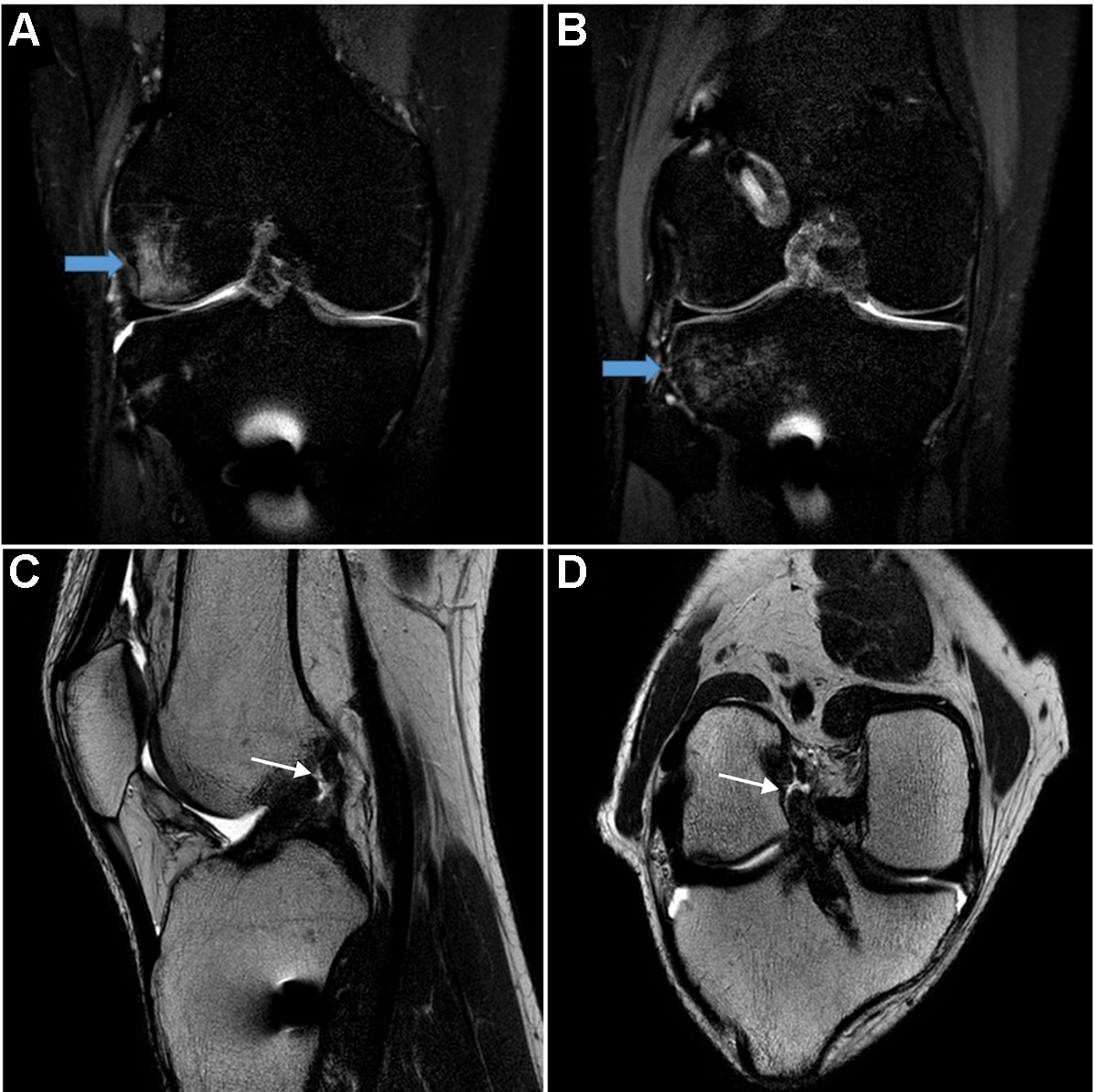
Right knee magnetic resonance imaging (MRI) of a male patient who underwent anterior cruciate ligament (ACL) reconstruction when he was 20 years old. The reinjury occurred 30 months after primary ACL reconstruction. MRI scans taken immediately after reinjury show a bone bruise in the (A) lateral femoral condyle and (B) lateral tibial condyle (blue arrows). ACL graft rupture on (C) sagittal view and (D) oblique coronal view MRI scans (thin white arrows). Note the ruptured ACL graft maintaining normal graft angle and no anterior subluxation of tibia. For additional images, see Supplemental Figures S1 and S2, available separately.
