
Abstract
Background:
The Segond fracture is an avulsion-type fracture located on the anterolateral aspect of the tibia associated with a ligament recently termed the anterolateral ligament. This injury has been described as pathognomonic for an anterior cruciate ligament (ACL) tear and is associated with a higher grade pivot shift.
Purpose:
To present and report 2-year clinical outcomes of a surgical technique for acute ACL reconstruction with fixation of a concomitant Segond fracture.
Study Design:
Case series; Level of evidence, 4.
Methods:
A retrospective chart review was performed of patients who underwent acute reconstruction for a complete ACL tear with concomitant Segond fracture fixation between January 2010 and December 2014; surgery was performed by a single surgeon. Patients underwent direct Segond fracture repair by either suture alone, suture anchor, or cannulated screw fixation based on the size of the lesion, followed by a 2-incision hamstring autograft intra-articular reconstruction. Pre- and postoperative KT-1000 arthrometer assessment, Lachman test, and pivot-shift test were performed, and patients were administered validated subjective outcome surveys.
Results:
Twelve patients met inclusion criteria for this review. The measured pre- and postoperative objective and subjective scores were significantly improved in all patients. Side-to-side anterior laxity was significantly improved in all patients based on Lachman and KT-1000 arthrometer testing. A significant pivot shift demonstrated preoperatively (3+, n = 11 [92%]; 2+, n = 1 [8%]) was corrected after fixation, except in 1 patient (8%), who maintained a 1+ pivot shift. Lysholm, Tegner, and International Knee Documentation Committee subjective and objective scores were significantly improved. At a minimum 2-year follow-up, no patients reported rerupture, and only 1 patient (8%) underwent a subsequent procedure (a meniscectomy). No major or minor complications were reported, and all patients returned to their previous activity levels at a mean of 6 months postoperatively.
Conclusion:
Direct repair of the Segond fracture and plication of the anterolateral capsule in patients with an ACL rupture and a high-grade pivot shift demonstrate good clinical outcomes, restoration of rotational stability, and maintenance of knee range of motion at 2 years postoperatively, with no major complications.
Keywords
In 1879, the French surgeon Paul Segond 28 conducted a series of cadaveric studies and reported that a relatively constant avulsion-type fracture occurred on the anterolateral aspect of the tibial plateau with forced internal rotation of the knee. This injury therefore became known as the Segond fracture. With the invention of radiography, investigators found a correlation between anterior cruciate ligament (ACL) rupture and the presence of a Segond fracture 10,12,35 ; an ACL rupture was almost always present if a Segond fracture was seen on radiograph. 6,10 This association can be related to the internal rotation torsion on the knee seen frequently in noncontact ACL tear mechanisms.
Segond 28 further described in his report that “a pearly, resistant, fibrous band” was located in the anatomic position of this avulsion fracture, which became tight with internal rotation of the knee. In the more than 100 years since Segond’s report, this anatomic structure has been described in various anatomic studies and given different names: middle one-third of the lateral capsule ligament, 13 anterolateral femorotibial ligament, 24 anterolateral ligament (ALL), 33 and anterolateral complex (ALC). 8 A descriptive study performed by Claes et al 5 in 2013 identified this ligament (using the term anterolateral ligament) in 40 of 41 cadaveric knees (97%). Subsequent biomechanical studies 23,27 have suggested that the ALL contributes to the control of internal rotation and that injury to this ligament may worsen the degree of the pivot-shift phenomenon seen after an ACL rupture.
Recently, Ferretti et al 8 performed a descriptive clinical study on patterns of injury and prevalence of ALC injuries during an acute ACL reconstruction. The investigators found that while Segond fractures appeared in about 10% of cases, a soft tissue, intraligamentous injury of the ALC and concomitant anterolateral capsule damage were found in up to 90% of cases. As these structures appear to affect the pivot-shift phenomenon, the stability of the anterolateral aspect of the knee should be assessed and adequately managed for a potentially high-grade pivot shift, which may lead to subsequent instability episodes after intra-articular reconstruction alone. The purpose of the present study was to present our surgical technique for acute ACL reconstruction with fixation of a concomitant Segond fracture and to report minimum 2-year clinical outcomes in a series of patients who underwent this procedure.
Methods
We reviewed the charts of all patients who underwent acute reconstruction for a magnetic resonance imaging (MRI)–confirmed complete ACL tear between January 2010 and December 2014; all procedures were performed by the senior surgeon (A.F.). Patients with a Segond fracture, detected on standard anteroposterior (AP) radiographs, and who were participating in sports at a competitive level (Tegner level ≥6) were included. Additional inclusion criteria were a preoperative examination under anesthesia demonstrating a positive Lachman test and the presence of a pivot shift. Patients with meniscal tears and/or cartilage damage were included in the study.
