
Abstract
Background:
The Anterior Cruciate Ligament–Quality of Life (ACL-QOL) questionnaire is a widely used and effective scale for quality of life in patients with chronic anterior cruciate ligament (ACL) injury.
Purpose:
To translate and adapt the ACL-QOL questionnaire for Chinese patients and evaluate its reliability, validity, and responsiveness in this population.
Study Design:
Cohort study (diagnosis); Level of evidence, 2.
Methods:
Translation and adaptation were conducted in accordance with the guidelines of the A merican Academy of Orthopaedic Surgeons Outcome Committee. Included were 121 patients who were diagnosed with a chronic ACL injury and underwent ACL reconstruction between January 2020 and June 2021. Preoperatively, patients completed the simplified Chinese version of the ACL-QOL (ACL-QOL-C), the Knee injury and Osteoarthritis Outcome Score, and the 12-Item Short Form Health Survey. The ACL-QOL-C was also completed at 12- and 24-week follow-ups. Psychometric evaluations were then performed and included score distribution, internal consistency, test-retest reliability, construct validity, and responsiveness.
Results:
The Cronbach alpha ranged from .905 to .975, indicating excellent internal consistency, and the intraclass correlation coefficient ranged from 0.864 to 0.985, indicating excellent test-retest reliability. The consistency between the above results and our a priori hypotheses was more than 70% (35/42), indicating good construct validity. The standard error of measurement and effect size of the total score and each item of the ACL-QOL-C were >0.8 at the final follow-up, indicating good responsiveness.
Conclusion:
The English version of the ACL-QOL has been successfully translated into Chinese, and it has been shown to be applicable for the assessment of the quality of life in Chinese patients with chronic ACL injury.
Anterior cruciate ligament (ACL) injury is one of the most common musculoskeletal injuries of the knee joint. To assess the quality of life after an ACL injury, determine whether surgical treatment is necessary, and guide postoperative functional rehabilitation exercises, physicians need a tool that can evaluate the condition of the patient’s entire knee joint. The Anterior Cruciate Ligament–Quality of Life (ACL-QOL) questionnaire, which was first published in 1998, is a subjective scale for measuring the quality of life of patients with chronic ACL injury. 10 It has been proven to be reliable, responsive, and valid to clinical changes and is recommended for the evaluation of patients with chronic ACL injury both before and after treatment. 10
The ACL-QOL has been translated and verified into Brazilian, 13 Persian, 3 and Turkish 6 ; however, it has not been translated and verified into Chinese. Thus, the purpose of this study was to perform a cross-cultural adaptation, translate the original version of the ACL-QOL into simplified Chinese, and validate the simplified Chinese version.
Methods
The protocol for this study was approved by the ethics committee of our hospital, and all procedures involving human participants in this study were performed in accordance with the 1964 Helsinki Declaration and its subsequent amendments or similar ethical standards. All participants provided written informed consent.
ACL-QOL Questionnaire
The ACL-QOL is a disease-specific and patient-based tool and includes 31 questions in 5 domains: Symptoms and Physical Complaints (SPC), with 5 items; Work-Related Concerns (WRC), with 4 items; Recreational Activities and Sport Participation or Competition (R&S), with 12 items; Lifestyle, with 6 items; and Social and Emotional Concerns (SE), with 5 items. Each item is scored using a 100-mm visual analog scale, with the mean score for each domain and the mean total score ranging from 0 to 100. The higher the score, the higher the quality of life related to the knee joint. 10
Translation and Cross-cultural Adaptation of the ACL-QOL
We followed the 5 steps recommended by the American Academy of Orthopaedic Surgeons Outcome Committee 12 for the translation and cross-cultural adaptation process of the original ACL-QOL as follows:
Step 1: Initial Translation. Two independent, bilingual, Chinese native speakers translated the ACL-QOL from its English version into simplified Chinese. One was a skilled knee surgeon and the other was a Chinese student who did not have a medical background.
