
Abstract
Background:
Inferior return to sports (RTS) and functional outcomes have been reported in women after anterior cruciate ligament reconstruction (ACLR).
Purpose/Hypothesis:
The purpose was to evaluate the results of combined ACLR and anterolateral ligament reconstruction (ALLR) in young women with a high-grade pivot shift (grade ≥2). It was hypothesized that combined ACLR and ALLR would result in better RTS and rotational stability than isolated ACLR.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Two groups were retrospectively evaluated and compared. Group I (n = 39; mean age, 31.1 ± 5.7 years) underwent isolated ACLR using hamstring autografts; group C (n = 39; mean age, 30.4 ± 6.1 years) underwent combined ACLR and ALLR. Subjective outcome measures included the International Knee Documentation Committee subjective form, Lysholm, Tegner, and ACL–Return to Sport after Injury (ACL-RSI). Objective tests included a KT-2000 arthrometer stress test, a pivot-shift test, an isokinetic strength test, a Y-balance test, and a single-leg hop test. A postoperative questionnaire was administered to determine the rates and types of RTS, quality of sports performance, and reinjury and satisfaction rates. Subjective scores and clinical tests were performed at 2 years. Magnetic resonance imaging and second-look arthroscopy were conducted during the 1- and 2-year follow-ups, respectively.
Results:
The mean follow-up for groups I and C were 30.4 ± 3.9 and 29.3 ± 3.5 months, respectively (P = .194). Patients in group C had better anteroposterior (P = .001) and rotational (P = .005) stability and higher ACL-RSI scores (P = .025) than those in group I. Group C had higher composite and posteromedial reach scores on the Y-balance test than group I (P = .014 and P = .010, respectively). A total of 26 (66.7%) patients in group C and 17 (43.6%) in group I returned to their prior level of sports (P = .040). Rerupture of the ACL graft and contralateral ACL rupture occurred in 2 (5.1%) and 2 (5.1%) patients in group I, respectively, compared with no rerupture or contralateral ACL rupture in group C.
Conclusion:
Combined ACLR and ALLR in young women with a high-grade pivot shift was associated with better knee stability parameters, dynamic postural stability, and psychological readiness to RTS than isolated ACLR.
Keywords
It has been reported that women are more likely (2-8 times) to sustain anterior cruciate ligament (ACL) injuries. 17,73 Multiple risk factors of this discrepancy include increased quadriceps angle, smaller notch width, smaller ACL diameter, increased laxity in tibial rotation, a higher ratio of quadriceps-to-hamstring recruitment, and a more erect posture during landing. 17,73 After ACL reconstruction (ACLR), female patients have inferior functional outcomes, a lower rate of return to sports (RTS), and worse biomechanical tests. 40,41,69,77 To date, little has been revealed regarding the cause of this disproportionate discrepancy.
Increased rotational laxity and valgus laxity have been previously proven in female knees, which will likely affect ACLR results. 11 In a recent study, a review of a large cohort with ACLR showed that 946 women had significantly lower subjective knee scores and greater knee laxity scores and limb symmetry indexes (LSIs) in the single-leg hop test than 1726 men. 81 The anterolateral ligament (ALL) injury is often accompanied by ACL rupture, and the rate of ALL healing is low. 45,47 Since female ALL is structurally weaker than male ALL, even if some healing occurs, there may be more rotational laxity and more deterioration in knee function in women after ACL surgery. 16
Several systematic reviews have reported that performing ACLR combined with ALL reconstruction (ALLR) reduces rotational laxity and improves patient-reported outcomes compared with performing ACLR alone. 33,51,54,65 Currently accepted indications for ALLR or extra-articular procedures include high-grade pivot shift, young patients returning to pivoting activities, generalized ligamentous laxity, genu recurvatum, revision ACLR, and chronic ACL injury. 22 Nevertheless, in the existing ALLR or extra-articular procedure studies, only a few women were included, making it difficult to infer the results found for this specific population known to have relatively more residual laxity and poor outcomes.
In the present study, we aimed to compare residual instability, functional outcomes, RTS, and rupture rates in women with a high-grade pivot shift undergoing isolated ACLR or combined ACLR and ALLR. We hypothesized that women undergoing combined ACLR and ALLR would show lower residual instability and achieve better outcomes than those undergoing isolated ACLR.