Patients were excluded if they had multiligamentous injuries as detected by MRI and/or clinical examination (varus or valgus stress, recurvatum, and posterior drawer test), age older than 40 years, body mass index greater than 30 kg/m2, or previous knee trauma or surgery.
Ethics approval was received for this study.
Preoperative Patient Assessment
All patients were evaluated preoperatively by the senior surgeon. Clinical assessment of knee ligament integrity included the Lachman test, pivot shift, and varus-valgus maneuvers. The Lachman test was graded as negative or 0 (–1 to 2 mm; symmetric anteroposterior translation with a firm end point), 1+ (3- to 5-mm increased anteroposterior translation compared with contralateral side), and 2+ (6- to 10-mm increased anteroposterior translation compared with contralateral side) and included the modification for the presence of a firm end point. The pivot-shift test was graded 0 (negative), 1+ (glide), 2+ (clunk), and 3+ (gross subluxation). The KT-1000 arthrometer (Medmetric) was used to objectively assess the quantitative anterior translation of the knees bilaterally.
Imaging
Standardized radiographs (AP and lateral views) (Figure 1) were performed to evaluate osseous pathologic changes. Adequate AP radiographs must be performed to evaluate for the presence of a Segond fracture, located on the lateral aspect of the tibial plateau in this view. MRI studies (Figure 2) were done to evaluate the menisci and cartilage for concomitant lesions that would need to be addressed intraoperatively.
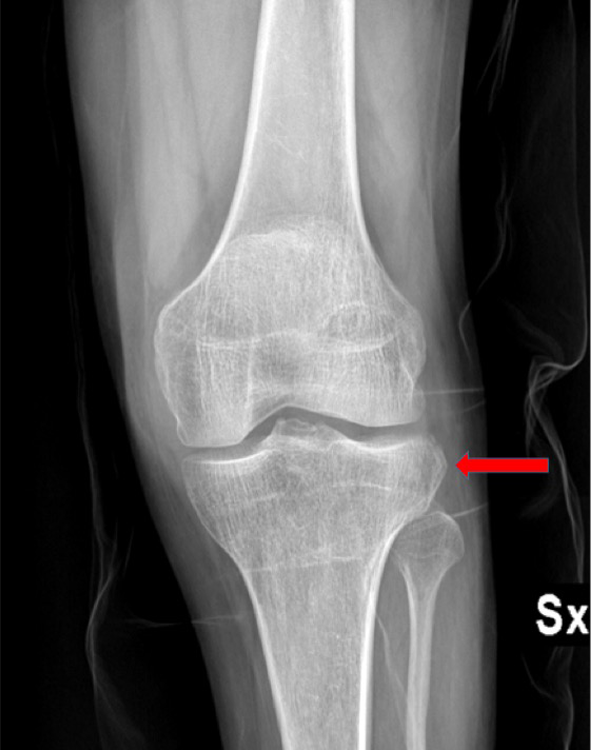
Segond fracture located on the lateral aspect of the tibia as seen on anteroposterior radiograph in a patient with an anterior cruciate ligament rupture.

Segond fracture located on the anterolateral aspect of the tibia as demonstrated on coronal magnetic resonance image of a patient with an anterior cruciate ligament rupture.
Outcome Scores
Validated patient outcome scores were administered preoperatively and at final follow-up. The Tegner activity score 30 was used to assess current patient activity level, and the Lysholm score 30 was used to evaluate subjective functional status. The International Knee Documentation Committee (IKDC) evaluation system was included to assess the patients’ subjective evaluation of knee function, such as symptoms and activity level, as well as objective measures such as knee laxity and range of motion (ROM) examinations, which were performed by the senior surgeon. The results of the IKDC objective score were graded as A (normal), B (nearly normal), C (abnormal), or D (severely abnormal).
Surgical Technique
All surgeries were performed by the senior surgeon. First, the lateral compartment was addressed. The patient was placed in a supine position on the operating table, allowing for complete mobilization of the lower leg throughout the procedure. A thigh tourniquet was placed and inflated to 350 mm Hg before the incision was made. With the patient’s knee flexed to 90°, the surgeon initiated a hockey-stick incision distally at the Gerdy tubercle and extended the incision proximally to just inferior to the lateral femoral epicondyle, 10 to 12 cm in length. The fascia lata was incised longitudinally along its fibers and gently elevated to enable visualization of the lateral compartment. The Segond fracture was directly repaired in all patients by use of a technique based on the dimension of the bone fragment (direct suture, anchors, or screw fixation) (Figures 3 and 4).

