
Abstract
Background:
Long-term studies of patients after anterior cruciate ligament (ACL) reconstruction with or without concomitant meniscal tear treatment are limited.
Purposes:
To (1) report postoperative outcomes after anatomic ACL reconstruction with a hamstring autograft, (2) investigate how concomitant treatment of meniscal injury could affect these outcomes, and (3) evaluate the association between quality of life and activity levels at a minimum 10-year follow-up.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Patients treated with a unilateral, anatomic ACL reconstruction between 2005 and 2011 were investigated. The following patient-reported outcome measures (PROMs) were reported for the overall sample as well as a subsample of patients with meniscal injury: International Knee Documentation Committee Subjective Knee Form (IKDC-SKF), Knee injury and Osteoarthritis Outcome Score (KOOS), Lysholm knee score, Tegner activity scale, 5-level EQ-5D (EQ-5D-5L), and patient satisfaction. Sex, age, body mass index (BMI), and meniscal injury treatment (meniscectomy vs meniscal repair) were examined as patient-specific risk factors regarding long-term activity and quality of life.
Results:
Overall, 106 patients, 90 men (85%) and 16 women (15%), were enrolled in the study, with a mean follow-up of 13.2 years. The ACL retear rate was 2.8%. The mean scores were 80.6 ± 16.7 (IKDC-SKF), 87.4 ± 15.0 (KOOS), 90.5 ± 11.5 (Lysholm), 5.6 ± 1.9 (Tegner), and 91.8 ± 14.5 (EQ-5D-5L). The majority (90.6%) of patients considered their knee state satisfactory during follow-up. When compared with patients who underwent meniscal repair, patients who underwent meniscectomy had statistically significantly lower scores on all PROMs except for the Tegner and EQ-5D-5L (P < .05 for all). The mean difference between the 2 groups was ≥7 points on all PROM scores. Patient sex, age, and BMI did not affect PROM scores. There was a statistically significant, strong positive correlation between quality of life and activity.
Conclusion:
Patients had few or no symptoms and considered their knee state satisfactory 13.2 years after anatomic ACL reconstruction. Patients with concomitant meniscal tears having undergone meniscal repair had improved PROMs compared with those treated with meniscectomy. Finally, participation in activities of daily living and sports was interrelated with quality of life and was not affected by patient age, sex, or BMI.
Keywords
Anterior cruciate ligament (ACL) rupture is a common sports injury, and ACL reconstruction is one of the most common orthopaedic procedures. 37 Currently, ACL reconstruction is performed mainly using autografts, since the use of allografts and synthetic grafts has shown inferior results in terms of retear rate. 5,6,16 The classic bone–patellar tendon–bone (BPTB) graft, the hamstring tendon graft, and the quadriceps graft, which have gained popularity since 2014, are currently the 3 most common options. 2 Although many studies on short-term outcomes using all types of autografts have been published, long-term studies are still lacking, especially on reconstruction using a hamstring graft, which did not become widely used until the early 2000s. 13,32 Concomitant meniscal tears are usually encountered during ACL reconstruction and should be repaired when possible because of the chondroprotective effect of the meniscus. 22 Studies comparing patients who underwent ACL reconstruction and meniscal repair with patients with ACL reconstruction and meniscectomy have shown improved outcomes for the meniscal preservation groups in both short- and long-term studies. 27,31
In a recent consensus aiming to establish a standardized approach to assessment of clinical outcomes after ACL treatment, the role of patient-reported outcome measures (PROMs) was highlighted along with the clinical examination. 41 Their use has been also recommended as an adjunct in clinical trials. 8 Their main advantage is the ability to evaluate hundreds of patients at a fraction of the time and cost that would be necessary when having patients return for face-to-face clinical evaluation. 39 During the past 2 years, the outbreak of the 2019 novel coronavirus (COVID-19) changed the practice of most physicians, including orthopaedic surgeons and sports physicians, since elective care was deferred and telemedicine became necessary. 3,24 Inevitably, long-term follow-up of patients with no life-threatening health problems would have been impossible without the PROMs.
In recent systematic reviews of studies following patients ≥10 years after ACL reconstruction, a variety of articles have been included. 9,26,33 Most studies focus on the risk for posttraumatic osteoarthritis (OA) and rerupture rates, while others compare different grafts or techniques. Among these studies, results of anatomic ACL reconstruction using the anteromedial portal and a hamstring autograft have been reported by few centers, usually with samples of ≤90 patients. 10,34,35,42 The largest sample of such patients was reported by Bourke et al 7 and included 359 patients; however, the only questionnaire used in this study was the International Knee Documentation Committee Subjective Knee Form (IKDC-SKF). None of the above studies commented on the meniscal status of these patients and how it affected the outcomes of the reconstruction, especially regarding their activity levels and quality of life.