Methods
Patients
This retrospective comparative study was considered exempt from ethics committee approval because the data did not include the patients’ personal information. The items evaluated in this study were the tests that all patients normally undergo in our institution. A group of consecutive female patients with ACL rupture and a high-grade pivot shift (grade ≥2) underwent combined ACLR and ALLR performed by a senior surgeon (J.G.K.) between April 2017 and June 2020. This group was compared with a historical control group of female patients with a high-grade pivot shift (≥grade 2) who underwent isolated ACLR performed by the same surgeon between January 2014 and March 2017. The enrollment period was different because combined ALLR and ACLR as a routine procedure in a high-grade pivot shift (≥grade 2) was started in our institution in 2017. This additional procedure was started after the publication of several biomechanical and clinical studies 13,14,19,20,70 that demonstrated ALLR is beneficial for the elimination of rotational laxity. The additional procedure during revision ACLR was performed in 2013 44 and its indication has been extended to a high-grade pivot shift. The inclusion criteria for this study were as follows: (1) age <45 years; (2) female sex; (3) high-grade pivot shift (≥grade 2); (4) undergoing primary unilateral ACLR; (5) undergoing follow-up magnetic resonance imaging (MRI) 12 months after primary ACLR; (6) undergoing second-look arthroscopy at a minimum of 24 months postoperatively; and (7) a minimum follow-up of 24 months. The exclusion criteria were as follows: (1) concomitant multiple ligamentous injuries; (2) previous contralateral injuries; (3) revision surgery; (4) subtotal or total meniscectomy; (5) cartilage lesions that required repair; (6) generalized laxity (≥5 points according to the modified Beighton score 9 ) or recurvatum (passive hyperextension of the knee beyond 10°); (7) increased posterior tibial slope ≥12°; and (8) malalignment. Patients who did not agree to undergo a follow-up MRI or second-look arthroscopy were excluded. Based on the selection criteria, 78 patients were included in this study. The patients were divided into 2 groups according to the surgical procedure: group I (isolated ACLR; n = 39) and group C (combined ACLR and ALLR; n = 39) (Figure 1).

Flowchart of included patients in the 2 groups. ACLR, anterior cruciate ligament reconstruction; ALLR, anterolateral ligament reconstruction.
Surgical Technique and Postoperative Rehabilitation
All patients underwent anatomic single-bundle ACLR using a hamstring autograft (the quadrupled semitendinosus tendon) with the modified transtibial method, as previously described. 43,53 Our published studies revealed that anatomic femoral tunnel placements did not vary between the modified transtibial group and the outside-in (OI) group, and the modified transtibial group had more benefits in graft maturity than the OI group. Therefore, the modified transtibial technique was used for anatomic ACLR. 43,46,53 The gracilis tendon was additionally used to create a sufficient diameter of the autograft if the diameter of the quadrupled semitendinosus tendon was <8 mm. 49 An anatomic femoral tunnel was made using the method previously developed by the senior author. 43,46 The femoral graft was dual-fixed using XO Button (ConMed Linvatec) and Bio-Cross Pin (RIGIDFIX; DePuy Mitek). The tibial graft was also dual-fixed using a bio-interference screw (Matryx; ConMed Linvatec) and an additional cortical screw or staple. ALLR was performed in group C using a tibialis anterior tendon allograft (fresh frozen) as described earlier. 71 The femoral tunnel was made using a 6-mm drill at the femoral origin of the ALL, which was placed just proximal and posterior to the lateral epicondyle. The tibial tunnel was made of 2 tunnels approximately 1 cm below the joint line using a 4.5-mm drill. One was posterior to the Gerdy tubercle and the other anterior to the proximal tibiofibular joint. The 2 tunnels were connected in a subcortical manner using a right-angled clamp (Figure 2). After the graft was passed through the connected tibial tunnels, the 2 strands of the graft were passed underneath the iliotibial band but superficial to the lateral collateral ligament, and 2 strands were passed into the femoral tunnel. 54 Femoral fixation was performed using a 6-mm bio-interference screw (Matryx; ConMed Linvatec) with the knee at 20° to 30° and neutral rotation.