Postoperative anteroposterior radiograph of a patient who underwent concomitant anterior cruciate ligament reconstruction and Segond fracture fixation with two 5-mm suture anchors. Intra-articular anterior cruciate ligament reconstruction was performed by use of a hamstring autograft and was fixed with the Swing Bridge device on the femur and the Evolgate device on the tibia.

Postoperative anteroposterior radiograph of a patient who underwent concomitant anterior cruciate ligament reconstruction and fixation of a large (>2 cm2) Segond fracture with cannulated cancellous screw fixation. Intra-articular anterior cruciate ligament reconstruction was performed by use of a hamstring autograft and was fixed with the Swing Bridge device on the femur and the Evolgate device on the tibia.
Direct suture or anchor fixation (surgeon discretion) was used when the bone fragment was 2 cm2 or smaller. The surgeon placed 3 parallel square knot stiches using No. 2 Vicryl suture or a 5-mm suture anchor (Corkscrew; Arthrex) with mattress suture fixation while the patient’s knee was in 90° of flexion and neutral rotation. Fragments larger than 2 cm2 were secured by cannulated screws. Plication of the capsule with absorbable suture was performed concomitantly when extensive damage or stretching of the capsule was observed, as described previously. 8 The knee was then tested gently for ROM and pivot shift. The repair was considered successful if full ROM and absence of the pivot shift were demonstrated.
An arthroscopically assisted anatomic single-bundle ACL reconstruction was performed as described previously. 7,18 A 2-incision technique was used to reconstruct the ACL with a doubled semitendinosus and gracilis tendon autograft. The graft was fixed to the femur by use of the Swing Bridge device (Citieffe) and to the tibia with the Evolgate device (Citieffe). The lateral incision and arthroscopic portals were closed at the end of the surgical procedure after the tourniquet was released.
Postoperative Rehabilitation
The involved knee was placed in a full-extension brace for 4 weeks postoperatively. Patients were allowed immediate weightbearing as tolerated in the brace with crutches. Progressive ROM exercises were initiated after the first postoperative day, and daily isometric and isotonic exercises were prescribed. At 4 weeks postoperatively, full weightbearing without crutches or the brace was permitted. At 8 weeks postoperatively, a muscle-strengthening program was initiated with open kinetic chain exercises. At 4 months postoperatively, a month-long gradual return to noncontact athletic and sport-specific training was encouraged, including running and cutting. Return to full sport activities was then allowed at 5 months postoperatively, based on trainer evaluation and determination of readiness for return to sport.
Statistical Analysis
Descriptive statistics used mean and standard deviation, including the range of values. Continuous variables were analyzed with the Student t test. The alpha level for all analyses was set at .05. All statistical analysis was performed with SPSS Statistics version 9.0 (IBM Corp). This study was approved by the University of Rome Sapienza’s institutional review board.
Results
A total of 12 patients were included in this study (10 male, 2 female). Demographics of these patients are shown in Table 1.
