
Abstract
Background:
Medial meniscus posterior root tears (MMPRTs) disrupt the integrity and hoop tension of the meniscus, leading to cartilage degeneration and accelerated osteoarthritis (OA) progression. The management of patients with MMPRT is controversial, and the efficacy of different treatment options is unclear.
Purpose:
To compare the clinical, radiographic, and magnetic resonance imaging (MRI) outcomes of patients with MMPRT between trans–posterior cruciate ligament (trans-PCL) all-inside repair and partial meniscectomy.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
We identified patients with MMPRT who underwent trans-PCL all-inside repair (group AR) or partial meniscectomy (group PM) between 2015 and 2019 at a single institution. The trans-PCL all-inside repair was performed by suturing the torn meniscus root to the PCL fibers. Patient-reported outcomes as well as radiographic and MRI outcomes were collected at baseline and final follow-up. Clinical failure was defined as conversion to total knee arthroplasty (TKA), and Kaplan-Meier survival analysis was used to investigate the survival rates of patients with different surgical procedures.
Results:
Included were 29 patients in group AR and 31 patients in group PM (mean age, 62.69 and 60.68 years, respectively; mean follow-up, 2.91 ± 1.33 and 3.45 ± 1.50 years, respectively). There were no differences in baseline patient characteristics between the groups. All patient-reported outcome scores improved significantly in both groups at the final follow-up. When we compared final outcomes between the groups, group AR had less joint space narrowing (P = .010), less Kellgren-Lawrence OA grade progression (P = .002), and less medial meniscal extrusion (MME; P = .002) than group PM. In addition, group AR showed less progression of bone marrow lesions and cartilage lesions (P < .05) than group PM. The rate of conversion to TKA was 6.90% in group AR and 29.0% in group PM. The 5-year survival rates in the AR and PM groups were 82.6% and 59.8%, respectively (P = .153).
Conclusion:
Trans-PCL all-inside repair for MMPRTs was associated with greater improvement in clinical function, better radiographic results, less MME and cartilage degeneration, and a lower rate of subsequent TKA compared with partial meniscectomy.
The meniscus absorbs and transmits compressive loads in the knee joint. Biomechanical and clinical studies have demonstrated a clear link between medial meniscus posterior root tear (MMPRT) and acceleration of the progression of knee osteoarthritis (OA). 1,14,24 MMPRTs are defined as avulsion injuries or radial tears within 10 mm of a bony attachment of the medial meniscus posterior horn. 30,33,38 These injuries significantly disrupt the normal structure of the meniscus and its function to distribute axial compressive loads, resulting in decreased contact surface areas and increased contact pressures of the joint. 25,29,31,32 Biomechanical studies have shown that the peak pressure of the medial compartment in MMPRTs increased by 25% compared with the normal knee, which was equivalent to the biomechanical effect of complete meniscectomy. 29
Arthroscopic repair by the transtibial pullout suture technique and anchor refixation are common techniques used to address MMPRT. Biomechanical studies have shown that these repairs could restore the integrity and biomechanical function of the meniscus, delaying cartilage degeneration and the progression of osteoarthritis. 31,32 Clinical studies assessing patients with root repairs documented encouraging clinical outcomes and satisfactory healing rates via second-look arthroscopy and magnetic resonance imaging (MRI), 5,7,12,28,36 demonstrating that root repairs could delay the progression of radiographic knee OA compared with meniscectomy. 7,12,15
Despite the encouraging results, these repair techniques still have several drawbacks. Repair techniques require accurate anatomical placement of the meniscus root, as even a 5-mm error in placement has been associated with increased joint contact loads. Deficient repair may lead to a decrease in contact area and an increase in contact pressure compared with the normal knee. 8,25,39 Transtibial pullout repair could carry the risk of suture abrasion in the bony tunnel and creep of the sutures, which would then reduce the strength of the repair and increase the rupture risk of the suture. 2,22 Suture anchor refixation is technically difficult and has the potential risk of fixation failure. 2 To date, there are no clear criteria throughout the published literature to support the best technique in terms of optimum results.
To overcome the shortcomings of existing repair techniques, a new trans–posterior cruciate ligament (trans-PCL) all-inside repair technique was developed that involves a simple suture fixing the torn root back to the adjacent PCL fibers with the all-inside suture device. Given the proximity of the medial meniscus posterior root to the most proximal PCL tibial attachment (which was directly 8.2 mm from the medial posterior root attachment center), 19 all-inside repair via suture fixation to the PCL could provide an analog to the Wrisberg ligament with the potential for decreased technical difficulty, increased speed, and fewer surgical incisions and complications (nerve and vessel injuries) as compared with other treatment options. The biomechanical effectiveness of trans-PCL all-inside repair with reconstruction of tibiofemoral contact mechanics compared with that of the intact knee in human cadaveric knee specimens has been demonstrated in Saltzman et al’s 35 report. However, there is a lack of clinical evidence to verify the safety and effectivity of trans-PCL all-inside repair. In addition, the restoration of meniscal stability and hoop tension should be tested from a clinical viewpoint.
In this study, we compared the clinical, radiographic, and MRI results of patients with MMPRTs who underwent either trans-PCL all-inside repair or partial meniscectomy to determine the clinical effect of these surgical techniques on OA progression. We hypothesized that the clinical, radiographic, and MRI results in patients who underwent trans-PCL all-inside repair would be better than in those who underwent partial meniscectomy, presuming that meniscus root refixation might delay the progression of knee OA.