(A) The tibial tunnel is made of 2 tunnels. One is posterior to the Gerdy tubercle and the other is anterior to the fibular head. (B) The 2 tunnels are connected subcortically using a right-angled clamp.
The rehabilitation protocols were similar in both groups. All patients were allowed to bear weight with an ACL-supporting brace (Legend; DonJoy), and gradual range of motion (ROM) exercises were immediately started if tolerated. Full ROM was achieved at 3 weeks. Progressive closed kinetic and weighted open kinetic chain exercises were introduced at 3 and 6 weeks, respectively. After home-based rehabilitation, light running and side-cutting were introduced at 3 months, and sports activities were introduced at 9 months, based on the results of the functional tests.
Clinical Assessment
Subjective and objective assessments were performed before primary ACLR, 6, 9, and 12 months after surgery, and every year afterward. When analyzing clinical data in this retrospective study, data at 2 years after the surgery were used. Therefore, the clinical follow-up periods for the 2 groups were the same.
The Lysholm score, International Knee Documentation Committee (IKDC) subjective knee score, and Tegner activity scale (TAS) were examined to assess subjective knee function. Sports activity levels were classified using the TAS (Table 1). The ACL–Return to Sport after Injury (ACL-RSI) scale was used to assess patients’ psychological readiness to RTS. A questionnaire on patient satisfaction was provided to demonstrate the value of the operative intervention. Patient satisfaction was evaluated using a 5-point scale (5 = very satisfied; 4 = somewhat satisfied; 3 = neither satisfied nor dissatisfied; 2 = somewhat dissatisfied; and 1 = very dissatisfied). 30,62
Tegner Activity Scale Classification of Sports Activity a

a The ACL–Return to Sport after Injury (ACL-RSI) scale was used to assess patients’ psychological readiness to return to sports. A questionnaire on patient satisfaction was provided to demonstrate the value of the operative intervention. Patient satisfaction was evaluated using a 5-point scale (5 = very satisfied; 4 = somewhat satisfied; 3 = neither satisfied nor dissatisfied; 2 = somewhat dissatisfied; and 1 = very dissatisfied). 30,62
The objective assessments included the KT-2000 arthrometer (MEDmetric), pivot-shift test, isokinetic muscle strength test, single-leg hop for distance test, and Y-balance test (YBT). Laxity tests (KT-2000 arthrometer and pivot-shift test) were performed under anesthesia during primary ACLR and second-look arthroscopy. These were assessed based on the consensus of the senior author (J.G.K.) and the first author (D.W.L.). All other tests were administered by a single author (S.I.C.) who was blinded to the patient’s information.
Isokinetic muscle strength was measured using a Biodex System III dynamometer (Biodex Medical Systems) at an angular velocity of 60 deg/s. The peak torque (maximum value of 4 repetitions) in extension and flexion was measured for the involved and uninvolved knee, and the side-to-side deficits in extensor and flexor strength (%) were calculated. The single-leg hop for the distance test was performed as described previously and recorded as an LSI. 61 The YBT for dynamic postural stability was evaluated using the Y-Balance Test Kit (Functional Movement Systems). The test was performed 3 times in each of 3 directions (anterior, posteromedial, and posterolateral), and the maximum reach distance in each direction was recorded. These distances were then summed to yield a composite reach distance, which was normalized to leg length using the following calculation: [(anterior + posteromedial + posterolateral) / (3 × leg length)] × 100. All YBT scores were recorded as LSIs.
MRI Evaluation
MRIs were taken 1 year after the surgery. All MRI scans were obtained using a 3.0-T system (Signa HD; GE Healthcare). Image analysis was performed using a picture archiving and communication system (PACS) workstation (Centricity RA 1000; GE Healthcare). The signal/noise quotient (SNQ) of the ACL graft was measured at 3 intra-articular graft sites (femoral one-third, middle, and tibial one-third) on the oblique coronal plane to evaluate graft maturation, and the SNQ of the graft was calculated by averaging the SNQ value of the 3 sites. 3,6,75 To adjust the signal intensity of the ACL graft at each MRI, the SNQ was calculated with a region-of-interest method using a 3-mm diameter circle with the following formula: SNQ = (signal of ACL graft – signal of the quadriceps tendon) / signal of background. 3,6,56 The signal intensity of the quadriceps and the background located 25 mm medially to the medial tibial plateau was used as a reference value. The analysis was performed using the PACS workstation; all measurements were performed twice (4 weeks apart) by the same radiologist who was blinded to the patient surgery information; and mean values were used.
