
Abstract
Background:
The literature on revision anterior cruciate ligament (ACL) reconstruction (ACLR) outcomes is generally sparse, but previous studies have demonstrated that autograft use results in improved sports function and patient-reported outcome measures compared with allograft. However, knowledge is still lacking regarding the impact of graft type on rates of re-revision.
Purpose:
To investigate the clinical outcomes and failure rates of revision ACLRs performed with either allograft or autograft.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
A search of the Danish Knee Ligament Reconstruction Registry identified 1619 revision ACLRs: 1315 were autograft procedures and 221 were allograft procedures (type of graft was not identified for 83 procedures). Clinical outcomes after 1 year were reported via the Knee injury and Osteoarthritis Outcome Score (KOOS), the Tegner activity score, and an objective knee stability measurement that determined side-to-side differences in instrumented sagittal knee laxity. Failure was determined as re-revision. Outcomes for revision were provided for the full life of the registry, up to 10 years.
Results:
The re-revision rate was significantly higher for allograft compared with autograft (12.7% vs 5.4%; P < .001), leading to a hazard ratio for re-revision of 2.2 (95% CI, 1.4-3.4) for allografts compared with autografts when corrected for age. At 1-year follow-up, objective knee stability was significantly different (2.1 ± 2.1 mm for allograft vs 1.7 ± 1.8 mm for autograft; P = .01), and the KOOS subscale scores for symptoms, pain, activities of daily living, sports, and quality of life were 67, 76, 84, 49, and 46 for allograft and 67, 78, 84, 51, and 48 for autograft, respectively, with no difference between groups.
Conclusion:
In this observational population-based study, the ALCR re-revision rate was 2.2 times greater for allograft compared with autograft procedures. Allograft was associated with greater knee laxity at 1-year follow-up. However, subjective clinical outcomes and knee function were not inferior for allograft patients. These results indicate that autograft is a better graft choice for revision ALCR.
Patients who undergo revision anterior cruciate ligament (ACL) reconstruction (ACLR) have shown significantly lower Knee injury and Osteoarthritis Outcome Score (KOOS) results compared with patients who have primary ACLR. 8 The failure rate of revision ACLR is 3 to 4 times higher than for primary ACLR when failure is defined as re-revision, more than 5 mm of laxity, or high-grade pivot shift. 17 The 2-year revision rate is 1.7% for primary ACLR and 4.7% for revision ACLR. 8 Optimized surgical technique is therefore important to minimize failure rates after revision ACLR.
The most common graft choice for revision ACLR is an autograft from a different location than the graft that was used at primary surgery. However, allograft is frequently used for revision ACLR for numerous reasons, such as lack of suitable remaining autograft options, avoidance of additional donor-site morbidity, need to fill bone tunnels with tunnel widening, or need for large-diameter graft tissue. 7,11,17 In the United States, allografts have mainly been used for primary ACLR because of their high availability. The Multicenter Orthopedic Outcome Network (MOON) group has investigated a large US cohort of primary ACLRs and found an increased risk of reinjury with use of allograft. This risk was correlated to age, with younger patients having higher risk for failure. 4 A US study from the Kaiser Permanente Institute demonstrated allografts to have 3 times higher risk of revision compared with bone–patellar tendon–bone autograft. 12
The literature is generally sparse regarding outcomes of revision ACLR, but results from the US Multicenter ACL Revision Study (MARS) have demonstrated that autograft use results in improved sports function and patient-reported outcome measures compared with allograft. 9 Furthermore, the rerupture rate at 2-year follow-up was 2.2% for autografts compared with 4.4% for allografts. 10 A Danish national cohort study found a 5-year re-revision risk of 5.4% after revision ACLR. 8 More data are needed regarding the influence of graft choice on failure and subjective clinical outcomes in a large cohort, which potentially reflects the overall clinical state of revision ACLR. National clinical registries offer high patient numbers that allow investigation of rare parameters such as failure after ACLR.
The purpose of the present study was to investigate the clinical outcomes and failure rates of revision ACLRs performed with either allograft or autograft. We hypothesized that revision ACLRs performed with allografts would entail more knee laxity and higher re-revision rates than revision ACLRs performed with autografts.
Methods
This study is based on information retrieved from the Danish ACLR Registry (DKRR), which is a nationwide, web-based clinical database that was started on July 1, 2005. It contains data on primary and revision ACL procedures. Both public and private hospitals provide data, and it is obligatory for all Danish hospitals to register. Completeness of patient inclusion in the registry is higher than 90%; this has been calculated by identifying missing procedures through use of the Danish National Patient Registry, which contains all surgical procedures performed in the country, enabling investigation of outcomes with different graft types for revision surgery. 8 Preoperative and 1-year follow-up data in the registry are recorded by the operating surgeon. Furthermore, the patients independently report on subjective knee function using self-assessment scores: the KOOS and the Tegner activity score. These data are web-recorded by the patient before surgery and 1 year after surgery.