Methods
Study Design
The protocol for this retrospective study received institutional review board approval. We identified consecutive patients with MMPRTs who underwent trans-PCL all-inside repair or partial meniscectomy at a single institution between 2015 and 2019. Included were patients with an isolated complete MMPRT confirmed by arthroscopy and knee OA evaluated as Kellgren-Lawrence (K-L) grade ≤2. 26 The exclusion criteria were patients with (1) concomitant multiple ligament injuries; (2) K-L grade 3 or 4; (3) >6 degrees malalignment (varus or valgus deformity); and (4) additional operative procedures such as ligament reconstruction, chondroplasty, microfracture and osteochondral autograft transplantation.
All arthroscopic surgeries were performed by the senior orthopaedic surgeon (T.S.). A pragmatic approach was adopted and all-inside repair was performed in patients when the quality of meniscus posterior roots was suitable for performing repair and the patient was willing to modify their lifestyle and use crutches and braces for 12 weeks after surgery. Patients who were not meeting the above conditions underwent partial meniscectomy.
Surgical Technique
Standard diagnostic knee arthroscopy with anterolateral and anteromedial portals was used. All-inside repair was performed with a suture device (FasT-Fix 360 Meniscal Repair System; Smith & Nephew, Endoscopic Division) by suturing the torn meniscus root to the adjacent PCL fibers. The first suture was inserted into the meniscus posterior horn 4 mm from the torn root edge, and the second suture was then inserted into the 5 mm lateral to the most medial edge of the PCL fibers. The depth limitation was 20 mm to prevent nerve and vascular injury. This process was repeated with a second all-inside suture into the posterior horn and nearby PCL fibers. The tension of the sutured meniscus was confirmed with a probe (Figure 1). Partial meniscectomy was performed with biters and a 4.5-mm shaver, the unstable part of meniscal tears were resected, and the retaining part was debrided to a stable and smooth shape. The resection range was determined according to tear type, tear location, and quality of meniscal tissue.
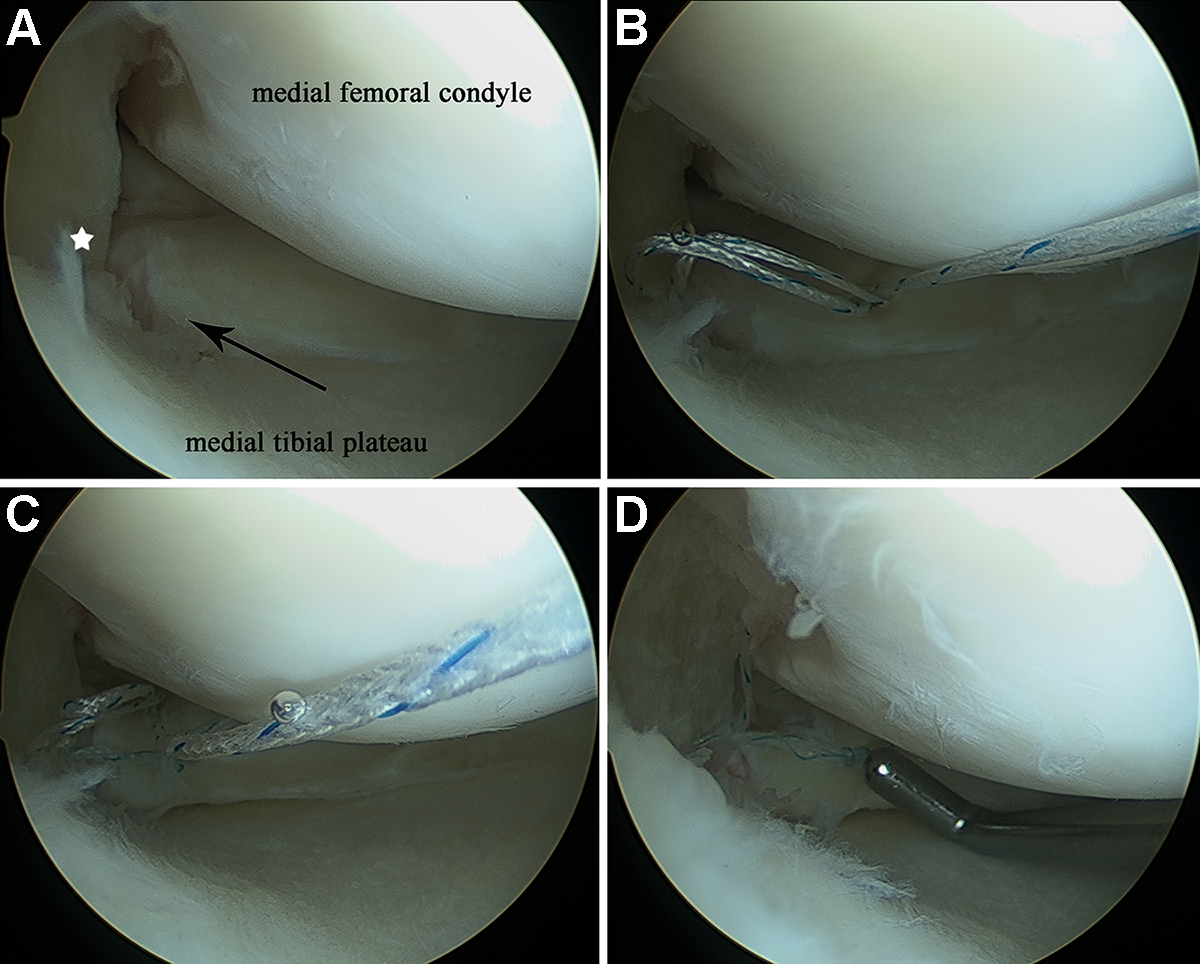
Arthroscopic pictures with a 30° arthroscope through the anterolateral portal showing medial meniscus posterior root tear refixation to the adjacent posterior cruciate ligament (PCL) by the all-inside repair technique. (A) The black arrow shows complete avulsion tear of medial meniscus posterior root; the white star indicates PCL fibers. (B) The torn meniscus root was refixed to the adjacent PCL fibers. (C) The process is repeated with a second all-inside suture placed on the meniscal horn posterior to the initially placed suture to provide stability. (D) Confirmation of meniscal tension and stability after refixation by probing.