Second-Look Arthroscopy
Second-look arthroscopy and hardware removal were performed 24 months after surgery, as in published studies. 4,12,18,21,24,34,36 –38,52,58 Second-look arthroscopy and hardware removal were routinely recommended, 36,46,48,50 and the risks and benefits of second-look arthroscopy were explained to all patients. All patients included in the present study volunteered to evaluate graft status, including graft tension and synovial coverage. They also desired to have their tibial hardware removed. Graft tension and synovial coverage of the graft were assessed with knee extension and flexion using a probe based on the consensus of 2 experienced orthopaedic surgeons (D.W.L. and J.G.K.). Graft tension was graded as good (taut, probing <2 mm), fair (slightly lax, probing 2-5 mm), or poor (lax, probing >5 mm). 5,34,39,78 Synovial coverage was classified 2,24,60 as >75%, 50% to 75%, 25% to 50%, and <25%. Good synovial coverage was defined as covering ≥50%.
Statistical Analysis
Statistical analysis was performed using the SPSS software (IBM SPSS Statistics 21; IBM Corp). The independent t test or the Mann-Whitney U test was used to compare parametric variables such as age, body mass index, duration, the side-to-side difference on the KT-2000 arthrometer, and clinical scores and nonparametric variables such as the TAS and the pivot-shift test between the 2 groups, respectively. The chi-square test or the Fisher exact test was used to compare categorical variables. Statistical significance was set at P < .05. Intraobserver reliability was assessed using the intraclass correlation coefficient (ICC), with values interpreted as excellent (>0.9), good (0.75-0.9), moderate (0.5-0.75), or poor (<0.5). 42 Multivariate logistic regression was performed to identify factors associated with better ACL-RSI scores (>57 points) and any variables that were significantly different between the 2 groups. The results of the regression analysis were presented as odds ratios (ORs) and 95% confidence intervals.
To detect a difference of 10 points in the IKDC score between the 2 groups with a significance level of .05 and a power of 80%, the required sample size was determined a priori to be 36 patients per group according to a previous study. 48
Results
A comparison of the preoperative demographic and clinical characteristics between the study groups indicated no significant differences (Table 2). Medial meniscal repairs were performed for 6 (15.4%) and 7 (17.9%) patients in groups I and C, and lateral meniscal repairs were performed for 8 (20.5%) and 8 (20.5%) patients in groups I and C, respectively.
Demographic Data and Clinical Characteristics of the Study Groups a

a Data are reported as mean ± SD unless otherwise indicated. BMI, body mass index; IKDC, International Knee Documentation Committee; SSD, side-to-side difference; TAS, Tegner activity scale.
Comparative data regarding subjective assessments at the final follow-up are shown in Table 2. Although there were no significant between-group differences in the Lysholm score, IKDC subjective score, or TAS, the means of the data favored group C. All patients were cleared to return to any sports; however, the rate of return to a prior level of sports activity was significantly higher in group C (P = .040). In group I, a preinjury-to-postoperative shift was found from high-activity sports to medium- and low-activity sports and this trend was more pronounced than in group C. All patients in group C returned to medium- or high-activity sports (Figure 3).

(A) Preinjury level of sports activity of the 2 groups. (B) Postoperative level of sports activity of the 2 groups. Low, TAS 1-3; medium, TAS 4-6; high, TAS 7-10. TAS, Tegner activity scale.
Group C showed better ACL-RSI scale scores (P = .025), anteroposterior stability as evaluated by KT-2000 arthrometry (P = .001), and rotational stability as assessed by the pivot-shift test (P = .005) (Table 3). In group I, 15% of patients showed a high-grade pivot shift (≥grade 2) compared with none in group C postoperatively. Regarding dynamic postural stability during the YBT, group C showed higher composite and posteromedial reach scores than group I (P = .014 and .010, respectively) (Table 4). Regarding patient satisfaction, 3 patients (7.7%) in group I and no patients in Group C reported being somewhat dissatisfied or very dissatisfied with the outcome of the surgery (P = .240) (Table 5).