Failure of nonoperative treatment was defined as a grade 3 Lachman or pivot shift after 6 months of treatment. It was explained to the eligible patients that if the nonoperative treatment failed, a delayed revision ACL reconstruction could still be performed. All the patients accepted our explanation and chose nonoperative treatment. The patients undergoing nonoperative treatment for their partial graft rupture (group A) were compared with a cohort of patients who underwent revision ACL reconstruction for a totally displaced graft rupture (group B).
Nonoperative Treatment
The nonoperative treatment protocol (Table 1) was the same as that for the postoperative rehabilitation of revision ACL reconstruction. Immediate weightbearing was permitted. Range of motion (ROM) exercises were not allowed for 3 weeks with a full-extension brace. Until the sixth week, the patients were not allowed to flex their knee up to 90°. ROM exercises were allowed gradually.
Protocol of Nonoperative Treatment and Rehabilitation After Revision ACL Reconstruction a

a ACL, anterior cruciate ligament.
Surgical Technique
A single surgeon (K.H.Y.) performed all the ACL reconstructions and revision ACL reconstructions. During revision ACL reconstruction, allograft bone chips and blocks were packed into the femoral and tibial tunnels for bone tunnel widening if the previous tunnel was widened by >9 mm. During the revision ACL reconstruction, an autograft was used if possible. A tibial tunnel was created on the anatomic ACL footprint. Next, the femoral tunnel was placed in the anatomic ACL footprint using the transtibial or transportal technique 38 according to the bony landmarks and arthroscopic findings of the ACL footprint. The graft tendon was fixed on the tibial side with a soft tissue washer and screw, with a biodegradable interference screw fitted to the diameter of the tunnel, and on the femoral side with an Endobutton CL (Smith & Nephew). The patients with primary and revision ACL reconstruction followed a similar rehabilitation protocol.
Postoperative Rehabilitation
All the patients followed a similar rehabilitation protocol (Table 1), except for those who required meniscal repair. 36,37 Similar steps were taken to those for nonoperative treatment, beginning with limiting ROM exercises in the third week. In patients who required meniscal repair, rehabilitation was modified to exclude weightbearing activities and 90° of knee flexion for the first 6 weeks. Full flexion was allowed between 3 and 6 months postoperatively.
Clinical and Radiological Evaluation
Clinical scores and stability function tests were evaluated at each follow-up outpatient clinic visit. Clinical scores were based on the International Knee Documentation Committee (IKDC), Lysholm, and Tegner activity scores. The stability function tests included the anterior drawer test, Lachman test, pivot-shift test, and side-to-side difference in anterior tibial translation on Telos stress radiography at 30° of knee flexion. The Lachman test results were graded as 0 (1-2 mm), 1 (3-5 mm), 2 (6-10 mm), and 3 (>10 mm). The pivot-shift test results were graded as 0 (equal), 1 (glide), 2 (clunk), and 3 (locking). 13 Side-to-side difference in anterior tibial translation was measured using Telos stress radiographs. 26 Four patients in group A delayed the side-to-side difference testing until 6 months after reinjury, as the examination itself can progress from partial to complete rupture and impair continuity.
The condition of the ACL graft was assessed using MRI (3.0-T Achieva; Philips Medical Systems) with a knee coil 6 months after reinjury for group A and 1 year postoperatively for group B. Images were taken with the patient positioned in 5° of knee flexion (Figure 2).

Magnetic resonance imaging (MRI) scan of the right knee taken 6 months after nonoperative treatment (same patient as in Figure 1). The MRI scan shows the healed anterior cruciate ligament graft in the (A) sagittal view and (B) oblique coronal view.