Demographic data (N = 12 Patients)
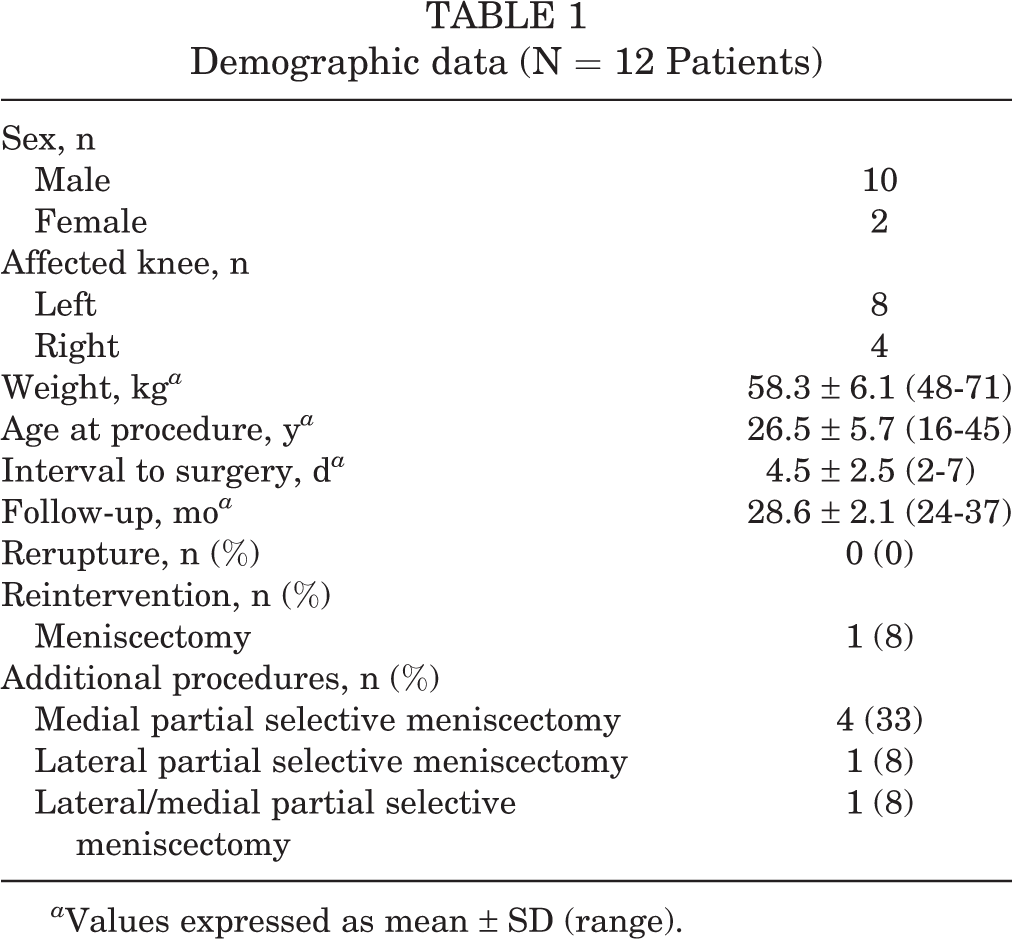
a Values expressed as mean ± SD (range).
Mean ± SD age at the time of surgery was 26.5 ± 5.7 years (range, 16-45 years). The patients were observed for a mean 28.6 ± 2.1 months (range, 24-37 months). During this follow-up period, no patients experienced graft rerupture, but 1 patient underwent a second operation for a meniscectomy.
A bony avulsion off the anterolateral tibia was detected in all patients in addition to capsular damage. Four patients had a concomitant massive disruption of ALC, extending to the posterolateral capsule. Repair of the Segond fracture was performed in 7 patients by use of periosteal stitches, in 4 patients with suture anchors, and in 1 patient, due to a larger fragment, with a cancellous screw (Figure 4). In all patients, due to the severity of the capsular damage, the capsule was retensioned by plication. Six patients (50%) had an unstable radial or flap meniscal tear at the time of surgery that was not amenable to repair; all 6 patients underwent partial selective meniscectomy. There were no bucket-handle or ramp lesions in this cohort. Correction of the pivot shift with no limitation to knee ROM, which constituted a successful repair, was observed in all patients.
Pre- and postoperative outcome data are shown in Table 2.
Pre- and Postoperative Clinical and Outcome Data a

a IKDC, International Knee Documentation Committee.
b Values expressed as mean ± SD (range).
c Values expressed as mean ± SD.
The Lachman test was positive (2+) in all patients preoperatively but was negative (0) in all patients postoperatively (P = .028). The pivot shift was graded as 3+ in 11 patients and 2+ in 1 patient preoperatively; however, postoperative pivot shift was negative in all except for 1 patient, who was found to have a glide (1+) (P = .032). The KT-1000 arthrometer objective testing of joint laxity also demonstrated a significant improvement in anterior knee laxity (P = .045).
No complications such as infections, malunions of the bone fragment, postoperative stiffness, or rerupture of the ACL were reported. On average, patients returned to sport after 6 months. At the latest follow-up, all patients had returned to their preoperative sports activity level.
Discussion
Although the Segond fracture has long been described as a pathognomonic radiological sign for an ACL tear, the biomechanical effect of such a fracture has not been fully elucidated. Since Segond’s initial study, 28 multiple authors have reported on the anatomic features of the lateral aspect of the knee. 13,24,33 Several authors 3,11,21 have further described the anatomic features and insertion point of the ALL on both the femoral and tibial sides. While the femoral insertion is still debated, the tibial insertion has been widely reported as located midway between the Gerdy tubercle and the fibular head, corresponding to the radiological description of the Segond fracture. 4 For this reason, we speculate that the Segond fracture is the bony equivalent of an avulsion of the ALL occurring during an ACL injury.