Postoperative Rehabilitation
Lifestyle modifications were recommended to all patients. For patients who underwent trans-PCL all-inside repair, partial weightbearing (use of crutches or walking aid) and knee braces were worn for 3 months after surgery. In the initial 4 weeks, the braces were locked in full extension. The range of motion of the knee joint started at 30° at 4 weeks after surgery and increased by 30° per week. Full weightbearing and progressive closed kinetic chain strengthening exercises were allowed ≥3 months after surgery. For patients who underwent partial meniscectomy, bracing was not needed. Partial weightbearing and knee flexion exercises were allowed after surgery, and full weightbearing was allowed 1 month after surgery. For all patients, return to sports was allowed 6 months after surgery.
Clinical Evaluation
Patient demographics (sex, age, and body mass index [BMI]) and surgical details (history of knee surgery, side of knee injury, root tear location, mechanism of injury, K-L grade, knee alignment, and follow-up time) were recorded. Patient-reported outcomes were collected at baseline and final follow-up and included the Lysholm score, International Knee Documentation Committee (IKDC) subjective knee form, and the Knee injury and Osteoarthritis Outcome Score (KOOS) subscales (Symptoms, Pain, Activities of Daily Living [ADL], Sport and Recreation [Sport/Rec], and knee-related Quality of Life [QOL]).
For patients who were converted to total knee arthroplasty (TKA), the follow-up patient-reported outcomes were obtained immediately before TKA. The indications for TKA were as follows: (1) patients reported difficulty in walking and going up or down stairs due to unbearable knee pain; (2) knee joint with varus deformity and/or flexion contracture; or (3) radiography showed joint space narrowing (K-L grade 3 or 4), osteophytes, and sclerosis.
Radiographic Evaluation
Posteroanterior weightbearing knee radiographs at 45° of flexion (Rosenberg view 37 ) were performed at baseline and at final follow-up to evaluate the medial joint space width (m-JSW) and K-L grade. The m-JSW was measured at 25% of the width of the femur from the medial margin of the femur (Figure 2). 11 The K-L grading system was used to evaluate the degree of OA (grade 0, no degenerative change; grade 1, questionable osteophytes and no joint space narrowing; grade 2, definite osteophytes with possible joint space narrowing; grade 3, definite joint space narrowing with moderate multiple osteophytes and some sclerosis; and grade 4, severe joint space narrowing with cysts, osteophytes, and sclerosis). 20 All radiographic measurements were documented 3 times using a picture archiving and communication system (PACS); the averages of all measurements were recorded and used in our analysis. For patients who were converted to TKA, the follow-up radiographic outcomes were obtained immediately before TKA.

Landmarks and definition of coordinate system in radiography. Line A (x-axis) was found based on the femoral edge. Lines B (y-axis) and C are perpendicular to line A and at a tangent to the peripheral surface of the femoral condyle that continues from the articular surface. Medial joint space width was measured at 25% of the width of the femur from the medial margin of the femur.
MRI Evaluation
MRI was performed in all patients at baseline and in patients who were not converted to TKA at final follow-up. MRI was performed using a 1.5-T scanner (Magnetom Tim Trio; Siemens Medical Solutions) with a transmit-receive quadrature knee coil. The imaging protocol included sagittal T1-weighted spin-echo sequence (repetition time [TR]/echo time [TE], 400/9.4 ms; field of view [FOV],180 mm; matrix size, 320 × 224; slice thickness, 4.0 mm); sagittal, coronal, axial proton density–weighted fat-saturated sequence (TR/TE 2500/40 ms; FOV, 180 mm; matrix size, 320 × 224; slice thickness, 4.0 mm) and sagittal 2-dimensional dual-echo fast spin-echo sequence (TR/TE, 1000/13.8, 27.6, 41.4, 55.2, 69.0 ms; FOV = 160 mm; matrix size, 320 × 214; slice thickness, 3 mm), which was used for measuring T2 relaxation time.
Medial meniscal extrusion (MME) was defined as the distance from the medial edge of the tibial plateau to the periphery of the medial meniscus, which was measured on coronal MRI at the level of the medial collateral ligament. 21,23 Osteophytes were excluded for determining the tibial margin (Figure 3). 21

Medial meniscal extrusion was measured from the tangent perpendicular to the medial tibial edge (the right white line) and the peripheral edge of the medial meniscus (the left white line) on coronal magnetic resonance imaging at the level of the medial collateral ligament.