Anterior tibial subluxation was determined by using the technique described by Tanaka et al. 31 On the sagittal proton density images, a best-fit circle over the subchondral line of the posterior condyle was drawn. A line perpendicular to the lateral tibial plateau was drawn along the posterior margin of this circle. Then a second line perpendicular to the tibial plateau was drawn through the posterior aspect of the lateral tibial plateau. The direct distance between these 2 lines was then measured to determine the amount of anterior tibial translation (Figure 3). According to Tanaka et al, the lateral tibial position was anteriorly translated a mean of 3.9 mm in the setting of failed ACL reconstructions. In our study, ≤3 mm of anterior tibial translation was defined as no anterior tibial subluxation.

Measurement technique of anterior tibial translation. First, a best-fit circle was drawn over the subchondral line of the posterior condyle, and then line a was drawn tangent to the lateral tibial plateau. Next, 2 parallel lines, b and c, perpendicular to line a, were drawn through the posterior margin of the circle and lateral tibial plateau, respectively. The distance between lines b and c determined the anterior tibial translation.
Graft signal intensity was qualitatively assessed according to the protocol of Kanamiya et al. 16 Based on T2-weighted oblique-coronal images, which express the ACL fibers in parallel, the low signal intensity was similar to that of the patellar tendon (Figure 4A), the intermediate signal intensity was similar to that of the gastrocnemius muscle (Figure 4B), and the high signal intensity was greater than the intermediate signal intensity (Figure 4C).
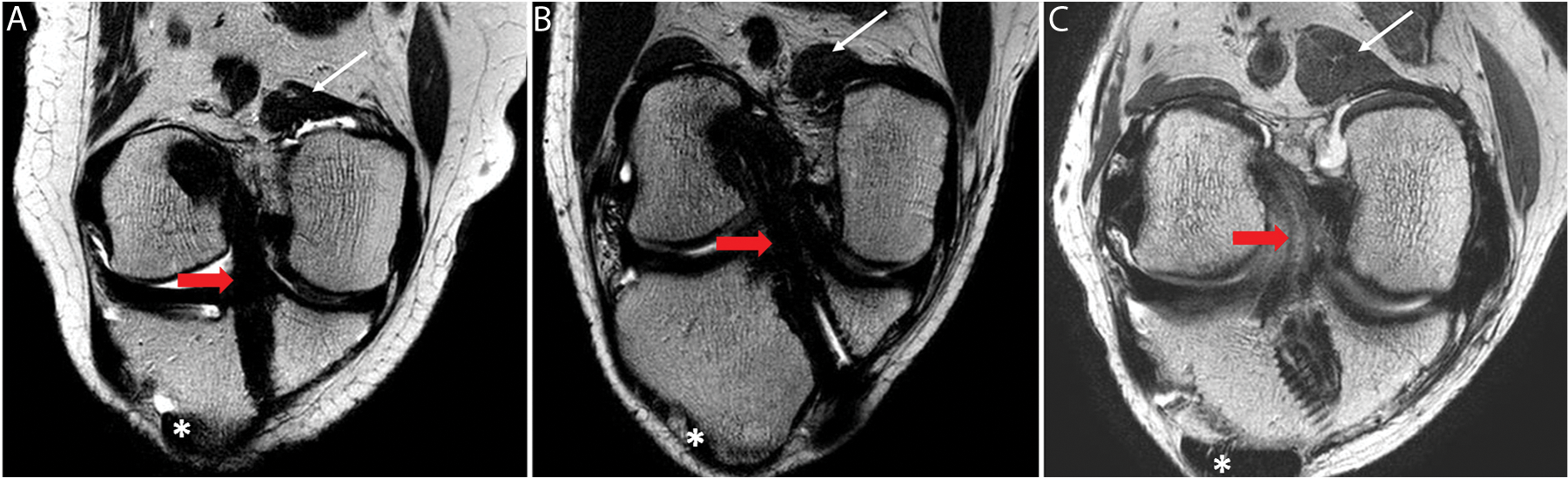
Oblique coronal magnetic resonance imaging (MRI) after anterior cruciate ligament (ACL) reconstruction. Asterisks indicate the patellar tendon for low-signal MRI intensity, thin white arrows indicate the gastrocnemius muscle for intermediate-signal MRI intensity, and red arrows indicate the ACL graft.