Comparison of Clinical Outcomes at 2 Years After Surgery Between the 2 Groups a

a Data are reported as mean ± SD unless otherwise indicated. Bold P values indicate statistically significant differences between groups (P < .05). ACL-RSI, Anterior Cruciate Ligament Return to Sport After Injury; IKDC, International Knee Documentation Committee; LSI, limb symmetry index; SSD, side-to-side difference; TAS, Tegner activity scale.
Comparison of the Y-Balance Test Between the 2 Groups a

a Data are reported as mean ± SD unless otherwise indicated. LSI, limb symmetry index. Bold P values indicate P < .05.
Patient Satisfaction at the Last Follow-up

The results of MRI and second-look arthroscopy at the 2-year follow-up are summarized in Table 6. All ICC values for intraobserver reliabilities were >0.8 (good) in radiologic measurements. The SNQ of the proximal one-third of the intra-articular graft was higher in group I than in group C (P = .023) (Figure 4). There were no significant differences in graft tension and synovial coverage during second-look arthroscopy between the 2 groups. The rate of good coverage (≥50%) was 82.1% for group C and 64.1% for group I (P = .074). None of the patients had newly appeared cartilage lesions or meniscal tears. Medial meniscal retears were found in 1 patient in group I and 1 patient in group C, and they underwent partial meniscectomy.
Results of MRI and Second-Look Arthroscopy a

a Data are presented as mean ± SD, n, or n (%). The bold P value indicates a statistically significant difference between groups (P < .05). MRI, magnetic resonance imaging; SNQ, signal/noise quotient.

The SNQ of the proximal one-third of the intra-articular graft (black arrow) was higher in (A) isolated ACLR compared with (B and C) ACLR combined with ALLR (black arrowheads). ACLR, anterior cruciate ligament reconstruction; ALLR, anterolateral ligament reconstruction; SNQ, signal/noise quotient.
Rerupture of the ACL graft and contralateral ACL rupture occurred in 2 (5.1%) patients and 2 (5.1%) patients in group I, respectively. Two patients were reinjured during medium or high levels of sports activity at 17.5 ± 2.4 months after the surgery. They did not undergo revision ACLR because the grade of laxity was <2. Two contralateral ACL ruptures occurred during medium or high levels of sports activity >2 years after the surgery. No rerupture or contralateral ACL rupture occurred in group C. Regarding complications, no patients showed loss of ROM. However, 3 patients in group C experienced anterolateral discomfort in the first 3 months after surgery. After 6 months, no further discomfort was reported. There was no fracture around proximal tibial tunnels for ALL grafts.
Multivariate regression analyses indicated that variables significantly associated with an ACL-RSI of >57 points were combined ACLR and ALLR (compared with isolated ACLR), lower postoperative pivot shift, higher preinjury TAS, and higher posteromedial reach score in YBT (Table 7).
Multivariate Regression Analysis of Factors Associated With Better (>57 Points) ACL-RSI a
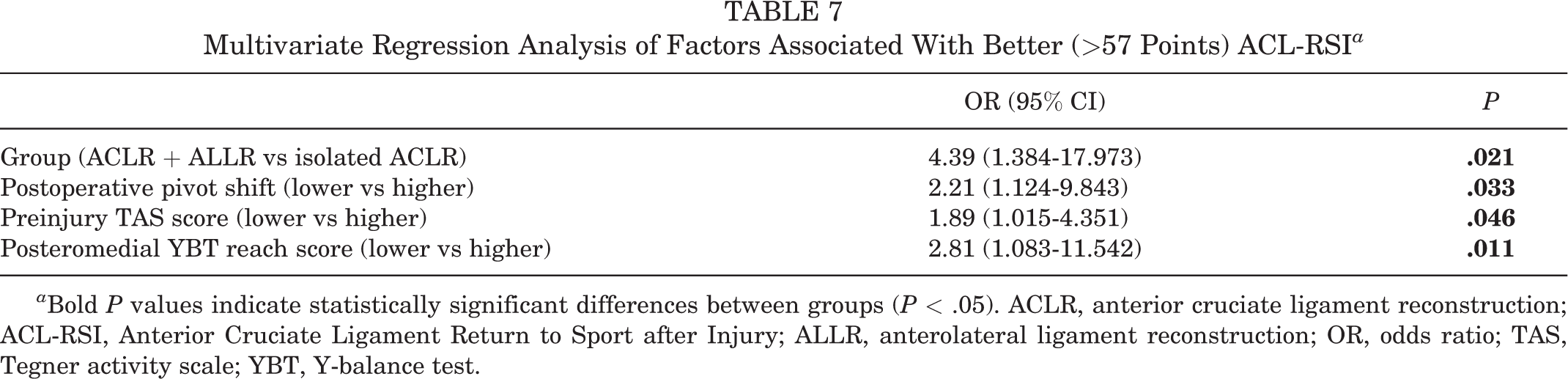
a Bold P values indicate statistically significant differences between groups (P < .05). ACLR, anterior cruciate ligament reconstruction; ACL-RSI, Anterior Cruciate Ligament Return to Sport after Injury; ALLR, anterolateral ligament reconstruction; OR, odds ratio; TAS, Tegner activity scale; YBT, Y-balance test.