The goals of the present study were to (1) report PROMs at a minimum 10-year follow-up after anatomic ACL reconstruction with a hamstring autograft using the anteromedial portal, (2) investigate how a concomitant meniscal injury and its management could affect these outcomes, and (3) identify the association of patient quality of life with functional activity. The primary hypothesis was that patients treated with ACL reconstruction would present satisfactory scores in PROMs, and the secondary hypotheses were that meniscal preservation would positively influence outcomes and quality of life would be positively correlated with activity levels in this group of patients.
Methods
Study Design and Patient Enrollment
This was a retrospective cohort study of a series of patients who underwent ACL reconstruction by a single surgeon (M.H.) between January 2005 and January 2011. Ethical approval for the study protocol was obtained, and the research was performed in accordance with the 2008 Declaration of Helsinki Ethical Principles for Medical Research involving Human Subjects. A written informed consent form was signed by all participants. The Strengthening the Reporting of Observational Studies in Epidemiology guidelines were used to ensure a high-quality and complete report of the research findings.
Included in the study were patients with an ACL rupture with or without a concomitant meniscal tear who underwent unilateral arthroscopic ACL reconstruction through the anteromedial portal using a hamstring autograft. Exclusion criteria were concomitant cartilage lesions, associated posteromedial or posterolateral laxity, associated ligament injury requiring surgery, associated root tears or ramp lesions, prior knee surgery, revision ACL surgery, open physes during surgery, and refusal to participate in the research project.
During this time frame, 348 patients were identified as having undergone an ACL reconstruction, and 113 met the study’s inclusion criteria and were asked to enroll in the study. However, 7 of them were not located or refused to participate, and the final sample consisted of 106 patients (Figure 1).

Flowchart of the patient inclusion process in this study. ACL, anterior cruciate ligament.
Surgical Technique
All patients underwent an anatomic ACL reconstruction using a hamstring tendon autograft. The femoral tunnel was drilled through the anteromedial portal, at the middle of the native ACL femoral footprint. The tibial tunnel was drilled outside-in, aiming at the middle of the ACL tibial footprint. The autograft used was a 4-stranded (quadruple) graft prepared by folding the semitendinosus and gracilis tendons. Femoral fixation was performed using a button, while tibial fixation was performed using a bioabsorbable interference screw. Post fixation was also performed using a bicortical screw.
Regarding meniscal tears, the decision for preservation of the meniscus or meniscectomy was made based on the location of the tear, the repairability of the tissue, and a discussion with the patient before the surgery. Meniscectomy was performed with appropriate arthroscopic scissors and a shaver. An inside-out, outside-in, or all-inside technique was used for meniscal repair, based on the location and the type of tear.
Rehabilitation
All patients were given instructions for protection, optimal loading, ice, compression, and elevation (POLICE principles) immediately after the injury. Physical therapy was not prescribed preoperatively; however, all patients were advised to perform simple exercises at home in order to regain range of motion (ROM) and maintain muscle power of the quadriceps and hamstrings. The postoperative rehabilitation protocol was modified according to concomitant procedures. Patients who underwent isolated ACL reconstruction or ACL reconstruction with additional meniscectomy were encouraged to immediately initiate progression of weightbearing as tolerated, with an emphasis on gaining ROM. On the contrary, patients treated with ACL reconstruction and additional meniscal repair had limits to their flexion ROM: 0° to 30° for the first 2 weeks, 0° to 60° for weeks 3 and 4, and 0° to 90° for weeks 5 and 6 with the use of a hinged brace. Starting from week 7, the brace was removed and full ROM exercises were initiated. A carefully progressive program with increased strengthening and proprioceptive exercises was followed by both groups as soon as full ROM was achieved. Return to sports activities was recommended no earlier than 8 months postoperatively depending on the type of sport and knee function.
Data Collection of Patient-Reported Outcomes
An extensive search in our computerized data repository was performed. Patient surgery data were collected and analyzed. Patients suitable for enrollment in the study were then contacted by telephone. For patients who were not reached immediately, calls were repeated at least twice. To all those who agreed to participate in the study, the PROMs were sent via email. Finally, all responses were collected and analyzed by 2 resident orthopaedic surgeons (G.C. and V.M.) who had not participated in the ACL reconstruction.