Treatment Failure
Treatment failure was defined as the need for additional surgery or grade 3 instability on the pivot-shift test at 6 months after reinjury or postoperatively, which is consistent with graft failure. 37
Statistical Analysis
All statistical analyses were performed using IBM SPSS Statistics for Windows Version 22 (IBM Corp). An independent t test or Mann-Whitney U test was used to compare parametric or nonparametric variables between the 2 groups. Preoperative and postoperative parametric or nonparametric variables were compared using the paired t test or Wilcoxon signed-rank test. The chi-square test was used to compare categorical data. If >20% of the expected frequencies were >0.5, the Fisher exact test was applied. Statistical significance was set at P < .05.
Results
Patient Characteristics
Among the 2114 patients who underwent isolated ACL reconstruction between January 2000 and June 2020, 85 (4.0%) patients experienced failure. Of these patients, 47 were included in the study; 10 patients underwent nonoperative treatment (group A), and 37 patients underwent revision ACL reconstruction (group B) (Figure 5). One of the patients who underwent nonoperative treatment had a delayed revision ACL reconstruction. The data before revision ACL reconstruction of this patient were included in group A.

Flowchart of patient enrollment. ACL, anterior cruciate ligament.
Among the 85 patients for whom treatment failed, 31 used autografts at the time of primary ACL reconstruction and 54 used allografts (P = .002). Of the 47 patients who experienced a traumatic graft rupture, 11 used autografts at the time of primary ACL reconstruction and 36 used allografts (P = .001) (Table 2).
Overall ACL Graft Failures and Traumatic Partial Rupture by Graft Type a
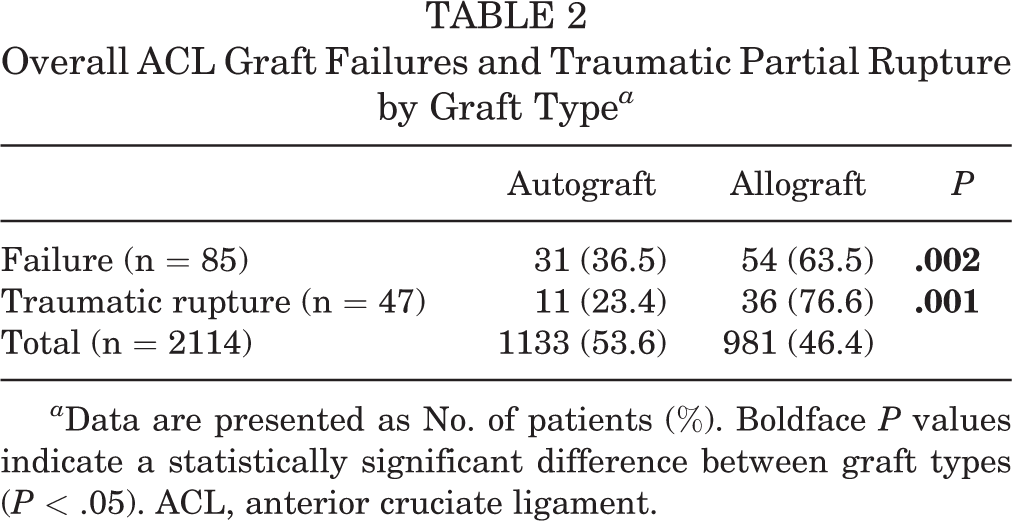
a Data are presented as No. of patients (%). Boldface P values indicate a statistically significant difference between graft types (P < .05). ACL, anterior cruciate ligament.
The mean time from reinjury to final follow-up was 33.2 ± 15.3 months in group A, and the mean time from revision reconstruction to final follow up was 49.2 ± 31.5 months in group B. The patient characteristics for both groups are summarized in Table 3. There were no significant differences between the groups.