The present study included all first-time revision ACLRs performed with either an allograft or autograft in the period from July 1, 2005, to December 31, 2015. The exclusion criterion was multiligament reconstruction. In total, 1619 revision ACLRs were identified in the DKRR: 1315 (81%) autograft procedures, 221 (13.6%) allograft procedures, and 83 (5%) procedures with unregistered graft. The patients with unknown graft type were excluded from the study. The completeness for 1-year objective knee laxity data was 52%, and the completeness for patient-registered 1-year follow-up subjective scores was 27%. The patients were separated by graft type; the data regarding sex, age, and meniscal and cartilage injury for each cohort are described in Table 1.
Comparison of the 2 Graft Cohorts a
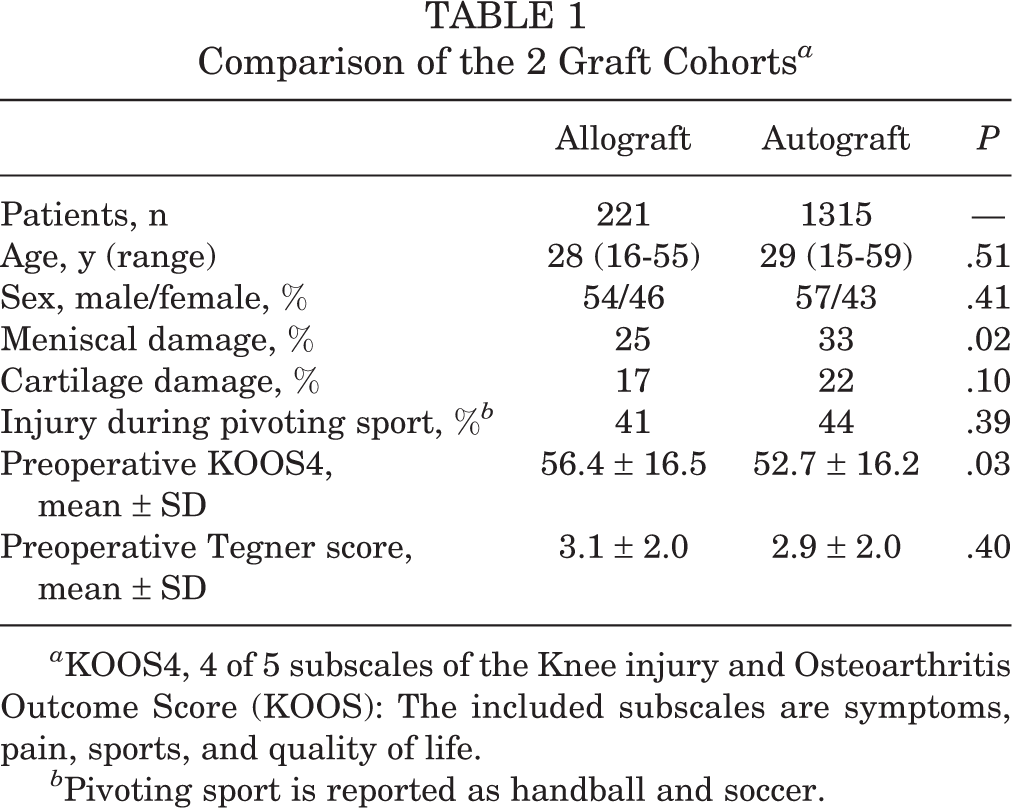
a KOOS4, 4 of 5 subscales of the Knee injury and Osteoarthritis Outcome Score (KOOS): The included subscales are symptoms, pain, sports, and quality of life.
b Pivoting sport is reported as handball and soccer.
Outcome Measures
The KOOS 13 and the Tegner activity score 16 were used to measure subjective outcomes and knee function at 1 year of follow-up. To calculate a single measure for the impact of ACLR based on KOOS data, a new parameter has recently been defined for ACLRs. This measure is designated as KOOS4 and is defined as the change in the 4 most responsive KOOS subscale scores from preoperative to postoperative assessments. 2 The included subscales are symptoms, pain, sports, and quality of life. KOOS4 is a validated parameter for evaluating knee function. 2 Objective knee stability, defined as side-to-side difference in instrumented sagittal knee laxity, was determined at 1 year by Rolimeter or KT-1000 arthrometer measurement; 70% of clinics used Rolimeter and 30% used KT-1000 arthrometer. Failure was defined as a new revision ACLR procedure. Follow-up for revision was from 1 to 10 years depending on inclusion time.