Discussion
The main finding of this study is that female patients with a preoperative high-grade pivot shift who underwent combined ACLR and ALLR showed better anteroposterior, rotational, and dynamic postural stabilities and a reduced likelihood of graft rerupture compared with isolated ACLR. Moreover, psychological readiness to RTS was higher in the combined ACLR and ALLR group, although there were no significant differences in IKDC subjective score, Lysholm score, and TAS between the 2 groups. Thus, female patients with high-grade pivot shift may benefit from extra-articular augmentation.
Women have been shown to have inferior subjective knee scores, greater laxity, inferior RTS, and worse functional tests than men after ACLR. 17 Data from the Swedish knee ligament registry reported that women showed statistically worse 1-year postoperative scores (Knee injury and Osteoarthritis Outcome Score [KOOS] Pain and KOOS Sport/Recreation subscales) and 2-year postoperative scores (KOOS Sport/Recreation and KOOS Quality of Life subscales). 1 Other data from the Netherlands ACLR registry documented that men showed slightly better self-reported knee questionnaires 1 year after ACLR. 77 A systematic review and meta-analysis based on 135 publications revealed that women showed a statistically significant increase in pooled anterior laxity (standardized mean difference, 0.24 [95% CI, 0.11-0.37]) and a statistically significant inferior outcome in the incidence of not returning to sports (relative risk, 1.12 [95% CI, 1.04-1.21]). 74 Hamrin Senorski et al 26 also reported that women (51% of 272 patients) showed a statistically significant lower RTS rate 1 year after ACLR (OR, 2.58 [95% CI, 1.43-4.65]). Kuenze et al 41 demonstrated that women displayed significantly higher total Landing Error Scoring System scores, with a statistically significant difference, and were more likely to land with less trunk flexion (OR, 4.94), more medial knee position at initial contact (OR, 6.01), greater medial knee displacement (OR, 7.88), and less total joint displacement (1 error: OR, 2.10; 2 errors: OR, 3.71). Based on these findings, we suggest different treatment strategies for women.
