
Abstract
Background:
The medial meniscus posterior root tear (MMPRT) is a contributing factor to osteoarthritis (OA). The Coronal Plane Alignment of the Knee (CPAK) classification is a method for characterizing knee alignment phenotypes by incorporating the arithmetic hip–knee–ankle (aHKA) and the joint line obliquity (JLO).
Purpose:
To evaluate the CPAK type in patients with MMPRT while comparing the radiographic parameters between the MMPRT knees and the unaffected knees.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A total of 74 patients with MMPRT, including 87 knees, were confirmed using magnetic resonance imaging. Radiographic parameters of long-leg radiographs were measured separately by 2 reviewers at 2 different time points to classify the CPAK phenotypes, where the neutral aHKA was determined by 0°± 2° and neutral JLO by 180°± 3°.
Results:
Patients with MMPRT were predominantly women (72.97%), with a mean age of 55.1 ± 9.3 years and a body mass index of 27.7 kg/m2. Among 74 patients, 13 had bilateral MMPRT. According to a mean aHKA of −2°± 3.4° and JLO of 173.9°± 4.2°, a total of 87 MMPRT knees tended to demonstrate varus (41.4%) to neutral (49.4%) alignment, and apex distal JLO (73.4%). The CPAK distribution of MMPRT was type 2 (39.1%), type 1 (28.7%), type 4 (11.5%), type 5 (10.3%), type 3 (5.6%), type 6 (3.5%), and type 7 (1.2%); types 8 and 9 were not found. There was no difference in CPAK distribution between the MMPRT knees and the non-affected knees. The intra- (0.74) and interrater (0.80) reliability of the CPAK classification were in substantial agreement. The intrarater reliability for the lateral distal femoral angle (LDFA) and the medial proximal tibial angle (MPTA) was good (intraclass correlation coefficient [ICC] = 0.89). Interrater reliability was excellent for the LDFA (ICC = 0.91) and MPTA (ICC = 0.93).
Conclusion:
Among patients with MMPRT, the most common CPAK phenotypes are types 2, 1, and 4, respectively. Most patients had an apex-distal JLO and varus-to-neutral alignment. These findings suggest that apex distal JLO may be a contributing factor for the development of MMPRT.
The medial meniscus posterior root tear (MMPRT) is a clinically important subtype of meniscal injury, constituting approximately 15% to 20% of all meniscal tears.6,26 These injuries occur within 1 cm of the meniscal root attachment and are especially prevalent in middle-aged and older adults, particularly in populations engaged in repetitive deep flexion activities.1,3,6,13,15,18 MMPRT severely impairs the meniscus's role in transmitting circumferential hoop stress and distributing load, leading to significant joint space narrowing and accelerated osteoarthritis (OA).2,3,8,18,26
The Coronal Plane Alignment of the Knee (CPAK) classification is a phenotype-based system that integrates the arithmetic Hip–Knee–Ankle angle (aHKA) and the joint line obliquity (JLO) to describe knee alignment across 9 distinct types. 14 Among healthy individuals and those with early-stage OA, type 2 is most commonly observed.14,16,19, 20, 21,22,25 In contrast, type 1, characterized by constitutional varus and apex distal JLO, becomes increasingly prevalent in patients with advanced OA, with studies5,9,16,20,25 reporting rates exceeding 50%.
Previous studies have identified several anatomical risk factors for MMPRT, such as varus alignment and tibial slope.4,7,17 However, none have investigated this within the context of a standardized coronal alignment phenotype like the CPAK classification. 14 This represents a key knowledge gap, as the CPAK offers a reproducible framework that could improve risk stratification. Understanding the association between CPAK types and MMPRT may help identify high-risk individuals earlier and inform preventive strategies before irreversible joint degeneration occurs.
This study aimed to evaluate the type of CPAK in patients with MMPRT and to compare radiographic parameters between MMPRT knees and unaffected knees.