Evaluation of activity levels and quality of life was based on the following PROMs: the IKDC-SKF score, the Knee injury and Osteoarthritis Outcome Score (KOOS), the Lysholm knee score, the Tegner activity scale, and the 5-level EQ-5D (EQ-5D-5L). All PROMs have been validated and adapted in the Greek language. 23,28,29,45 Preinjury and preoperative Tegner scores were available in patients’ records, and study participants were asked to provide follow-up scores. Finally, patients were asked to provide a binary (yes/no) response to the following question to measure patient satisfaction: “Taking into account your level of pain, your daily life activities and your sport participation limitations and restrictions, do you consider the current state of your knee satisfactory?” All the above measures are considered important in the follow-up of patients with an ACL reconstruction according to a recent consensus statement. 41
Statistical Analysis
Statistical analyses were conducted with the use of the software IBM SPSS Statistics 26. Descriptive and inferential statistics were performed. All P values were 2-tailed with 95% CIs. The threshold for statistical significance was set at P < .05.
Patient and surgery characteristics as well as PROM scores were reported for the entire study sample. In addition, we conducted a subgroup analysis of differences in characteristics and outcomes in patients with meniscal injury by comparing those who underwent meniscectomy with those who underwent meniscal repair. The Kolmogorov-Smirnov Z test was used to determine if the data had a normal distribution. Continuous outcomes were described and analyzed using an independent-samples t test, while the chi-square test was used for categorical variables.
Pearson correlation analysis was performed on the entire study sample to assess the relationship of patient quality of life as assessed by the KOOS–Quality of Life (KOOS-QoL) subscale and EQ-5D-5L, with functional limitations in activities, and pain. Functional limitations were assessed by the Tegner score and the KOOS–Activities of Daily Living (KOOS-ADL) and KOOS–Sport and Recreation (KOOS–Sport) subscales, and pain was assessed by the KOOS–Pain subscale. The Pearson correlation coefficient (r) can range from –1 to +1, with values of r closer to +1 indicating a stronger positive linear relationship and values closer to –1 indicating a stronger negative linear relationship.
Multivariate linear regression analysis of scaled values for all the patients was also used to obtain a set of descriptive variables that were independently associated with PROMs. The variables included in the model were determined by their significance in the univariate comparisons, enabling the identification of the most important variables in explaining the outcome. In the derived model, all variables had a calculated P value <.05 when added to the other variables in the model. In this way, the independent variables of patient sex, body mass index (BMI), and age at surgery were examined with 5 different statistical models as the dependent variable: EQ-5D-5L, KOOS-QoL, KOOS–Sport, KOOS-ADL, and pre- to postoperative difference in Tegner score.
Results
Study Population
The mean follow-up was 13.2 years (range, 10.1-15.0 years). A total of 113 patients met the study’s inclusion criteria. The response rate was 94% (106 of 113 patients responded). Injury of the ACL occurred in 84% during sporting activities, in 10.4% during a car accident, in 2% at work, and in 4% during other activities. Moreover, 62 patients (58.5%) sustained the injury in the dominant leg and 44 patients (41.5%) in the nondominant leg. The retear rate was 2.8%. Patient characteristics including age, sex, and BMI are presented in Table 1.
Characteristics of the Patients Enrolled in the Study (N = 106) a
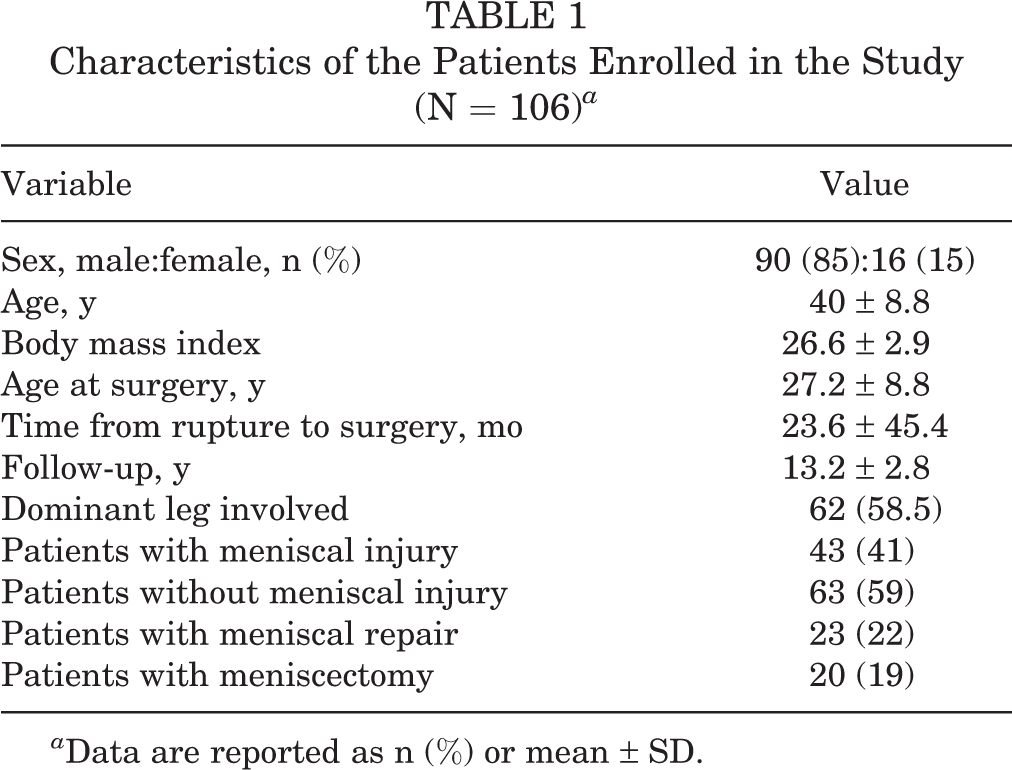
a Data are reported as n (%) or mean ± SD.