Patient Characteristics (N = 47) a

a Data are presented as No. of patients or mean ± SD. ACL, anterior cruciate ligament; ACLR, anterior cruciate ligament reconstruction; BMI, body mass index.
b Follow-up duration is from reinjury for group A and from revision anterior cruciate ligament reconstruction for group B.
Two patients in group A had a longitudinal tear of the medial meniscus. The patients underwent meniscal repair after 6 months of nonoperative treatment. The arthroscopic appearance of the ACL graft at the time of meniscal repair is shown in Supplemental Figure S3, available separately. In total, 22 patients in group B had a meniscal injury. The patients underwent revision ACL reconstruction with meniscal excision for horizontal and flap tears and meniscal repair for longitudinal and root tears (Table 4).
Combined Meniscal Injuries a

a Data are presented as No. of patients (%). ACLR, anterior cruciate ligament reconstruction.
Clinical and Radiological Evaluation
At the final follow-up, clinical scores including the IKDC, Lysholm, and Tegner activity scores were improved after treatment but did not differ significantly between the groups (Table 5). The IKDC subjective score was 76.6 ± 9.1 in group A and 69.6 ± 17.2 in group B at the final follow-up (P = .295). There was no significant difference in Lysholm scores (79.8 ± 19.1 vs 76.6 ± 18.2; P = .196) or Tegner activity scores (5.4 ± 1.6 vs 5.9 ± 2.5; P = .851).
An all-stability function test also showed postoperative improvement in both groups. However, the anterior drawer test and side-to-side difference test in group A were not statistically different. There was no significant intergroup difference between the 2 groups in stability function tests or MRI evaluations after the treatment.
Clinical and Radiological Outcomes After Reinjury and at Latest Follow-up a

a Data are presented as mean ± SD or No. of patients. ACLR, anterior cruciate ligament reconstruction; IKDC, International Knee Documentation Committee; MRI, magnetic resonance imaging; SSD, side-to-side difference.
b The values are for 6 patients.
Treatment Failure
In group A, 1 patient with an allograft for primary ACL reconstruction underwent delayed revision ACL reconstruction at 1 year after reinjury because the patient was unable to participate in vigorous activities. In group B, 3 patients underwent re-revision ACL reconstruction. Of these, 2 patients experienced failure because of reinjury during exercise, and 1 patient experienced failure because of repetitive microtrauma. All 3 patients had an autograft for their primary ACL reconstruction. There were no patients with grade 3 pivot shift in either of the groups (Table 6).
Characteristics of Failure a
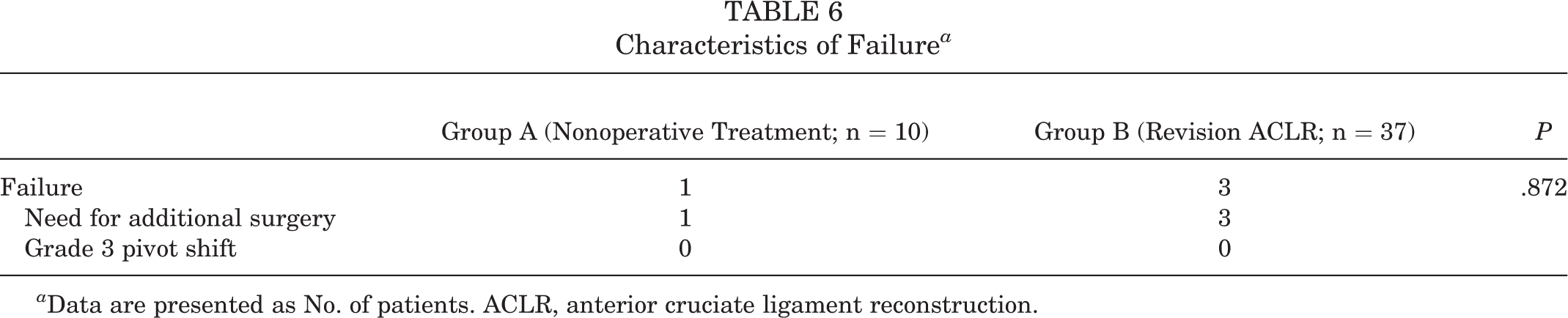
a Data are presented as No. of patients. ACLR, anterior cruciate ligament reconstruction.