Methods
Study Design and Participants
This cross-sectional etiologic study was conducted by reviewing the medical records database at Thammasat University Hospital between January 2015 and March 2025. The research was approved by the ethics committee of Thammasat University Hospital (Registration No. MTU-EC-SA-0-128/68).
Inclusion Criteria
Participants were Thai, aged between 18 and 80 years, and had been diagnosed with MMPRT, confirmed using magnetic resonance imaging (MRI), and reviewed by orthopaedic surgeons (A.A.) and musculoskeletal radiologists. Diagnostic MRI findings included the presence of the cleft sign, ghost sign, meniscal extrusion >3 mm, or a tear involving the posterior root or within 10 mm adjacent to the posterior root of the medial meniscus. All participants were required to have long-leg standing radiographs performed before or after MRI within 6 months of the MRI.
Exclusion Criteria
Participants were excluded if they had a history of previous osteotomy, inadequate imaging quality, flexion contracture >5°, advanced OA (Kellgren-Lawrence [KL] grade 4), or significant bone loss, acute trauma or multiligamentous injury, rheumatoid arthritis or other inflammatory joint diseases, metabolic bone disease, extra-articular deformity, congenital or developmental limb deformities, or neuromuscular disorders.
Data Collection
Descriptive data for each participant were recorded from the medical record system, including sex, age (in years), and body mass index (BMI) at the onset of the condition. The affected knee sides were also noted.
Radiographic assessment was performed using long-leg standing radiographs, which were independently analyzed by 2 trained reviewers (5th-year medical student, N.L., and W.D.) to classify the CPAK phenotype for each knee. To assess intra- and interrater reliability, each reviewer performed all measurements twice with a 2-week interval between assessments. The radiographic parameters measured included the mechanical hip–knee–ankle angle (mHKA), which represents the angle between the mechanical axes of the femur and tibia intersecting at the knee joint center and is used to determine leg alignment as either varus or valgus. The medial proximal tibial angle (MPTA) and lateral distal femoral angle (LDFA) were also measured, representing the angles between the respective joint lines and mechanical axes of the tibia and femur. The arithmetic aHKA was calculated as the difference between MPTA and LDFA (aHKA = MPTA − LDFA). Alignment was classified based on aHKA as follows: varus alignment for aHKA <–2°, neutral alignment for aHKA between −2° and +2°, and valgus alignment for aHKA >+2°. The JLO, determined by summing the MPTA and LDFA (JLO = MPTA + LDFA), was used to evaluate the slope of the joint line, which was classified as follows: apex distal obliquity (JLO <177°), neutral obliquity (JLO between 177° and 183°), and apex proximal obliquity (JLO >183°). Based on the combination of alignment and JLO classifications, knees were categorized into 9 CPAK phenotypes: type 1 (varus alignment and apex distal JLO), type 2 (neutral alignment and apex distal JLO), type 3 (valgus alignment and apex distal JLO), type 4 (varus alignment and neutral JLO), type 5 (neutral alignment and neutral JLO), type 6 (valgus alignment and neutral JLO), type 7 (varus alignment and apex proximal JLO), type 8 (neutral alignment and apex proximal JLO), and type 9 (valgus alignment and apex proximal JLO). 14 Additional radiographic parameters included the mechanical axis deviation (MAD), defined as the perpendicular distance from the center of the knee joint to the mechanical axis line, and the joint line convergence angle, which is the angle between tangent lines drawn to the femoral condyles and the tibial plateau. The tibiofemoral angle was also measured, defined as the angle formed by the intersection of the anatomical axes of the femur and tibia at the center of the knee joint. This measurement was used to preliminarily assess lower-limb alignment, indicating whether the knee exhibited a varus or valgus deformity. Lastly, meniscal extrusion was also measured on the affected knee's MRI, defined as the distance the medial meniscus extended beyond the edge of the tibial plateau on mid-coronal MRI sequences.