Regarding the subgroup analysis according to meniscal status, 43 patients (41%) had a concomitant meniscal injury. In 28 patients (65.1%) the medial meniscus was injured, in 11 patients (25.6%) the lateral meniscus was injured, and in 4 patients (9.3%) both menisci were injured. Meniscectomy was performed along with ACL reconstruction in 20 patients (46.5%), and concomitant meniscal repair was performed in 23 patients (53.5%). Descriptive characteristics of the meniscectomy and meniscal repair groups are presented in Table 2.
Differences in Characteristics Between Patients Treated With Meniscectomy Versus Meniscal Repair a
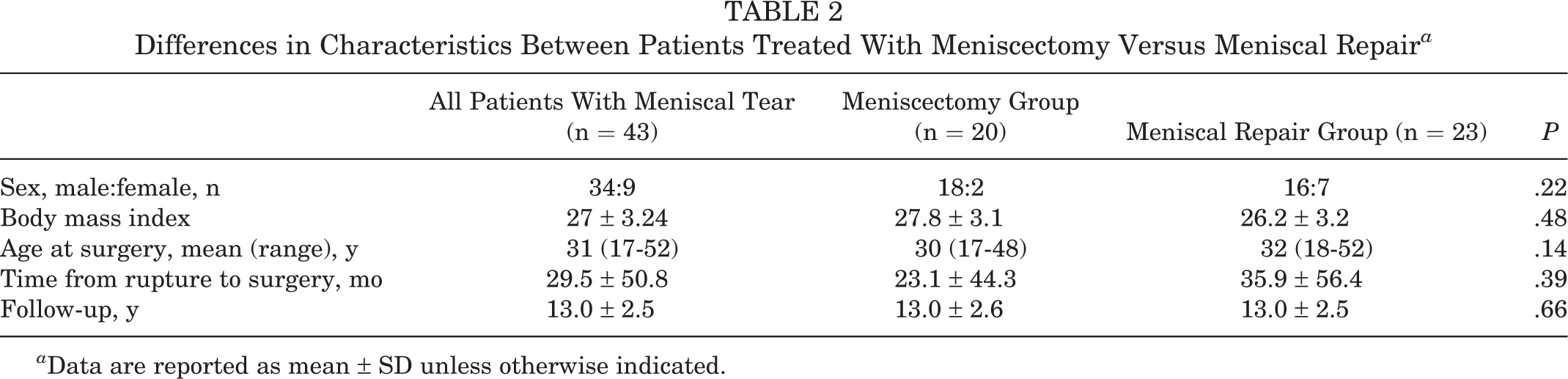
a Data are reported as mean ± SD unless otherwise indicated.
PROM Scores
The PROM scores for the total sample of the study along with the meniscal injury subgroups are presented in Table 3. Patients who underwent meniscal repair had statistically significantly better scores compared with patients who underwent meniscectomy on all PROMs except for the Tegner score and EQ-5D-5L.