In this context, a strategy to further secure postoperative knee stability is needed in cases of preoperative high-grade pivot shift in female patients. Several authors have reported that preoperative high-grade pivot shift is a significant risk factor for residual pivot shift after ACLR. 31,32,79 Residual anterolateral rotatory instability causes limitations in returning to the preinjury level of sports activities and performance. 66,76 Furthermore, rotational instability could increase the risk of meniscal injury and osteoarthritis. 29,57 Therefore, resolving anterolateral rotatory instability may be critical in improving knee stability and clinical outcomes after ACLR. Recently, many authors have revealed that ALL acts synergistically on the ACL as a secondary rotatory stabilizer, and combined ACLR and ALLR have advantages in terms of stability of internal rotation and anterior translation, subjective clinical scores, RTS, and rerupture rate. 8,16,51,82 Our results are consistent with those of previous studies. Group C showed favorable results in the anteroposterior laxity and pivot-shift tests, with statistical significance. Helito et al 27 reported that the ACLR combined with ALLR group (n = 33) showed significantly better anteroposterior laxity tested by the KT-1000 arthrometer than the isolated ACLR group (n = 68) in chronic ACL injuries (1 mm vs 2 mm; P = .048). Helito et al 28 also proved that the ACLR combined with ALLR group (n = 30) showed better anteroposterior laxity assessed by the KT-1000 arthrometer than the isolated ACLR group (n = 60) in ligamentous hyperlaxity (1.5 ± 1.1 vs 2.3 ± 1.4 mm; P = .02). A pivot-shift phenomenon includes anterior tibial translation and tibial internal rotation, and additional extra-articular procedures can reduce both anterior translation and tibial internal rotation. 80 However, laxity cannot be measured more accurately than 1 mm, and even then, we have to allow for a measurement error of ±1 mm. To prove this, it seems necessary to conduct a prospective study with large sample sizes. In our study, there was no high-grade pivot shift after combined ACLR and ALLR, while 15.4% of the 39 patients showed a high-grade pivot shift after isolated ACLR. A recent systematic review and meta-analysis 8 demonstrated that combined ACLR and ALLR reduced the rate of residual pivot shift by 66% compared with isolated ACLR (P < .01). In a dynamic postural stability assessment during the YBT to evaluate the control of the trunk and lower limb, group C showed statistically better results in the composite and posteromedial reach scores than group I. The dynamic postural stability test can reflect the actual sports activities in a closed kinetic chain system better than knee laxity tests (anteroposterior laxity test and pivot-shift test) performed in an open kinetic chain system. 10,55 Kim et al 35 revealed that YBT scores had significant correlations with functional performance tests (single-leg hop test and single-leg vertical jump test) after ACLR. Although some studies reported no significant relationship between composite score and future injury, others revealed significant relationships between posteromedial reach asymmetry and future injury risk. 64 Gonell et al 23 showed that football players with a difference of ≥4 cm between the lower limbs in the posteromedial reach had almost a 4-fold greater risk of noncontact injury in the lower extremity. The knee extensor, hip abductor, and hip extensor moments in the sagittal and frontal planes affect the posteromedial reach during the YBT. 59 Further studies are needed to determine whether improved knee laxities (anteroposterior and rotational) by additional extra-articular augmentation can improve dynamic postural stability. Combined ACLR and ALLR may affect ACL reinjury. Graft rerupture and contralateral ACL rupture were not found in group C, while 2 (5.1%) patients and 2 (5.1%) patients showed graft rerupture and contralateral ACL rupture in group I. A recent systematic review with meta-analysis 8 demonstrated that combined ACLR and ALLR reduced the rate of graft rupture by 66% compared with isolated ACLR (P < .01). Sonnery-Cottet et al 72 reported that the rate of graft failure with additional ALLR (221 patients) was at least 2.5 times lower than with other isolated ACLRs (281 patients).
We suggest that physical and functional benefits from additional ALLR affect psychological readiness to RTS and the rate of return to a prior level of sports activity, although there were no significant differences in some subjective knee scores between the 2 groups. We assume that psychological readiness was more closely related to ligament laxity than the IKDC or Lysholm scores in this study. Lower postoperative pivot shift, higher preinjury TAS, and higher posteromedial reach score in the YBT were significantly associated with an ACL-RSI of >57 points, including combined ACLR and ALLR (compared with isolated ACLR). In the present study, group C showed a higher ACL-RSI score than group I (73.2 ± 15.6 vs 64.8 ± 16.8, P = .025). The ACL-RSI scale was developed to assess psychological factors as an indicator of readiness to RTS after ACL injury or ACLR and validated by standardized statistical methods. 25 It contains 3 subdomains: confidence in performance, emotions, and risk appraisal. Previous studies reported that an ACL-RSI score <56 points indicated an increased risk of not returning to a prior level of sports activity. 