Step 2: Synthesis of the Translations. A meeting was held to discuss the differences between the 2 translations of the original version and a consensus was reached.
Step 3: Back translation. The initial Chinese version was backtranslated into English by 2 independent bilingual translators whose first language was English. These translators were not involved in the initial translation and had never read the English version of the ACL-QOL previously.
Step 4: Review by the Expert Committee. The initial Chinese version was evaluated by an expert committee, with 2 sports medicine specialists, 2 rehabilitation physicians, and 2 language experts. Any differences, ambiguities, or other opinions were discussed during the meeting. After considering all the suggestions, a provisional Chinese version was developed, which was equivalent to the concept of the original version.
Step 5: Pretesting. The provisional Chinese version of the ACL-QOL was tested on 20 patients preparing for ACL reconstruction to determine their understanding of the Chinese version. We collected their feedback and held a third consensus meeting to develop the final version of the ACL-QOL (ACL-QOL-C).
Patients and Data Acquisition
The study sample consisted of patients diagnosed with unilateral ACL injury who were planning to undergo ACL reconstruction at our hospital. The inclusion criteria were age between 18 and 60 years and injury duration of >1 month. The exclusion criteria were as follows: previous knee surgery; knee lesions; multiple injuries around the knee (eg, fracture around the knee joint, knee ligament injury other than the ACL, injury of articular cartilage and meniscus in the knee joint, or injury of important nerves and blood vessels around the knee joint); grade 3 collateral ligament injury; bilateral ACL injury; and posterior cruciate ligament injuries.
At the time of admission for reconstruction surgery, the patients provided demographic information, including age, sex, height, and weight. All participants then completed the ACL-QOL-C, the Knee injury and Osteoarthritis Outcome Score (KOOS), and the 12-Item Short Form Health Survey (SF-12) preoperatively. The KOOS and SF-12 were used to measure construct validity. To assess test-retest reliability, a subsample of participants completed the ACL-QOL-C again after 5 to 7 days (second round); this interval was chosen because 5 to 7 days were reported as a sufficient time interval to measure retest reliability. 16 Finally, to evaluate responsiveness, the patients were asked to complete the ACL-QOL-C when they visited our hospital for a routine physical examination at the 12-week (third round) and 24-week follow-ups (fourth round).
KOOS and SF-12 Questionnaires
The KOOS, which consists of 5 subscales—Pain, Symptoms, Activities of Daily Living, Sport and Recreation, and Quality of Life—is used to evaluate subjective knee function. 2 It has shown reliability, validity, and responsiveness in different populations with different pathologies, injury durations, ages, and activity levels; its Chinese version has also been verified and validated. 4 The SF-12 has 12 items, and Physical Component Summary (PCS) and Mental Component Summary (MCS) scores are calculated using a standard scoring algorithm. 5 The Chinese version of the SF-12 has been verified, with good responsiveness, reliability, and effectiveness. 7
Psychometric Assessments and Statistical Analysis
We assessed the ACL-QOL-C in terms of its reliability (the degree to which the measurement is free from error), content validity (comprehensiveness and relevance of the scale items), construct validity (the degree of consistency with other outcome instruments), and responsiveness (the ability of structures to be measured over some time). All statistical analyses were performed in SPSS Version 25.0 for Windows (IBM). Statistical significance was set at P ≤ .05.
Measurement error, internal consistency, and test-retest reliability were analyzed to assess the reliability of the ACL-QOL-C. 18 Measurement error was analyzed using the standard error of measurement (SEM) and the minimal detectable change (MDC). 11 The degree of internal consistency was derived by the Cronbach α coefficient of the scale, in which α values of > .7, .8 and .9 were considered acceptable, good, and excellent, respectively. 16 In addition, the effect of each item of the scale on the overall Cronbach α value was assessed by removing 1 item at a time. 16 Test-retest reliability between the 2 preoperative ACL-QOL-C rounds was assessed using the intraclass correlation coefficient (ICC) based on a 2-way analysis of variance in a random-effects model 9 ; ICC values were reported with 95% CIs. Reliability was considered good if ICC values were >0.8 and was considered excellent if ICC values 9 were >0.9. Bland-Altman plots were used to evaluate within-patient variation using limits of agreement 15 (mean difference ± 1.96 SD).