Patient-Reported Outcome Scores for the Total Specimen and the Subgroups of the Study a
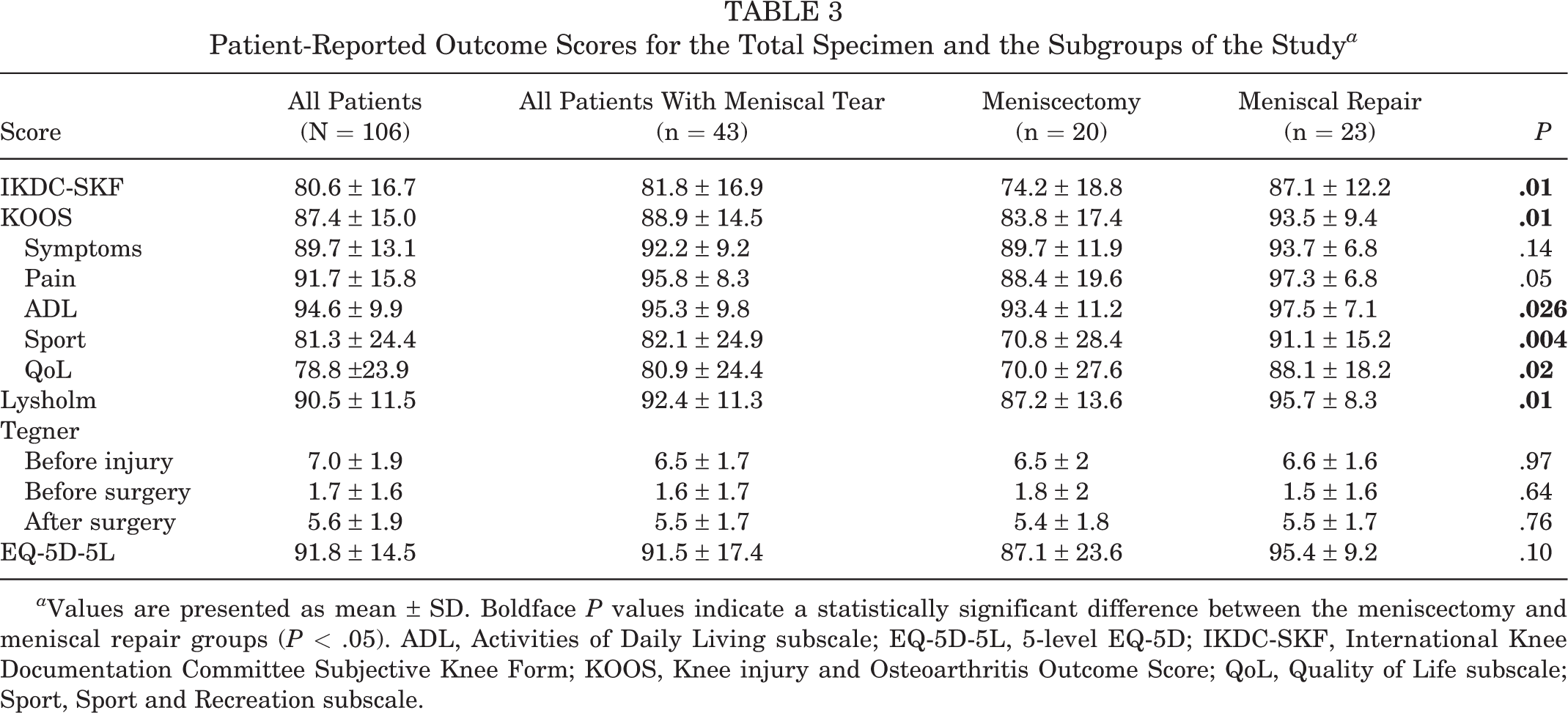
a Values are presented as mean ± SD. Boldface P values indicate a statistically significant difference between the meniscectomy and meniscal repair groups (P < .05). ADL, Activities of Daily Living subscale; EQ-5D-5L, 5-level EQ-5D; IKDC-SKF, International Knee Documentation Committee Subjective Knee Form; KOOS, Knee injury and Osteoarthritis Outcome Score; QoL, Quality of Life subscale; Sport, Sport and Recreation subscale.
Preoperative Versus Postoperative Patient Activity
Concerning patient activity levels, 81% of the patients were practicing sports ≥5 times a week before ACL rupture. After ACL injury and before reconstruction, only 12.3% were able to participate in even low-intensity sporting activities. The Tegner scores of patients before ACL rupture, before ACL surgery, and after ACL surgery can be seen in Figure 2. At the time of follow-up, Tegner scores were significantly higher compared with the presurgery period (5.6 ± 1.9 and 1.7 ± 1.6, respectively), with 48% of the patients being able to return to their previous high-level activities. However, as the competitive level increased, the return to previous level of activity decreased: 34.4% in Tegner scores 6 to 7 and 13.5% in Tegner scores 8 to 10. Meniscal status was not significantly correlated with Tegner score differences (P = .335). However, compared with patients who underwent meniscectomy, those who underwent meniscal repair had statistically significantly better results on the KOOS-ADL (P = .026) and KOOS–Sport (P = .004).