The MRI Osteoarthritis Knee Score (MOAKS) was used as a semiquantitative tool to evaluate the pathological features of knee OA, including bone marrow lesions (BMLs), cartilage lesions, and synovitis. The prevalence of BMLs, cartilage lesions, and synovitis in the medial tibiofemoral joint was evaluated at baseline and at final follow-up. Changes in MOAKS features over time were defined as “progression,” “no change,” and “improvement” according to preoperative scores and postoperative scores of each feature. 34 In addition, the medial femur (MF) was divided into 2 articular subregions (central [MFc], posterior [MFp]), and the medial tibia (MT) was divided into 3 subregions (anterior [MTa], central [MTc], posterior [MTp]) for further accurate assessment of changes in BMLs and cartilage. Region of interest segmentation and specific semiquantitative evaluation for each feature of knee OA have been described in previous studies. 17,34
The healing status of the meniscus root was evaluated in the group with all-inside repair (group AR), which was classified as follows: (1) complete healing (confirmed continuity in sagittal, coronal, and axial planes); (2) partial healing (loss of continuity in any 1 or 2 planes); or (3) nonhealing (loss of continuity in all planes). 4
The results were evaluated by an orthopaedic surgeon (J.S.) and a radiologist (H.W.) separately with the PACS.
Statistical Analysis
IBM SPSS Statistics Version 25.0 (IBM Corp, Armonk, NY, USA) was used for all statistical analyses. Statistical significance was set at 5% (P < .05). For continuous variables, normality was assessed (Shapiro-Wilk test). The independent t test was used to compare the distribution of normally distributed continuous variables, and the Mann-Whitney test was performed when the distribution departed from normality. The paired t test was used to compare both groups preoperatively and postoperatively. The Pearson chi-square test was used to compare unordered categorical variables, and when >20% of the expected frequencies were <5, the Fisher exact test was used. For ordered categorical variables, the Mann-Whitney test was used.
A Kaplan-Meier survival analysis with the log-rank test was used to visualize and compare the survivorship of trans-PCL all-inside repair compared with partial meniscectomy. In addition, the groups were divided into short-term follow-up (≤3 years) and middle-term follow-up (>3 years) for further subgroup analysis.
To test the reliability of the OA measurements, the radiographic and MRI parameters (m-JSW, K-L grade, MME, BML, cartilage defects, and synovitis) were measured by 2 clinical fellows (J.S. and Y.P.) in all knees twice within a 1-month interval. For each measurement, the intraclass correlation coefficient (continuous variables) and kappa value (categorical variables) of interobserver reliability were >0.80, indicating good agreement (Appendix Table A1).
Results
We identified 112 patients with MMPRTs who underwent trans-PCL all-inside repair or partial meniscectomy during the study period. A total of 67 patients were included in the study based on inclusion criteria. Of these, 29 patients in the trans-PCL all-inside repair group (group AR) and 31 patients in the partial meniscectomy group (group PM) had adequate follow-up during the data collection period, and 7 patients were lost to follow-up (89.6% retention rate). Figure 4 shows a patient flowchart for the AR and PM groups (mean follow-up, 2.91 ± 1.33 and 3.45 ± 1.50 years, respectively). The mean age of the AR and PM groups was 62.69 and 60.68 years, respectively, and the mean BMI was 26.21 and 26.04, respectively. There were no significant differences between the AR and PM groups with respect to age, sex, injury side, or BMI (Table 1).
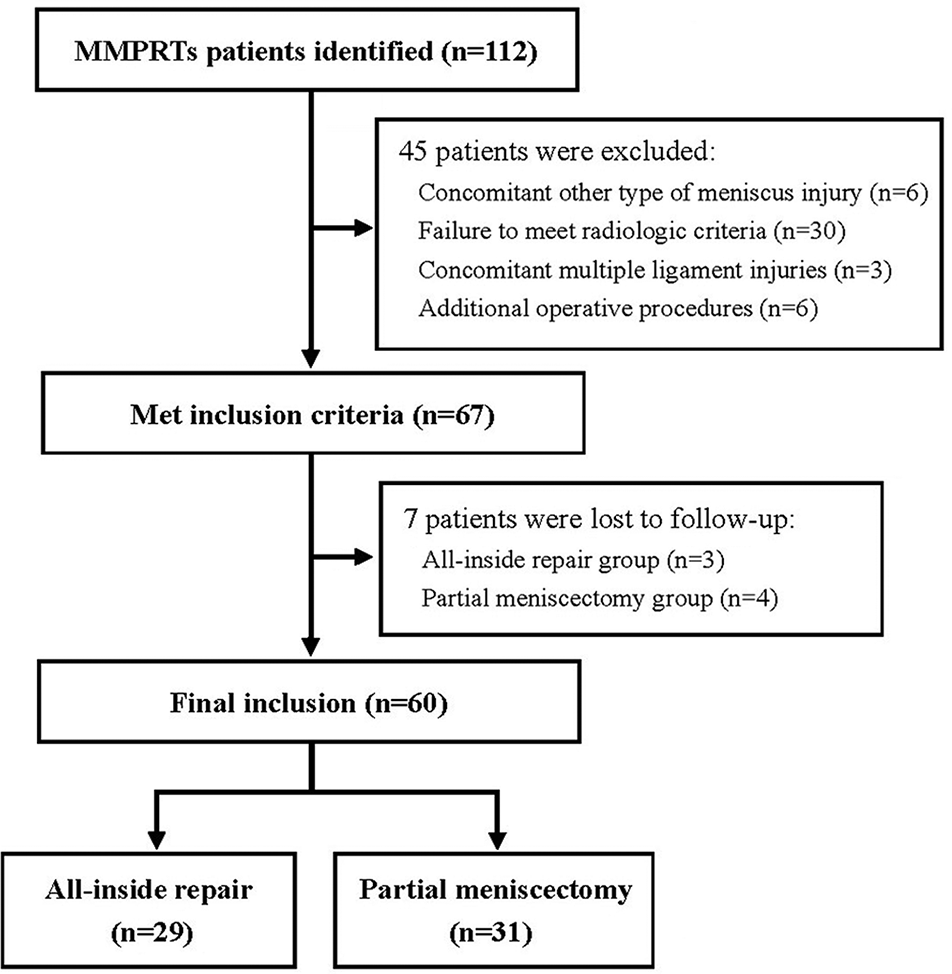
Flowchart of included participants. MMPRT, medial meniscus posterior root tear.