Content validity is measured using patient feedback, response rate, and floor/ceiling effects. 19 For this study, a floor/ceiling effect of <15% was considered good content validity. Since there is no gold standard to evaluate the construct validity of the ACL-QOL-C, a hypothesis test was used 11,14 ; and hypotheses were formulated regarding the association of the ACL-QOL-C scores (overall and by domain) with the SF-12 PCS, SF-12 MCS, and KOOS subscale scores. Associations were measured using the Pearson correlation analysis, with r values interpreted as none to slight (0.01-0.20), fair (0.21-0.40), moderate (0.41-0.60), substantial (0.61-0.80), or almost perfect 16 (0.81-1). The following 3 hypotheses were formulated:
Four of the ACL-QOL-C domains (SPC, WRC, R&S, and Lifestyle) would have at least a moderate correlation with the SF-12 PCS and a lower-than-fair correlation with the SF-12 MCS.
The correlation between the overall ACL-QOL-C and the KOOS subscales would be stronger than that between the ACL-QOL-C and the SF-12 PCS and MCS.
The SPC, WRC, R&S, and Lifestyle domains of the ACL-QOL-C would have at least a moderate correlation with the KOOS subscales, and the SE domain would have a lower-than-fair correlation with the KOOS subscales.
Good construct validity was considered as ≥70% of the stipulated a priori hypotheses having been met. 11
Responsiveness of the ACL-QOL-C was evaluated by comparing the preoperative and postoperative scores 12 and 24 weeks after surgery. The 2 indicators of reactivity evaluation were standardized response mean (SRM) and effect size (ES), with values considered small if <0.50, intermediate if between 0.50 and 0.80, and large 11 if >0.80.
Results
Translation and Cross-cultural Adaptation
Because the ACL-QOL items are easy to understand, there were no issues with the forward and back translation process. In addition, none of the study participants indicated that the questionnaire was difficult to understand. The final version of the ACL-QOL-C is shown in the Supplemental Material (available separately).
Patients
A total of 138 patients (134 men and 4 women) met the inclusion criteria, and 121 patients (117 men and 4 women) completed the ACL-QOL-C preoperatively. All patients underwent ACL reconstruction between January 2020 and June 2021. Two participants were unavailable for the follow-up in the third collection of the ACL-QOL-C (12 weeks postoperatively), and 5 participants were unavailable for the follow-up in the fourth collection (24 weeks postoperatively). Thus, 121 patients were included in the analysis of measurement error, floor/ceiling effects, internal consistency, and validity of the ACL-QOL-C. To evaluate test-retest reliability, a subsample of 50 patients were asked to complete 2 preoperative rounds, and the responsiveness of the scale was examined using the data of the 114 patients who completed the ACL-QOL-C 4 times. Table 1 shows the detailed demographic characteristics of the primary participants.
Characteristics of the Study Participants (N = 121) a

a BMI, body mass index.
Reliability
The Cronbach α for the total score and each of the 5 domains of the ACL-QOL-C ranged from .905 to .975, indicating excellent internal consistency. In addition, no improvement in the Cronbach α was found when a single scale item was removed, and the α value increased slightly when the item was reinstated, which indicated that removing any single item did not affect the overall reliability of the questionnaire.