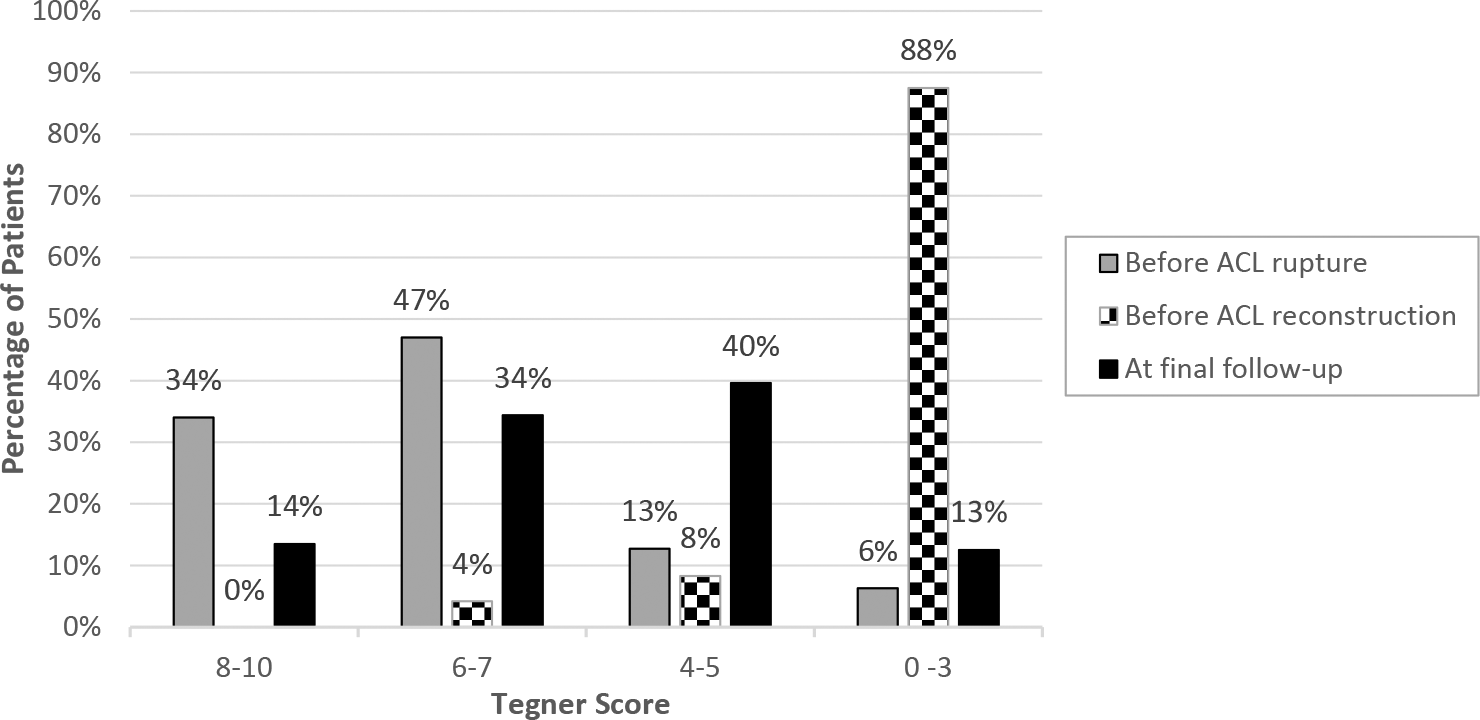
A bar chart demonstrating the Tegner score before anterior cruciate ligament (ACL) rupture, before ACL reconstruction, and at the final follow-up. Four subgroups of answers representing different activity demands in the Tegner activity scale have been created: 0 to 3, 4 to 5, 6 to 7, and 8 to 10.
Effect of ACL Injury and Reconstruction on Quality of Life
Concerning the impact of the injury to patient quality of life, the responses to the EQ-5D-5L indicated that 23.6% of patients experienced at least mild pain during daily activities; 21% experienced mild (n = 12), moderate (n = 8), or severe (n = 2) anxiety or depression; and finally, 64% altered their lifestyle and activities, even at a minimal rate.
Relationship of Patient Quality of Life With Functional Impairment in Activity and With Pain
There was a statistically significant, strong positive correlation between quality of life and functional impairment in activity levels, as shown in Table 4. A strong correlation between quality of life and pain was also found; however, quality of life was not significantly correlated with postoperative Tegner score.
Relationship of Patient Quality of Life With Functional Limitations and Pain a

a Boldface P values indicate statistical significance (P < .05). ADL, Activities of Daily Living subscale; EQ-5D-5L, 5-level EQ-5D; KOOS, Knee injury and Osteoarthritis Outcome Score; QoL, Quality of Life subscale; Sport, Sport and Recreation subscale.
Long-term Outcome Predictive Factors
Results of the regression models for the overall study sample are presented in Table 5. No statistically significant correlation was found between the dependent variables and patient sex, BMI, or mean age at surgery.
P Values for Multivariate Linear Regression Analysis Between Patient Characteristics and Postoperative PROM Scores a

a ADL, Activities of Daily Living subscale; EQ-5D-5L, 5-level EQ-5D; KOOS, Knee injury and Osteoarthritis Outcome Score; PROM, patient-reported outcome measure; QoL, Quality of Life subscale; Sport, Sport and Recreation subscale.
b Difference in Tegner score from preoperatively to postoperatively.