Baseline Patient and Clinical Characteristics a

a Data are expressed as mean ± SD or n unless otherwise indicated. Boldface P value indicates statistically significant difference between groups (P < .05). ADL, Activities of Daily Living; AR, all-inside repair; BMI, body mass index; BML, bone marrow lesion; IKDC, International Knee Documentation Committee; K-L, Kellgren-Lawrence; KOOS, Knee injury and Osteoarthritis Outcome Score; m-JSW, medial joint space width; MME, medial meniscal extrusion; MRI, magnetic resonance imaging; NA, not applicable; PM, partial meniscectomy; QOL, Quality of Life; Sport/Rec, Sport and Recreation.
Clinical Outcomes
Baseline patient-reported outcomes showed no significant differences between the AR and PM groups with respect to Lysholm, IKDC, or the KOOS Symptoms, Pain, Sport/Rec, or QOL subscale scores. However, baseline KOOS ADL scores were lower in the AR group (34.03 ± 10.83) than in the PM group (41.13 ± 11.86) (P = .009) (Table 1). Regarding the results at the final follow-up, there were no significant differences between the AR and PM groups for the Lysholm, IKDC, and all KOOS subscales (Table 2).
Comparison of Postoperative Clinical, Radiographic, and MRI Outcomes Between Groups at Final Follow-up a
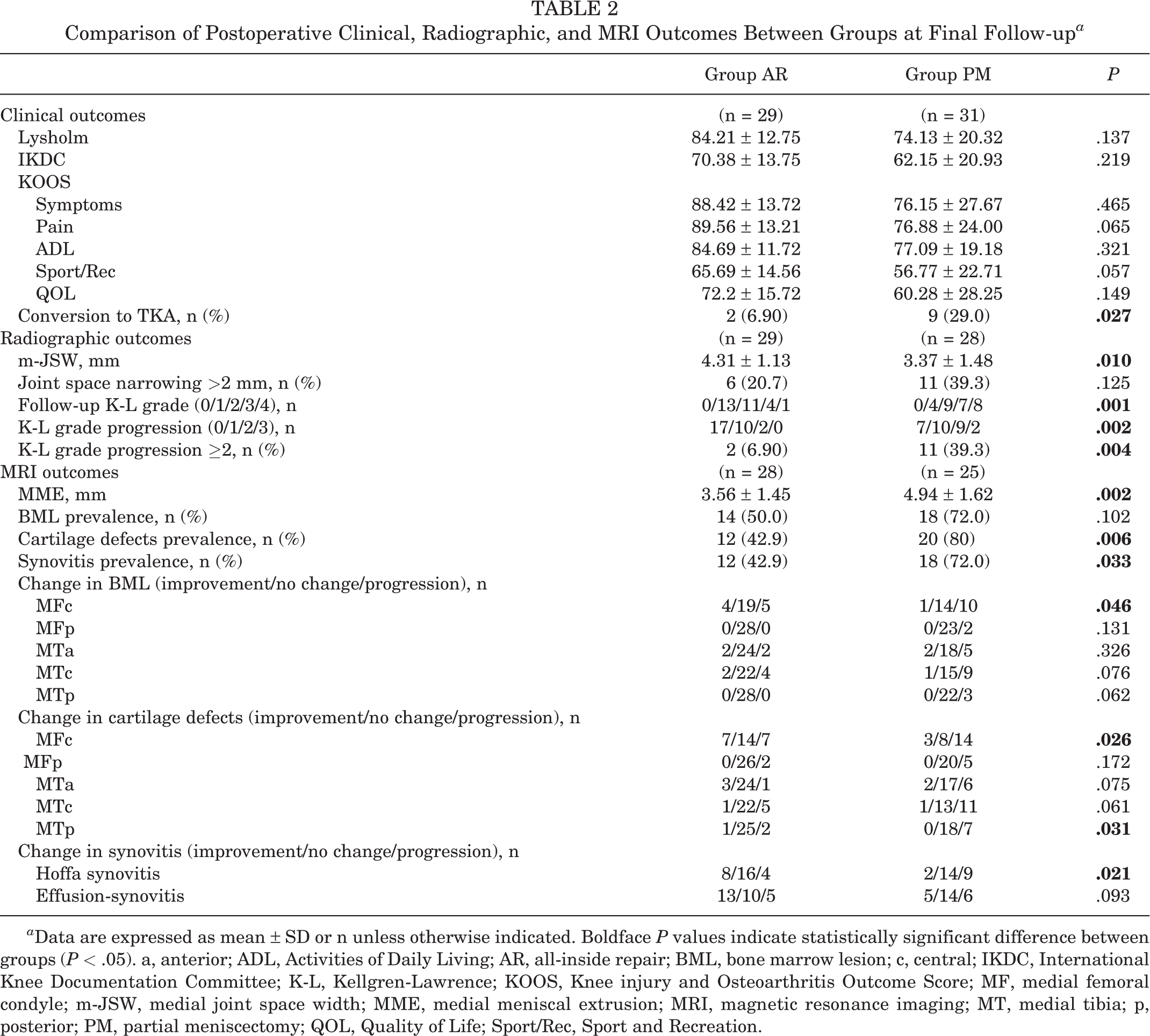
a Data are expressed as mean ± SD or n unless otherwise indicated. Boldface P values indicate statistically significant difference between groups (P < .05). a, anterior; ADL, Activities of Daily Living; AR, all-inside repair; BML, bone marrow lesion; c, central; IKDC, International Knee Documentation Committee; K-L, Kellgren-Lawrence; KOOS, Knee injury and Osteoarthritis Outcome Score; MF, medial femoral condyle; m-JSW, medial joint space width; MME, medial meniscal extrusion; MRI, magnetic resonance imaging; MT, medial tibia; p, posterior; PM, partial meniscectomy; QOL, Quality of Life; Sport/Rec, Sport and Recreation.