Since the 1970s, researchers have documented that the anterolateral structures of the knee are important restraints to internal rotation of the knee, acting in synergy with the ACL. Lesions of these structures have recently been found to have a strong correlation with the degrees of the pivot-shift phenomenon seen after an ACL tear. A Segond fracture, the bony equivalent of an ALL tear, could therefore affect the pivot shift. This clinical finding was demonstrated in the current study, as the preoperative pivot-shift evaluation under general anesthesia was graded as 3+ in all but 1 patient and was found to be 0 or 1+ after repair of the Segond fracture and capsular plication alone. Therefore, repair of the Segond fracture appears biomechanically justified.
The main finding of this study is that repair of a Segond fracture performed with a standard hamstring ACL reconstruction is a safe and successful procedure resulting in excellent recovery of knee stability and function with no major complications. Another important finding of this study is that although another skin incision is required, the procedure presented in this study does not otherwise increase morbidity. Patient postoperative course, rehabilitation, and return to sport were identical to those occurring with an isolated, standard intra-articular ACL reconstruction. Our results compare well with previous studies, 9,31 which reported that extra-articular reconstruction in addition to standard ACL reconstruction improved clinical outcomes, knee stability, and rate of recurrence.
Many authors have demonstrated that although a certain degree of persistent rotational instability remains after an isolated intra-articular ACL reconstruction, the procedure typically results in good recovery of knee stability and function. 1,2,15 –17,29 Therefore, the indication for an additional procedure, even in the most severe cases of ALC damage and the presence of a Segond fracture, remains unclear. Previous authors have considered the addition of lateral extra-articular tenodesis techniques to the standard ACL reconstruction, with the aim of improving rotational stability of the knee. 14,19 An extra-articular procedure such as this, which is performed peripheral to the center of rotation of the knee, has a better lever arm for rotational control than that provided by an intra-articular reconstruction alone. The efficacy of these procedures has been demonstrated in long-term follow-up studies 9,22 as well as in kinematic studies. 23,36 However, the procedures described in these previous studies are not based on the restoration of anatomic structures. Contemporary belief is that if an anatomic structure is torn, the goal should be to reconstruct it as close to its native characteristics as possible. This study attempted to evaluate the effect of an anatomic direct repair of the Segond fracture.
Some authors 9,20,26,32,34 have recently reported that additional extra-articular procedures are indicated in cases of high-level athletes, sport participation, younger age, revision surgery, and increased laxity, the latter of which is seen in many female athletes. In the present series, patients were selected based on level of sport participation as well as the increased severity of instability reliably demonstrated in patients with a Segond fracture. The decision to include direct repair of the Segond fracture and plication of the lateral capsule was made in order to offer the greatest chance of stability and return to sport. Return to sport occurred, on average, after 6 months, similar to the return-to-sport statistics reported after isolated intra-articular ACL reconstruction.
As a retrospective case series, this study has inherent limitations, including selection bias and the lack of a control population. Although tests such as the pivot shift and Lachman were manually performed and therefore subjective in grading, the senior surgeon performed and reported all examination findings, and these tests have been reported to have high intraobserver correlations. 20,25 Furthermore, the same senior surgeon performed all surgeries and all clinical tests to eliminate interobserver variability. Although the sample size was limited to 12 patients, a Segond fracture revealed by radiograph is relatively rare, occurring in less than 10% of ACL injuries. Future studies may include multiple sites as well as a control patient population undergoing isolated intra-articular reconstructions.
The aim of this study was to evaluate the effect of an acute direct repair of Segond fractures in patients with acute ACL tears. To our knowledge, this is the first attempt to report outcomes after this procedure. Our results confirm the importance of the Segond fracture and the ALC in controlling rotational stability of the knee and the pivot-shift phenomenon, supporting early speculation that unrecognized injury to an extra-articular structure such as the ALC may account for some cases of rotational instability after ACL reconstruction.
Conclusion
The Segond fracture can be considered the bony equivalent of an ALC rupture. This fracture is associated with severe rotational instability of the knee as demonstrated by an increased pivot-shift grade. In this study, we reported that direct repair of the Segond fracture in acute ACL surgery restores rotational stability and demonstrates good clinical results without complications after a minimum of 2 years of follow-up.
Footnotes
One or more of the authors has declared the following potential conflict of interest or source of funding: A.F., E.M., and A.D.C. are consultants for Arthrex.
Ethical approval for this study was obtained from University of Rome Sapienza, Rome, Italy.