7,63 In our study, group C showed a higher ACL-RSI scale than isolated ACLR presented in previous studies. Lee et al 48 showed that ACL-RSI scales in adults and adolescents were 67.5 ± 7.2 and 63.7 ± 8.1 at a minimum 2-year follow-up. They suggested that the ACL-RSI scale of adolescents was significantly lower than that of adults because adolescents had a higher rate of poor ALL healing after ACLR. A French prospective ACLR cohort study (FAST) demonstrated that the ACL-RSI scale was 65.2 ± 25.3 at 2 years, and 58.4% of 681 patients could return to their prior level of sports activity at a 2-year follow-up. 67 The FAST suggested that the optimal ACL-RSI scale cutoff to return to the same sports at a 2-year follow-up was ≥65 points. In our study, all patients could participate in medium-level sports during the preinjury period. The medium-level sports mostly include pivoting sports. After the surgery, all patients could return to any sports activity; however, the rate of return to a prior level of sports activity was higher in group C than in group I (66.7% vs 43.6%), with a significant difference. Regarding activity level change after ACLR, group I showed a more pronounced shift from high to medium and low sports activity levels than group C. We assume that the additional ALLR has beneficial effects on sports activity or hinders function. A recent review 68 demonstrated that additional ALLR is associated with a significantly increased likelihood of return to the prior level of sports activity after primary ACLR (OR, 1.938 [95% CI, 1.174-3.224]). Lee et al 44 reported that revision ACLR combined with ALLR showed a higher rate of return to the prior level of sports activity than isolated revision ACLR (57.1% vs 25.6%; P = .008). The positive effect on the subsequent RTS may be related to patient satisfaction. In the present study, 7.7% of patients in group I reported being somewhat dissatisfied or very dissatisfied with the outcome of the surgery; however, none of the patients in group C reported being somewhat dissatisfied or very dissatisfied.
Extra-articular augmentation, which reduces anteroposterior laxity and anterolateral rotatory laxity, is important in protecting the ACL graft during the healing and remodeling phases. Engebretsen et al 20 revealed that extra-articular augmentation significantly decreased the strain on an ACL graft by a mean of 43%. We assume that these “backups” of additional ALLR could affect graft healing. In the present study, the SNQ of the proximal one-third of the intra-articular graft was higher in group I than in group C (P = .023), as measured by MRIs at a minimum 2-year follow-up. Based on this finding, the protective effect of additional ALLR appears appropriate in patients who are expected to have poor outcomes after primary ACLR. In this study, we did not analyze the SNQ of ALL from MRI. We suggest that MRI cannot accurately distinguish between ligamentous laxity and signal change of ALL. We think that it is reasonable to evaluate the function of extra-articular structure to the degree of laxity through physical examination rather than to measure it with the SNQ of MRI.
Some authors are concerned about conducting extra-articular augmentation because of the presumed high risk of complications. In the present study, there was no sustained pain, bioabsorbable screw protrusion, stiffness, or swelling at the minimum 2-year follow-up. A matched-pair analysis from the Scientific ACL Network International Study Group reported that additional ALLR did not delay functional recovery and did not have disadvantages in neuromuscular control, agility, or psychological readiness to RTS at 6 months postoperatively. 15
Limitations
The present study had some limitations. First, the analysis had a retrospective design, despite prospective data collection. A randomized controlled trial is warranted to confirm our results. Isolated ACLR and combined ACLR and ALLR were performed between January 2014 and March 2017 and between April 2017 and June 2020, respectively, nonrandomly. The different treatment periods in both groups could be a source of bias. A historical control was used because extra-articular augmentation started in 2017 and became the standard procedure for women with a preoperative high-grade pivot shift. Nevertheless, the preoperative demographic data after retrospective analysis demonstrated that the groups did not differ significantly. All surgeries were performed in the same institution by the same experienced surgeon. Second, the minimum 2-year follow-up period was not long enough to identify the complications of lateral compartment overstraining and osteoarthritis. Therefore, long-term studies are required. Third, a senior author (J.G.K.) who was not blinded at the follow-up examination with over a decade of experience conducted the pivot-shift test manually. In a state where quantitative analysis is difficult, consistent evaluation by experienced examiners is important. Therefore, developing a precise instrument to perform the pivot-shift test quantitatively is necessary. Finally, our results may not be generalizable for other grafts/techniques.
Conclusion
Combined ACLR and ALLR in young women with a high-grade pivot shift was associated with better knee stability parameters, dynamic postural stability, and psychological readiness to RTS than isolated ACLR. Combined ACLR and ALLR did not result in extra-articular procedure-related complications.
Footnotes
Final revision submitted February 25, 2023; accepted March 10, 2023.
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was waived by Konkuk University Medical Center (no. KUMC 2021-09-036).