Within-group analysis was performed to determine the differences from baseline to the final follow-up for the AR and PM groups. The patient-reported outcomes in both groups were significantly improved from baseline to the final follow-up. Between-group analysis showed greater improvements from baseline to the final follow-up for group AR than for group PM with respect to IKDC (P = .027), KOOS Symptoms (P = .033), KOOS Pain (P = .002), KOOS ADL (P < .001), KOOS Sport/Rec (P = .004), and KOOS QOL (P = .008) (Table 3). However, for Lysholm scores, there were no significant differences between the groups.
Within-Group Changes (Δ) in Clinical, Radiographic, and MRI Outcomes From Baseline to Follow-up a

a Data are expressed as mean ± SD. Boldface P values indicate statistically significant difference between groups AR and PM (P < .05). ADL, Activities of Daily Living; AR, all-inside repair; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; MME, medial meniscal extrusion; MRI, magnetic resonance imaging; PM, partial meniscectomy; post, postoperative; pre, preoperative; QOL, Quality of Life; Sport/Rec, Sport and Recreation.
Radiographic Outcomes
As the radiographs of 3 patients in group PM before TKA were not posteroanterior weightbearing knee radiographs with 45° of flexion (Rosenberg view), they were excluded when we compared radiographic outcomes between the groups. There were no significant differences in baseline m-JSW or K-L grades between the groups when the 3 patients in the PM group were excluded (Table 2).
At final follow-up, 20.7% of patients (6 of 29) in group AR showed severe joint space narrowing (>2 mm), and 6.90% (2 of 29) showed severe K-L grade progression (≥2 grades). In the PM group, 39.3% of patients (11 of 28) showed a more severe joint space narrowing (>2 mm), and 39.3% (11 of 28) showed severe K-L grade progression (≥2 grades) (Table 2). Group AR showed better m-JSW (P = .010) and less K-L grade progression (P = .002) than group PM (Table 2) at the final follow-up. In addition, group AR had less progression of osteoarthritis compared with group PM, with less joint space narrowing (P = .009) (Table 3) and a lower rate of severe K-L grade progression (P = .004) (Table 2).
In the subgroup analysis according to follow-up time, both groups showed OA progression according to K-L grade at short-term (≤3 years) and medium-term (>3 years) follow-up. Group AR showed less K-L grade progression in the medium-term follow-up than group PM (P = .013), whereas for the short-term follow-up, the differences were not significant (Table 4).
Subgroup Analysis of Radiographic and MRI Outcomes Between Groups at Final Follow-up a

a Data are expressed as mean ± SD or n. Boldface P values indicate statistically significant difference between groups AR and PM (P < .05). AR, all-inside repair; K-L, Kellgren-Lawrence; MME, medial meniscal extrusion; MRI, magnetic resonance imaging; PM, partial meniscectomy.
MRI Outcomes
The baseline MRI was performed in all patients; 1 patient in group AR and 6 patients in group PM did not accept MRI examination at final follow-up before TKA. Thus, there were 28 patients in group AR and 25 patients in group PM who were included in the MRI evaluation. Although the 7 patients were excluded from the MRI evaluation, there were no significant differences in baseline data between the AR and PM groups, especially with respect to MME and the prevalence of BMLs, cartilage lesions, and synovitis.
In the AR group, 35.71% of patients (10/28) showed a reduction in MME, and 64.29% of patients (18/28) showed progression of MME. However, group AR had less progression of MME compared with group PM (P = .002) (Table 2). In addition, group AR showed less MME than group PM in both short-term follow-up (≤3 years) and medium term follow-up (>3 years) (Table 4).
Group PM showed more severe cartilage lesions (P = .006) and synovitis (P = .033) than group AR at the final follow-up. However, there were no significant differences in the prevalence of BML between the groups. Regarding the changes in MOAKS features over time, progression of BMLs and cartilage lesions was found in both groups, especially in the weightbearing area of the medial compartment. Group AR showed less progression of BML in MFc (P = .046) and less progression of cartilage lesions in MFc (P = .026) and MTp (P = .031) than Group PM (Table 2).
With respect to the healing status of the meniscus root in group AR, 60.71% of patients (17/28) showed complete healing (Figure 5), 32.14% of patients (9/28) showed partial healing, and 7.14% of patients (2/28) showed nonhealing.

Postoperative magnetic resonance imaging demonstrating complete healing of medial meniscus posterior root (arrows). (A) Sagittal image. (B) Coronal image. (C) Axial image.
Survival Analysis
There were 29 patients in group AR and 31 patients in group PM who were included in the survival analysis, and 6.90% of patients (2/29) in group AR and 29.0% of patients (9/31) in group PM underwent conversion to TKA without other surgical treatments. Group AR reduced the risk of TKA in the MMPRTs, with an relative risk of 0.238 (P = .027). The Kaplan-Meier survival curve with the percentage of patients free from conversion to TKA is shown in Figure 6. The overall Kaplan-Meier probability of survival after trans-PCL all-inside repair was 94.4% at 3 years and 82.6% at 5 years, whereas that for partial meniscectomy was 82.7% at 3 years and 59.8% at 5 years. However, there were no significant differences in Kaplan-Meier survival curves between the AR and PM groups with the log-rank test (P = .153) (Figure 6).