Patient Satisfaction
Overall, 90.6% (96 patients) responded “yes” and 9.4% (10 patients) responded “no” when asked if they were satisfied with the current state of their knee. Among the latter group, 6 patients were treated with an isolated ACL reconstruction and 4 underwent meniscectomy for an injured meniscus.
Discussion
The primary hypothesis of this study was supported by the analysis of the results, since patients treated with ACL reconstruction had satisfactory activity levels at a mean of 13.2 years of follow-up. In total, 90.6% of the patients considered their knee state satisfactory during their long-term follow-up evaluation. The mean Lysholm score of 90.5, the mean overall KOOS of 87.4, and the mean IKDC-SKF score of 80.6 revealed that the majority of patients had few or no symptoms. Moreover, the mean Tegner score of 5.6 showed that most patients continued to participate in sports, although only 48% were able to return to previous high-level activities. Although low, this a satisfactory percentage, since the return to competitive level of sport ranges from 34% to 56% in the literature. 1 Sex, age, and BMI were not found to be patient-specific risk factors in the present analysis, although sex and higher BMI have been considered negative predictive factors in other studies. 12,39
As far as the second objective is concerned, patients treated with meniscal repair had significantly better IKDC-SKF scores, Lysholm knee scores, and KOOS values compared with patients treated with meniscectomy. In fact, the mean differences between the 2 groups in KOOS values were not only statistically significant but also clinically important for KOOS ADL, Sport and QoL subscales, based on the findings of a 2018 study by Ingelsrud et al. 20 However, statistically significant differences between the groups were not observed for the EQ-5D-5L or Tegner score. It should be noted that the EQ-5D-5L is a generic and not knee-specific questionnaire, and the Tegner score evaluates the level of the activity and not the patients’ perceptions regarding the ability to participate in the activity. Based on the above, the results of the current study support the statement that meniscal preservation should be the first choice, especially when treating young patients, since clinical outcomes are worse after meniscectomy. 22
Third, there was a statistically significant, strong positive correlation between the quality of life scores (EQ-5D-5L and KOOS-QoL) and the functional limitations in activity level scores (KOOS-ADL and KOOS–Sport), as well as the KOOS–Pain score. Once again, each quality of life questionnaire is different and assesses different variables. The KOOS-QoL is a knee-specific questionnaire and examines patients’ feelings, emphasizing their knee condition. The EQ-5D-5L is a nonspecific questionnaire examining anxiety and depression feelings along with the ability to perform basic activities such as walking or dressing. The correlation between KOOS-QoL, KOOS–Sport, and KOOS–Pain subscores has been highlighted by a recent systematic review 14 ; however, to our knowledge there are no studies presenting a similar correlation for the EQ-5D-5L questionnaire, which means that the latter, although nonspecific, may be also used during the follow-up of patients with ACL reconstruction instead of other generic questionnaires such as the 36-Item Short Form Health Survey. In summary, the above correlations indicate that patients who have less pain and are able to easily perform activities of daily living and exercise will feel less anxious, less depressed, and less aware of their knee condition.
Comparing the present study’s results with the literature, only a few studies presenting patient-reported outcomes after anatomic ACL reconstruction, using a hamstring autograft through the anteromedial portal, were identified. Chen et al 10 compared hamstring with synthetic grafts and reported similar findings and, more specifically, a mean Lysholm score of 92.5, a mean KOOS-QoL of 78.6, a mean KOOS–Sport of 82.9, and a mean Tegner score of 5.5 at 10 years of follow-up in a sample of 73 patients. Sajovic et al 34,35 prospectively followed patients comparing the BPTB graft with the hamstring graft and reported a mean Lysholm score of 95 at 11 years and 94 at 17 years in a sample of approximately 30 patients. Tsoukas et al 42 compared reconstruction with nonoperative treatment and reported a mean IKDC score of 86.8 in 17 patients. Finally, Bourke et al, 7 in the largest series of patients reported so far, reported a mean IKDC score of 85. In their sample, 73% returned to their preinjury activity level. 7 Results between those studies and the present study are similar; however, it should be noted that none of the above studies examined meniscal status and its treatment effects.