Discussion
The most important finding of this study was that patients with traumatic partial graft rupture after ACL reconstruction can be treated nonoperatively. After treatment, the clinical scores (IKDC subjective, Lysholm, and Tegner activity scores) improved in both groups and there was no significant difference in posttreatment outcome scores, laxity examination, or MRI appearance between groups. However, there were considerable differences between groups A and B. Group B had totally displaced graft rupture or anterior subluxation on the reinjury MRI. Group B also included patients with grade 2 or 3 laxity on stability testing, and they had more meniscal tears than group A. Therefore, these results should be interpreted with caution.
In our study, the clinical scores of both groups A and B were modest. In a recent meta-analysis, the mean IKDC subjective score was 76.99 (95% CI, 76.64-77.34) and the mean Lysholm score was 86.18 (95% CI, 79.08-93.28) in revision ACL reconstructions. 23 Previous studies have shown that revision ACL reconstruction has inferior clinical outcomes, including clinical scores and failure rates, to primary ACL reconstruction. 12,34 This is probably because of the bone tunnel defect, combined cartilage and meniscal injuries, and changes in anatomic landmark. 8,22,32,37
Two patients in group A and 22 patients in group B had a meniscal injury. In group A, patients underwent meniscal repair after 6 months of nonoperative treatment. According to the 2019 European Society for Sports Traumatology, Knee Surgery and Arthroscopy meniscal consensus, acutely repaired meniscal tears achieve better outcomes compared with chronically repaired tears, but repaired chronic meniscal tears also achieve favorable outcomes. 18 Coincidentally, there was no bucket-handle tear in our cohort. However, in the case of a traumatic ACL graft rupture with a bucket-handle tear of the meniscus, revision ACL reconstruction should be considered given the limited ROM.
Failure occurred in 1 (10%) patient in group A after nonoperative treatment. To the best of our knowledge, no previous studies have performed nonoperative treatment in patients with traumatic graft rupture. Barrack et al 3 evaluated the clinical outcomes of nonoperative treatment of ACL rupture and reported that only 37% had good or excellent knee function. Bak et al 2 evaluated the natural history of partial ACL tears 5 years after the initial injury. They reported that only 62% had good or excellent knee function, and a significant decline in activity was observed. These studies reported relatively poor results because the indications for nonoperative treatment were not established. Fujimoto et al 11 reported that of 31 patients with primary ACL rupture who underwent nonoperative treatment, 23 (74.2%) had good outcomes and 8 (25.8%) eventually underwent ACL reconstruction. In this study, indications for nonoperative treatment were low athletic demand and an injured ACL showing a continuity of fibers on an MRI scan. Ahn et al 1 reported that 47 of 48 patients with primary ACL rupture who underwent nonoperative treatment had good outcomes and that 1 patient underwent ACL reconstruction. In this study,1 patients diagnosed with an acute ACL injury by MRI, with Lachman test grade 1, and with good patient compliance were treated nonoperatively. In our study of a group of patients who underwent ACL reconstruction once, the failure rate was 10% as a result of nonoperative treatment with strict indications. We believe that favorable results can be obtained if one follows the strict indications for nonoperative treatment used in the current study.
In a recent study of the Knee Anterior Cruciate Ligament Nonsurgical vs Surgical Treatment trial, 16 of 54 (29.6%) patients who received nonoperative treatment showed ACL healing on MRI after complete rupture of their ACL. 9 Also, the patients with evidence of ACL healing on MRI at 2 years reported better clinical scores compared with the nonhealed patients and ACL reconstruction groups. Some authors speculate that younger age, remaining fibers in continuity not visualized on MRI, and overlying synovial lining holding the ends in proximity may be associated with greater healing potential. 7 In our study, the patient age of group A was 21.7 ± 2.7 years, and some fibers remained in continuity of the ACL graft. These factors may have influenced the healing of the ACL graft.