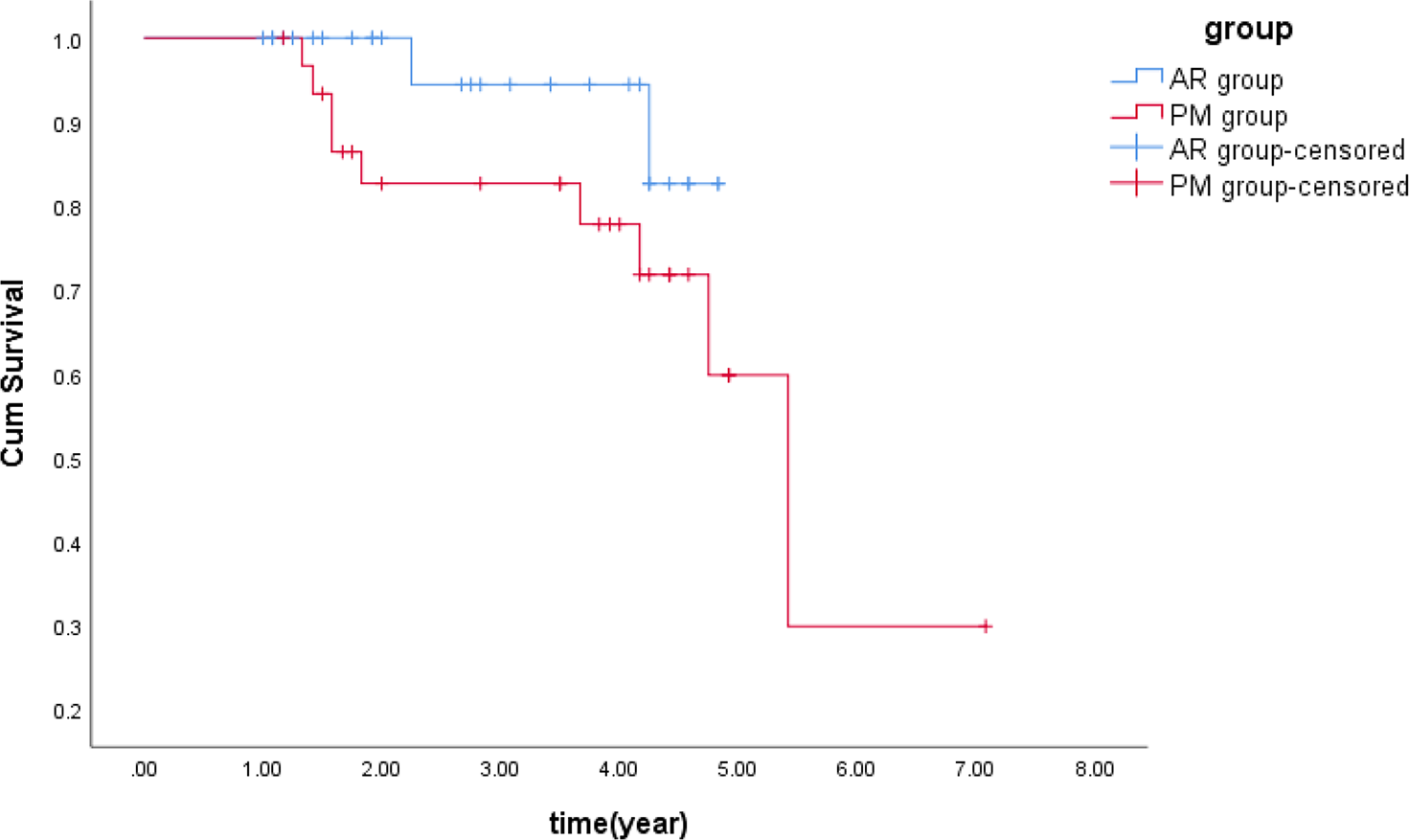
Kaplan-Meier survival curve demonstrating conversion to total knee arthroplasty by trans–posterior cruciate ligament all-inside repair (AR) (blue line) and partial meniscectomy (PM) (red line) in medial meniscus posterior root tear patients.
Discussion
The major finding of our study was that, compared with partial meniscectomy, trans-PCL all-inside repair in MMPRTs was associated with greater improvement of clinical function, better radiographic results, less MME, and cartilage degeneration, and a lower rate of conversion to TKA.
To date, there are no clear criteria throughout the published literature to support the best technique in terms of optimum results. Some studies have demonstrated that meniscectomy could provide symptomatic relief in short- to medium-term follow-up, 7,23 but showed significant OA progression and a high rate of TKA conversion in long-term follow-up, with 10-year survival rates of 44%. 6 Our study reported similar outcomes with a significant subjective functional improvement and symptomatic relief in the group PM, whereas 39.3% of patients showed severe K-L grade progression, and 29.0% converted to TKA. Compared with transtibial pullout repair and suture anchor repair techniques, trans-PCL all-inside repair avoids the need for tibial bone tunnels and high posteromedial portals with the suture of meniscus root to the adjacent PCL fibers with the potential for decreased technical difficulty, increased speed, and fewer surgical incisions and complications, considered a less invasive, less surgically demanding option than the above 2 techniques. Saltzman et al 35 demonstrated the biomechanical effectiveness of the repair via suture fixation of MMPRTs to the nearby PCL in a human cadaveric knee, which could improve contact area, mean contact pressure, and peak contact pressure compared with the mechanics of the “torn” condition, to a level that was not significantly different from the native knee. Dragoo et al 8 performed a similar repair technique in patients with meniscus root tears and reported that all-inside repair showed better clinical outcomes and lower rates of TKA conversion than conservative treatment, suggesting that surgical repair has a functional outcome benefit in elderly MMPRT patients. Our study was the first to compare the clinical, radiographic, and MRI outcomes of trans-PCL all-inside repair and partial meniscectomy.