The ICC for the total score, as well as 4 of the 5 domains, was >0.9, indicating excellent test-retest reliability of the ACL-QOL-C (Table 2). Only the SPC domain had a lower ICC value (0.864). In addition, Bland-Altman plots showed that most data points were within the 95% limit of agreement, which confirmed that there was no systematic error in the 2 preoperative rounds of the questionnaire. The SEM as well as the individual and group MDC values of the ACL-QOL-C and each domain are presented in Table 2.
Test-Retest Reliability and Measurement Error of ACL-QOL-C (n = 50 Patients) a

a ACL-QOL-C, Chinese version of the Anterior Cruciate Ligament–Quality of Life; ICC, intraclass correlation coefficient; MDC, minimal detectable change; R&S, Recreational Activities and Sport Participation or Competition; SE, Social and Emotional Concerns; SPC, Symptoms and Physical Complaints; WRC, Work-Related Concerns.
b Data are reported as mean ± SD.
Validity
The score distribution showed no floor effect (0%-1.7% [<15%]) or ceiling effect (0%-6.7% [<15%]) in the ACL-QOL-C. The consistency between the results and our a priori hypotheses was 35 of 42 (>70%), indicating that the ACL-QOL-C has good construct validity (Table 3).
Correlation of the ACL-Qol-C With the SF-12 and KOOS a
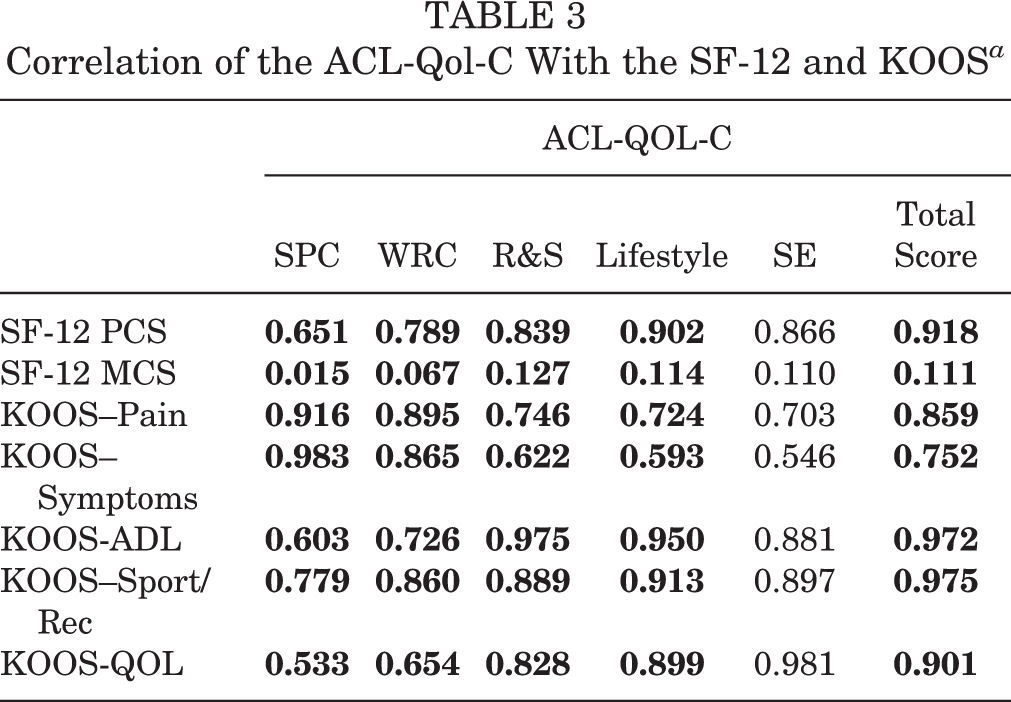
a Data are presented as Pearson correlation coefficients (r). Bold r values indicate correlations that met the hypotheses for establishing construct validity. ACL-QOL-C, Chinese version of the Anterior Cruciate Ligament–Quality of Life; ADL, Activities of Daily Living; KOOS, Knee injury and Osteoarthritis Outcome Score; MCS, Mental Component Summary; PCS, Physical Component Summary; QOL, Quality of Life; R&S, Recreational Activities and Sport Participation or Competition; SE, Social and Emotional Concerns; SF-12, 12-Item Short Form Health Survey; SPC, Symptoms and Physical Complaints; Sport/Rec, Sport and Recreation; WRC, Work-Related Concerns.