However, the definition of traumatic ACL graft rupture has not yet been established. In the MARS group, the surgeon involved in the study checked the mechanism of failure, but there was no clear definition of traumatic graft rupture. 35 In one study, traumatic graft rupture was determined through a review of medical records. 28 In another study, a questionnaire was used to determine whether there was traumatic incidence. 14 A single adequate traumatic incidence was considered a traumatic rupture, regardless of other technical and biological factors. For traumatic graft rupture to have clinical relevance in determining nonoperative treatment, graft rupture should occur only as a traumatic event without other technical or biological factors. Therefore, this study is limited to patients with these conditions.
In a recent MRI study at 12 and 24 months, ACL graft signals approximated the signals of a native intact ACL. 21 In addition, the more hypointense the signal intensity of the ACL graft at 2 years, the more likely the patient will be able to return to preinjury sports levels. Meanwhile, the reinjury rate after ACL reconstruction has been reported to be 6% to 12% in short- and mid-term follow-up studies 27,33 and 27% to 34% in the long-term follow-up study. 20,25 Therefore, we believe that MRI can be performed 1 or 2 years after surgery to provide evidence of graft maturation. This could serve as a basis for attempting nonoperative treatment in cases of traumatic graft rupture, similar to that in these patients.
Strengths and Limitations
The strength of our study is that it was conducted only on surgeries performed by an experienced surgeon at a single institution. Additionally, nonoperative treatment of traumatic graft rupture after ACL reconstruction has not been previously discussed. Furthermore, clear indications for nonoperative treatment for traumatic partial graft rupture are suggested.
There are several limitations to this study. First, because of its retrospective and nonrandomized design, selection bias may have influenced the results. Furthermore, group B had more meniscal tears than group A, and there were more patients with grade 2 or 3 on stability tests in group B before treatment. Second, the sample size was smaller in group A than in group B. Also, 4 of 10 patients in group A did not undergo a stability test, which could have potentially biased the results. However, this is inevitable because only a small number of patients meet these strict criteria, and our study is the first to compare nonoperative and surgical treatments for traumatic ACL graft rupture. Future studies need more data, such as data from multicenter studies. Third, associated injuries, such as chondral injury, were not considered in this study. Further discussion is needed in cases of traumatic ACL graft rupture with associated injury. Fourth, although not statistically significant (P = .067), group B was followed up for 16 months longer, on average, than group A; thus, further study with mid- and long-term follow-up is required. Fifth, our results lack the types of sports played and return-to-sports data. Finally, performing MRI 1 to 2 years after surgery can be costly for patients. However, if MRI shows that favorable results can be obtained without surgery through nonoperative treatment, we think it is worthwhile to perform MRI even at a cost.
Conclusion
The short-term clinical and radiological outcomes of nonoperative treatment of traumatic partial graft rupture after ACL reconstruction are comparable with those of revision ACL reconstruction. However, associated meniscal injury should be taken into account to determine treatment. Nonoperative treatment of traumatic partial graft rupture can produce satisfactory outcomes in selected patients.
Supplemental material for this article is available at https://journals.sagepub.com/doi/full/10.1177/23259671231182124#supplementary-materials
Supplemental material for this article is available at https://journals.sagepub.com/doi/full/10.1177/23259671231182124#supplementary-materials.
Supplemental Material
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671231182124 - Nonoperative Treatment for Traumatic Partial Graft Rupture After Anterior Cruciate Ligament Reconstruction: A 2-Year Follow-up Study
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671231182124 for Nonoperative Treatment for Traumatic Partial Graft Rupture After Anterior Cruciate Ligament Reconstruction: A 2-Year Follow-up Study by Kyung Ho Yoon, Cheol Hee Park, Hee Sung Lee and Sung Hyun Hwang in Orthopaedic Journal of Sports Medicine
Footnotes
Acknowledgment
Final revision submitted February 12, 2023; accepted March 2, 2023.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Kyung Hee University Hospital (reference No. KHUH 2022-06-070)
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.