The Danish National Board of Health and the Danish Data Protection agency approved this study.
Statistical Analysis
We hypothesized that the re-revision rate would be 5% for autograft and 10% for allograft. Power calculation with a power level of 0.80 demonstrated that 220 patients were needed per investigational group. With 221 patients in the smallest subgroup, we had sufficient patients for comparison of revision rates. Statistical analysis was performed using Stata software version 14 (Stata Corp). The KOOS and Tegner scores were calculated according to published standards, 13,14 and the KOOS4 was also calculated. We calculated proportions to describe patient characteristics for each study population. Side-to-side difference in knee laxity, measured in millimeters, was calculated as a mean value. Changes in KOOS and Tegner score data between preoperative assessment and 1-year follow-up were investigated by Student t test. Student t test was also used to compare 1-year KOOS and Tegner outcomes as well as knee laxity between study groups.
The chi-square test was used to compare rates of allograft and autograft reconstruction re-revision. Increased risk for revision was also calculated as a hazard ratio (HR), with autograft as the comparison group. A log-linear Cox regression analysis was used to adjust HR data for the following potential confounding factors: age, sex, cause of injury (pivoting vs nonpivoting sports), and meniscal injury (yes/no). A Kaplan-Meier curve was calculated for full follow-up survival. The assumption of proportional hazards was tested using log-log plots and Cox-Snell residuals and was found acceptable; P < .05 was considered statistically significant.
Results
Demographics
The autograft cohort consisted of 1315 patients, of whom 71 patients had re-revision ACLR. The allograft cohort had 221 patients, of whom 28 patients had re-revision ACLR. The re-revision rate was significantly higher for allograft (12.7%) compared with autograft (5.4%) (P < .001). Revision reconstruction survivorship is presented in a Kaplan-Meier survivorship curve (Figure 1), which shows that after only 1 year, there was a higher survivorship percentage for autografts. The HR for re-revision was 2.2 (95% CI, 1.4-3.4) for allografts compared with autografts when corrected for age.

Kaplan-Meier survivorship curves of the graft types versus time after revision anterior cruciate ligament reconstruction.
Knee Stability
Objective knee stability was 5.6 ± 2.5 mm for allograft and 5.7 ± 2.3 mm for autograft preoperatively, with no significant difference. At 1 year postoperatively, objective knee stability was 2.1 ± 2.1 mm for allograft and 1.7 ± 1.8 mm for autograft, with a significant difference (P = .01).
The proportion of patients who had 3 mm or more side-to-side difference in laxity was 30% for allograft revision and 22% for autograft, which was not statistically significant.
Patient-Reported Outcome Measures
Subjective outcome based on KOOS and Tegner scores demonstrated significant improvements from preoperative to 1-year postoperative assessments for both autografts and allografts (Table 2). The increase was found for 4 of the 5 KOOS subscales (KOOS symptoms being the subscale that did not show improvement). The most responsive KOOS subscales were sports and quality of life, which improved about 15 points for both. However, no differences in KOOS results between the 2 graft types were noted at 1-year follow-up. Tegner activity scores improved significantly from preoperative to 1-year postoperative for both autografts and allografts, with no significant difference at 1-year follow-up (Table 2).
Pre- and Postoperative Outcome Scores for the Different Graft Types a

a Values are expressed as mean ± SD. There were no significant differences between the autograft and allograft groups at 1-year follow-up. KOOS, Knee injury and Osteoarthritis Outcome Score; KOOS4, 4 of 5 KOOS subscales: symptoms, pain, sports, and quality of life.
Discussion
The most important finding in the present study was that allograft use resulted in a 2.2 times higher risk of re-revision compared with autograft when corrected for age. Allograft also resulted in a significant 0.4-mm higher knee laxity. This small difference is probably not of clinical relevance. The proportion of patients with high laxity (≥3 mm) was not significantly different between allograft and autograft groups. The main disadvantage of allograft use for ACL revision, therefore, is not poor stability compared with autograft but rather a higher risk of graft failure leading to re-revision surgery. For patient-reported outcome measures and knee function, both graft types resulted in significant improvements from preoperative to 1-year postoperative assessments, without any difference between graft types.