Data Analysis
According to a previous study, 21 the prevalence of distal apex joint-line obliquity in the general population was approximately 76.9%. Using this proportion (P = .769), a margin of error (Δ) of 0.1, and a confidence level of 95% (α = .05; Z = 1.959964), the required sample size was calculated using the n4Studies application for estimating a proportion in an infinite population. The resulting sample size was 70 knees.
All data were analyzed using descriptive and reliability statistics. Continuous variables—including age, BMI, LDFA, MPTA, JLO, aHKA, MAD, JLCA, and medial meniscal extrusion—were reported as means with standard deviations and 95% CIs. Categorical variables, such as sex, affected side, and KL grade, were summarized as counts and percentages. The distribution of CPAK types was presented as proportions. To assess the consistency of CPAK classification, both intra- and interrater reliability were calculated using Cohen's kappa coefficient and the intraclass correlation coefficient (ICC). The kappa (k) <0.00 was considered poor strength of agreement; 0.00 to 0.20, slight; 0.21 to 0.40, fair; 0.41 to 0.60, moderate; 0.61 to 0.80, substantial; and 0.81 to 1.00, almost perfect.10,12 The ICC values <0.5, 0.5-0.75, 0.75-0.9, and >0.90 indicate poor, moderate, good, and excellent reliability, respectively.10,23 All statistical analyses were performed using STATA Version 14.2. P < .05 was considered statistically significant.
Results
A total of 74 patients with MMPRT were included in this study, with a mean age of 55 years. The majority were women (73%), and the mean BMI was 27.7 kg/m2. The affected knee was the right side in 47% of patients and bilateral in 18%. Descriptive data of patients are presented in Table 1.
Descriptive Data of the Study Population a

Data are presented as mean ± SD or n (%). BMI, body mass index.
Radiographic analysis was performed on 87 affected knees. The mean mHKA was −4.1°± 3.7°, consistent with varus alignment. The mean LDFA was 87.9°± 2.5°, and the mean MPTA was 86°± 2.9°. No knees demonstrated a KL grade 4. The mean medial meniscal extrusion was 3.9 mm. The radiographic parameters are summarized in Table 2.