Meniscal status is an important factor to consider when assessing outcomes after ACL reconstruction. In a study by Phillips et al 31 of 15,000 patients from the Swedish National Knee Ligament Registry, patients who underwent meniscal repair with ACL reconstruction had similar clinical outcomes compared with isolated ACL reconstruction and superior outcomes to those having undergone meniscectomy at 2 years of follow-up. Similar conclusions have also been reported by other long-term studies, in which meniscal repair has led to higher activity levels, higher patient satisfaction, and less OA. 25,30,40,43 In a study by the MOON (Multicenter Orthopaedic Outcomes Network) Group, having a lateral meniscectomy at the time of ACL surgery was considered a significant risk factor for poorer 10-year KOOS-QoL scores, 39 and in a study of Curado et al, 12 medial or lateral meniscectomy was considered as a major contributor to the development of OA. Moreover, in the study of Costa-Paz et al, 11 at 20 years of follow-up of patients treated with ACL reconstruction, those with meniscal injury were 3.9 times as likely to develop OA than patients without meniscal injury. Finally, in a similar long-term study, Melton et al 27 reported a mean IKDC of 84.2 in patients with ACL reconstruction and meniscal repair compared with a mean score of 70.5 in patients with meniscectomy. All these results are in accordance with the findings of the present study, which is the first to report ameliorated outcomes in all PROMs except for the Tegner score and the EQ-5D-5L score for patients treated with meniscal repair along with ACL reconstruction.
Similar results can be also found when comparing the results of the present study with studies on nonanatomic ACL reconstruction using a hamstring autograft. Janssen et al, 21 in a prospective study of 100 patients treated with a hamstring autograft, found a mean Lysholm score of 95 and a mean Tegner score of 6 and also identified meniscectomy as a risk factor for OA, although they used a transtibial technique with a bone mulch screw for femoral fixation and a washer lock for tibial fixation. Comparable Lysholm scores were also reported by Holm et al, 19 who examined 29 patients also operated on using a transtibial technique; they reported a mean Lysholm score of 86. Long-term report of the KOOS can be found in the study of Barenius et al, 4 who found a mean KOOS–Sport score of 64 and a mean KOOS-QoL score of 62 at 14 years of follow-up in 65 patients. In this case, results are inferior compared with the present study’s findings, but this can be explained by the fact that 77% of the patients of this study had a meniscal injury, but only 8 (16%) of them were treated with meniscal repair. Finally, long-term report of the IKDC score can be also found in the literature. In the study of Hanypsiak et al, 17 the mean IKDC score was 70.3 in 44 patients treated with BPTB or hamstring autograft. This difference may be attributed to the fact that 46% of the patients in the study of Hanypsiak et al, 17 had an associated cartilage injury during ACL reconstruction, whereas in the present study, cartilage injury was an exclusion criterion.
When examining studies with even longer follow-up, some differences can be noticed. In the study of Salmon et al, 36 in 139 patients, the mean IKDC score was 89, at 20 years postoperatively. This higher score can be explained by the fact that in the study of Salmon et al, 36 , patients with a concomitant meniscal injury were not included. In the study of Zaffagnini et al, 46 who examined 52 patients, the mean Lysholm score was 85.7, the median Tegner score was 4, the mean overall KOOS was 83.7, the mean KOOS–Sport score was 76, and mean the KOOS-QoL score was 71. Minor differences can be noticed, but again, this study refers to a 2-stranded hamstring graft placed with an over-the-top technique, and moreover, ACL reconstruction was accompanied by extra-articular lateral tenodesis, 2 important differences compared with our sample.
Similar PROM scores have been reported when comparing the results of the present study with those of studies on other grafts. Using a BPTB autograft, Wu et al 44 reported a mean Lysholm score of 88 and a mean IKDC score of 80 at 10.3 years of follow-up. Similarly, Hart et al 18 reported a mean Lysholm score of 93 and a mean Tegner score of 6 at 10 years of follow-up. Lastly, Shelbourne and Gray 38 reported a mean IKDC score of 83.6 at 14 years of follow-up in a sample of 920 patients. Finally, similar Lysholm scores have also been reported by authors in patients with a quadriceps autograft; however, long-term studies are still missing regarding this type of graft. 15
Limitations
The most important limitation of this study is the lack of clinical evaluation of patients. A complete follow-up including a physical examination, specific clinical and functional tests, knee arthrometer measurements, and radiological examination for the possibility of knee OA was not possible because of the COVID-19 pandemic. However, this complete follow-up remains the goal for the authors since long-term follow-up for the patients of the study will be continued. Moreover, the size of the sample could be considered a limitation. Another limitation is that the preoperative score for PROMs is missing with the exception of the Tegner score, which can be considered as an intrinsic limitation in such a long-term retrospective study. Finally, small modifications of the suggested physical therapy program over the years can be considered a limitation. However, changes were minor and only made based on contemporary advances of the literature.
Conclusion
Patients had few or no symptoms and considered their knee state satisfactory 13.2 years after anatomic ACL reconstruction. Patients with concomitant meniscal ruptures having undergone meniscal repair had improved PROMs compared with those treated with meniscectomy. Finally, functional limitations in activities of daily living, recreational activities, and sports were interrelated with quality of life and did not seem to be affected by patient sex, BMI, or age.
Footnotes
Final revision submitted February 7, 2023; accepted March 9, 2023.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University Hospital of Larissa, Greece (study No. 48106).