Graft failure leading to revision ACLR is an important issue, but the literature contains few studies that investigate the influence of graft choice on clinical outcome for revision ACLR. A study from the MARS group based on 1205 patients showed that autograft resulted in better patient subjective scores, lower rerupture rates, and improved sport function compared with allograft. 10 When investigating 1099 revision ACLRs, Lind et al 8 showed that the relative risk of re-revision was 2.02 (95% CI, 1.5-2.4) with allograft compared with autograft. A smaller cohort study of 44 patients demonstrated no major differences between allograft and autograft but showed quicker return to sports for autograft. 6
The present study supports these findings, with allografts being associated with higher re-revision rates and greater knee laxity. However, unlike the MARS study, we did not find differences in patients’ subjective scores and knee function. In the present study cohort, allografts were used for revision ACLR in 14% of procedures. This proportion is lower than the referenced US MARS cohort, where allografts were used in 54% of procedures. 10 The lower use of allograft in the present study cohort reflects graft choices found in a review study 17 ; in that review, which described outcomes after revision ACLR in 1004 patients from 21 studies, allografts were used in 11% of procedures. The high incidence of allograft use in the United States is most likely attributable to good availability of allograft tissue for ligament reconstruction, which is also reflected in graft choice for primary ACLRs. 3 Another study from the MARS group investigated the reasons for graft choice for revision ACLR and found that surgeon preference was the most important factor and graft choice at primary surgery was the second most important factor. 5
Allograft is typically chosen for revision ACLR when autografts are not available due to use in previous reconstructions, or when previously made drill holes preclude anchoring of an autograft. Therefore, it is fair to assume that the ACLRs with allografts were made under more difficult surgical conditions. The poorer outcome found for allografts could therefore be influenced by the more challenging surgical conditions and poor bone stock due to previous surgery. In other words, use of allograft may entail a selection bias toward poorer outcome. The higher revision rate could also be attributed to biological properties of allograft tissue. Biological studies have shown that autograft tissue incorporates more quickly and completely than allograft tissue. 15 These different healing properties could place allograft tissue at higher risk for graft failure, as seen in the higher revision rate when allograft was used for revision ACLR. Allograft processing has been shown to affect graft biomechanical properties and thereby the potential safety of allografts for ligament reconstruction. 1 However, all allografts used in Denmark are fresh-frozen, unprocessed grafts, so graft processing is not a factor in the national Danish cohort.
The higher re-revision rate for allograft is the most important finding of this study and points toward autograft as a safer graft type for revision ACLR. The finding of less laxity for autograft compared with allograft also supports autograft as the best graft choice for revision ACLR.
A strength of the present study is that it included a large number of patients (n = 1536). The cohort consisted of only revision ACLRs, with no multiligament injuries, over a period of 10 years throughout Denmark. All DKRR registrants include detailed descriptions of surgical techniques, making it possible to investigate the influence of factors on rare incidence outcomes such as re-revision surgery. The primary endpoint of re-revision surgery has been shown to be more sensitive to inferior outcome than patient-reported outcome measures. The information from the DKRR is of high reliability and quality, and we thus believe that the findings in this study are applicable to the general population.
A limitation of the study is the low level of completeness for patient-reported outcome measures, which is a data quality issue. Validation studies, however, have demonstrated no differences in outcome level and background profile between patients who report PROM values and those who do not. The 2 investigated cohorts differed in size, and this affected the comparisons made between them. In the comparison of preoperative subjective patient scores (KOOS and Tegner) we noted a difference in KOOS symptoms subscale results, but the rest of the values were not significantly different, so the two study groups were relatively comparable. Selection bias cannot be ruled out, as the data provided do not include information about hospital-dependent revision indications, surgeon preferences (in terms of graft size, fixation material, and technique), or surgeon experience.
Additionally, we had no information about postoperative rehabilitation programs or patient rehabilitation compliance. The registry lacks other relevant outcome data such as work ability, comorbidities, and radiographic parameters. The full cohort included 83 grafts of unknown type, which were excluded from outcome calculations in order to avoid potential bias from incorrect graft allocation. In the present study we did not divide the patient data into all graft subtypes, which would have given more precise information about graft performance. Both autograft and allograft entail different graft types (eg, with and without bone blocks), which can influence graft healing and subsequent failure rates. Revision rates do not reveal the patients who had rerupture and did not receive re-revision ACLR either because the patient did not want to or because the individual surgeon did not find an indication for reoperation.
Conclusion
In this observational population-based study, the re-revision rate was 2.2 times higher for allograft compared with autograft when corrected for age. Allograft use was associated with greater knee laxity at 1-year follow-up. However, subjective clinical outcomes and knee function were not inferior for allograft patients. These results indicate that autograft is a safer graft choice for revision ACLR.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was obtained from the Danish National Board of Health and the Danish Data Protection Agency.