The Radiographic Parameters of the Study Population a
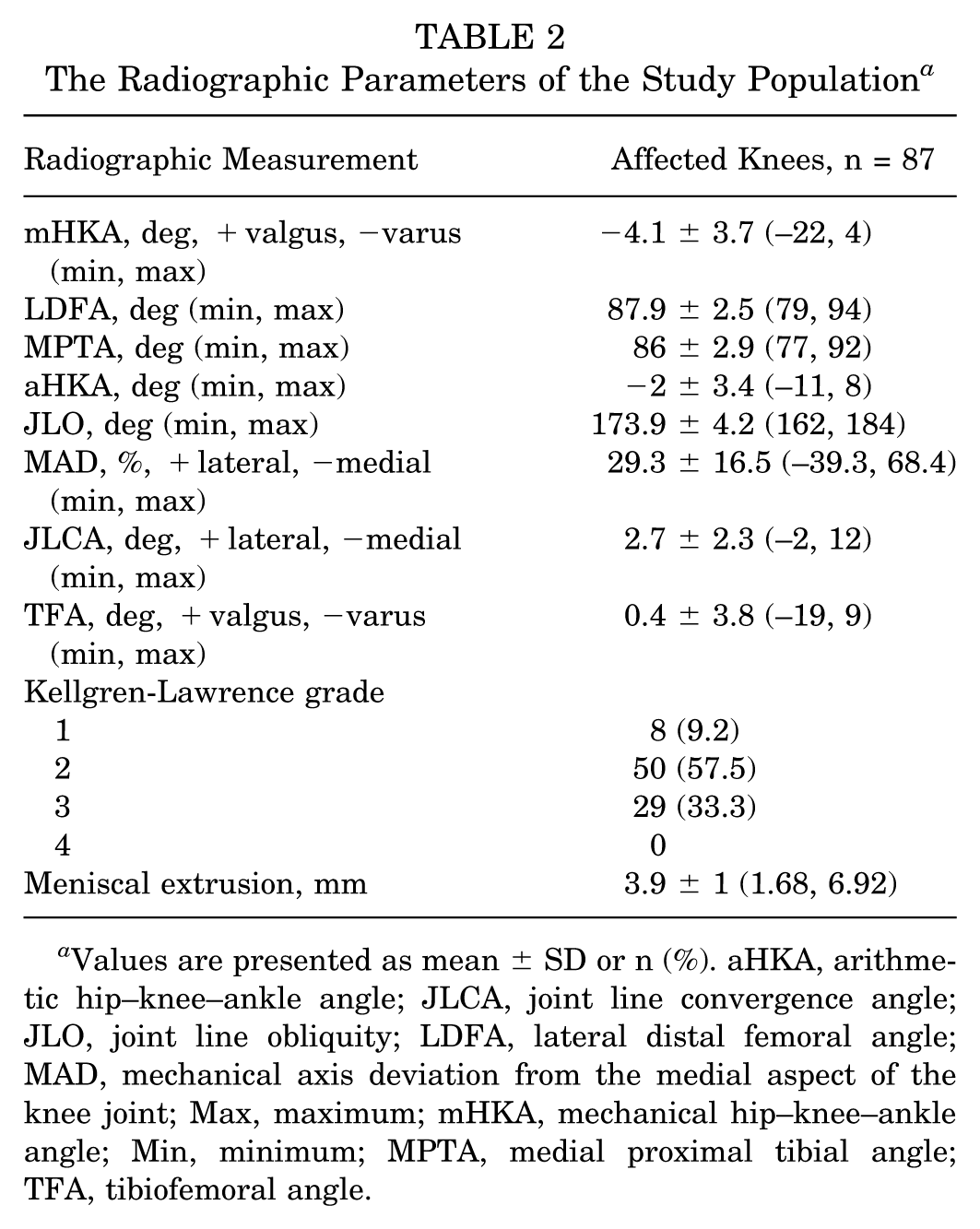
Values are presented as mean ± SD or n (%). aHKA, arithmetic hip–knee–ankle angle; JLCA, joint line convergence angle; JLO, joint line obliquity; LDFA, lateral distal femoral angle; MAD, mechanical axis deviation from the medial aspect of the knee joint; Max, maximum; mHKA, mechanical hip–knee–ankle angle; Min, minimum; MPTA, medial proximal tibial angle; TFA, tibiofemoral angle.
The CPAK type classification was plotted in Figure 1. The most frequently observed phenotypes were type 2 (39.1%) and type 1 (28.7%). Less common phenotypes included type 6 (3.5%) and type 7 (1.2%), while types 8 and 9 were not observed.

The CPAK type classification in populations with MMPRT. aKHA, arithmetic hip–knee–ankle angle; CPAK, coronal plane alignment of the knee; LDFA, lateral distal femoral angle; MMPRT, medial meniscus posterior root tear; MPTA, medial proximal tibial angle.
The radiographic parameters and CPAK classification were analyzed in 61 patients with unilateral MMPRTs (Table 3). No statistically significant differences were found in CPAK classification and radiographic parameters between affected and non-affected knees. However, the higher KL grade was found in the affected knees.
The Radiographic Parameters and CPAK Classification Comparison Between Affected and Nonaffected Knees a

Data are presented as mean (SD) [95% CI] or n (%). P values were analyzed using a paired t test. aHKA, arithmetic hip–knee–ankle angle; CPAK, coronal plane alignment of the knee; JLCA, joint line convergence angle; JLO, joint line obliquity; LDFA, lateral distal femoral angle; MAD, mechanical axis deviation; mHKA, mechanical hip–knee–ankle angle; MMRT, medial meniscus root tear; MPTA, medial proximal tibial angle; and TFA, tibiofemoral angle.
Analyzed with the Bowker test of paired categorical data.