Radiographic outcomes such as m-JSW and K-L grade are considered important indicators of the onset and progression of knee OA. When comparing the final outcomes in the current study, trans-PCL all-inside repair reduced the risk of severe K-L progression, effectively slowing down the onset and progression of knee OA. Regarding the failure rate, group AR (2/29) exhibited a lower rate of conversion to TKA than group PM (9/31). MME is a highly significant risk factor for degenerative cartilage damage and progressive arthritic changes. 18,27 Lee et al 27 described that the amount of extrusion, rather than the location of the meniscal tear, was the most important determinant of subsequent osteoarthritis severity. Kim et al 21 found that there was no significant difference between meniscal repair and partial meniscectomy in terms of MME. A meta-analysis showed little change in MME after meniscal repair in patients with MMPRTs. 3 In addition, a systematic review showed that a reduction in MME was achieved in only 56% of patients who underwent meniscal repair. 13 Meniscal extrusion had progressed at 1 year postoperatively in 76% of the transtibial pullout repair cases. 40 Our study demonstrated similar results; only 35% of patients in group AR showed a reduction in MME after surgery, which indicated that meniscus root repair could not prevent MME progression in all patients. However, all patients in the PM group showed MME progression at the final follow-up compared with the AR group.
Knee OA is likely precipitated by a destabilizing medial meniscus root tear in a joint compromised by the presence of multiple structural abnormalities (eg, large BMLs, cartilage loss, meniscal damage in ≥2 regions, large effusion-synovitis volumes). 9,10 The MOAKS semiquantitative tool was used to provide a more comprehensive and accurate assessment of the condition of the whole joint, including cartilage lesions, BMLs, and synovitis. Cartilage lesions are commonly defined as the initial phase of osteoarthritis. 16 A meta-analysis by Chung et al 3 evaluated the outcomes of the progression of cartilage lesions using the Outerbridge classification and found that a minimum of 75% or a maximum of 88.5% of patients with MMPRTs can delay cartilage injury via MMPRT repair. We found that group AR showed better outcomes in terms of cartilage condition and synovitis than group PM at final follow-up. In addition, progression of BMLs and cartilage was found in both groups in the weightbearing area of the medial compartment. However, group AR showed less progression of BMLs in MFc and less progression of cartilage lesions in MFc and MTp. Thus, although trans-PCL all-inside repair could not reduce MME completely, this repair procedure seemed to be an effective option for MMPRTs in terms of delaying the degeneration of cartilage and progression of BMLs by maintaining meniscal integrity and hoop tension to a certain degree.
Limitations
There are several limitations to this study. First, it is a nonrandomized, retrospective comparative study with a small sample size and short-term follow-up. Patients with poor quality of meniscus posterior roots, or who were unwilling to modify their lifestyle to comply with a strict rehabilitation, underwent partial meniscectomy. Thus, there is selection bias in surgical indication of meniscal repair and partial meniscectomy. Second, the actual meniscal healing and restoration of hoop tension after surgery were not assessed because second-look arthroscopy was not performed. Third, the results of other surgical procedures, including transtibial pullout repair and suture anchor, were not investigated. Additional prospective randomized controlled studies with long-term follow-up and large sample sizes comparing several management techniques, including trans-PCL all-inside refixation, transtibial pullout fixation, and suture anchor refixation, will be needed in the future.
Conclusion
In MMPRTs, compared with partial meniscectomy, trans-PCL all-inside repair was associated with greater improvement of clinical function, better radiographic results, less MME and cartilage degeneration, and a lower rate of subsequent TKA.
Footnotes
Final revision submitted February 3, 2023; accepted February 26, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: Funding was received from the Peking University People’s Hospital Research Development Fund (grant/award No.: RDL2020-05). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
J.S. and H.W. contributed equally to this article.
Ethical approval for this study was obtained from Peking University, People’s Hospital (No. 2019PHB116-01).
Appendix
Interobserver Reliability of Radiological and MRI OA Assessments a

| Variable | ICC or κ b |
|---|---|
| m-JSW | 0.913 |
| MME | 0.974 |
| K-L grade | 0.831 |
| BML | |
| MFc | 0.907 |
| MFp | 1 |
| MTa | 0.874 |
| MTc | 0.873 |
| MTp | 0.826 |
| Cartilage defects | |
| MFc | 0.867 |
| MFp | 0.861 |
| MTa | 0.897 |
| MTc | 0.891 |
| MTp | 0.839 |
| Synovitis | |
| Hoffa synovitis | 0.899 |
| Effusion-synovitis | 0.9 |
a Associated P values for all reliability values were <.001. a, anterior; BML, bone marrow lesion; c, central; ICC, intraclass correlation coefficient; K-L, Kellgren-Lawrence; MF, medial femoral condyle; m-JSW, medial joint space width; MME, medial meniscal extrusion; MT, medial tibia; OA, osteoarthritis; p, posterior.
b The ICC was used to calculate the interobserver reliability of continuous variables (m-JSW and MME) and the κ coefficient was used to calculate the interobserver reliability of categorical variables (K-L grade, BML, cartilage defect, and synovitis).