The radiographic parameters and CPAK classification type were independently assessed by 2 observers (N.L., W.D.), who performed each assessment twice with a 2-week interval between evaluations. The reliability analyses are shown in Table 4. Intrarater reliability for the LDFA and MPTA was good. Interrater reliability was excellent for both parameters. The CPAK classification showed substantial intrarater agreement and moderate interrater agreement.
Reliability Test of the Measurement Parameters a
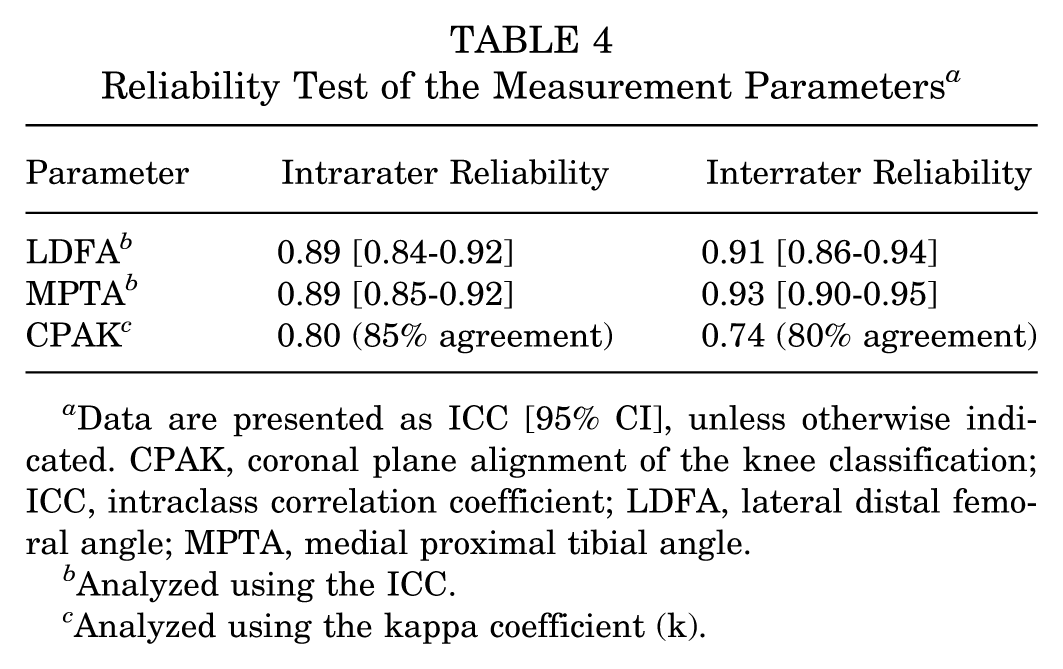
Data are presented as ICC [95% CI], unless otherwise indicated. CPAK, coronal plane alignment of the knee classification; ICC, intraclass correlation coefficient; LDFA, lateral distal femoral angle; MPTA, medial proximal tibial angle.
Analyzed using the ICC.
Analyzed using the kappa coefficient (k).
Discussion
The study results highlight that not only varus alignment (41.4%), but also the apex distal JLO, is a key feature in patients with MMPRT (73.4%). The most frequently observed CPAK phenotypes were type 2 (39.1%), type 1 (28.7%), and type 4 (11.5%), respectively. The mean mHKA and aHKA values were −4.1° and −2°, respectively, with an apex distal JLO averaging 174°. CPAK phenotypes did not differ significantly between affected and contralateral knees.
Our findings are consistent with previous literature describing coronal plane alignment patterns and CPAK phenotypes in knees with medial compartment pathology. The CPAK classification 14 combines the arithmetic aHKA and JLO to describe knee alignment in both healthy and osteoarthritic knees. They observed that type 2 (neutral alignment with apex-distal JLO) was most common in healthy knees, whereas type 1 (varus alignment with apex-distal JLO) predominated in knees with OA. This shift toward more varus-oriented alignment with increasing OA severity has since been confirmed in multiple cohort studies, including a large-scale analysis of CPAK distributions in Asian populations. These studies consistently report that type 1 is the most prevalent phenotype in patients with medial compartment OA.5,9,11,16,20,24,25
Our cohort of patients with MMPRT demonstrated similar alignment characteristics, with a mean aHKA of −2°± 3.4°, a mean JLO of 173.9°± 4.2°, and a KL grade of ≥2 changes in >90% of affected knees. These findings suggest a predominance of constitutional or acquired varus alignment combined with apex distal JLO, which may contribute to abnormal load distribution across the medial compartment. This altered biomechanics is a recognized mechanical risk factor for both meniscal root tears and early medial compartment degeneration. Studies from India, China, the Republic of Korea, Japan, and Malaysia have all reported high proportions of type 1 and type 2 phenotypes among patients with OA, especially those with varus alignment and those with apex distal JLO.5,9,11,16,20,24,25 These consistent patterns across diverse populations reinforce the external validity of the CPAK classification in characterizing coronal plane alignment relevant to MMPRT, and support the notion that apex distal JLO may play a meaningful role in the pathogenesis of MMPRTs.
Regarding measurement reproducibility, our interrater ICCs for LDFA (0.91) and MPTA (0.93), along with substantial intra-rater κ for CPAK classification (0.80), are consistent with previously reported10,12,23 reliability ranges for radiographic alignment assessments, in which ICC values typically range from 0.84 to 0.99 and κ coefficients between 0.70 and 0.82. Collectively, these results support that CPAK classification has both external validity and robust reproducibility in evaluating coronal alignment relevant to MMPRT.
This study has several limitations. First, the relatively small sample size, although adequately powered for prevalence estimation, may have limited the ability to detect differences in subgroup analyses. Second, radiographic measurements relied on full-length standing radiographs, which may be affected by patient positioning, limb rotation, and image quality, potentially introducing measurement variability despite good intra- and interrater reliability. Third, the lack of racial and ethnic diversity, with all participants being Thai, restricts the generalizability of findings to other populations. Fourth, the predominance of female patients in this study, reflecting typical MMPRT demographics, may influence the observed distribution of CPAK phenotypes, considering known sex-based anatomical differences. Finally, although end-stage OA knees (KL grade 4) were excluded, moderate degenerative changes present in many patients might have impacted the accuracy of angular measurements due to structural joint alterations such as osteophytes or joint space narrowing.
Taken together, these observations support the reliability and clinical relevance of the CPAK classification in the setting of MMPRT, where coronal plane alignment JLO appears to play a meaningful role in disease manifestation and progression. Building on this, future research should explore the potential of CPAK phenotypes as prognostic markers for both nonoperative and surgical outcomes, particularly in identifying which alignment profiles may predispose patients to more rapid osteoarthritic changes or suboptimal recovery after meniscal root repair. There is also a need to investigate how CPAK classification might inform decision-making in cases where the indication for concurrent realignment procedures, such as high tibial osteotomy, remains equivocal. Further studies across broader, more diverse populations, as well as longitudinal analyses of changes in alignment over time, will be important for clarifying the role of coronal alignment in the natural history and management of MMPRT.
Conclusion
In patients with MMRT, the most common coronal plane alignment classification was type 2 (39.1%), followed by type 1 (28.7%) and type 4 (11.5%). Apex distal joint line obliquity was observed in 73.4% of cases, while varus alignment was present in 41.4%. These findings suggest that apex distal JLO may be a contributing factor in the development of MMRT.
Footnotes
Acknowledgements
The authors wish to thank the Department of Orthopedics, Faculty of Medicine, Thammasat University; the Thammasat University Hospital; and the Thai Orthopedic Society for Sports Medicine for their kind support. Also, the authors wish to thank the proofreaders and editors for their assistance.
Final revision submitted November 6, 2025; accepted December 16, 2025.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto. Due to the cross-sectional study of the hospital database, ethical approval was not sought for the present study.