Responsiveness
The data regarding the responsiveness of the ACL-QOL-C are shown in Table 4. The 5 domains and total score of the ACL-QOL-C increased significantly at 12 and 24 weeks after treatment when compared with first-round preoperative values. The comparison of the first-round preoperative scores with the final scores at 24 weeks postoperatively indicated that the SRM and ES of the total score and each domain were >0.8, reflecting the high responsiveness of the tool.
Responsiveness of the ACL-QOL-C a
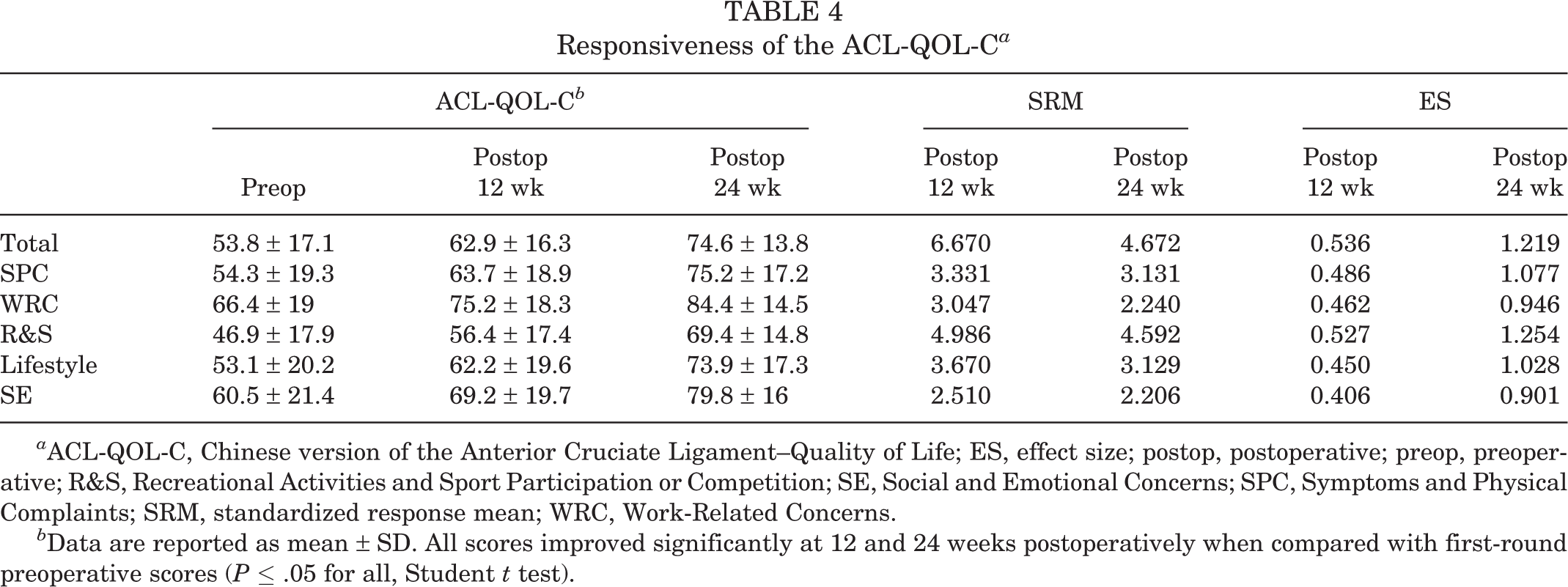
a ACL-QOL-C, Chinese version of the Anterior Cruciate Ligament–Quality of Life; ES, effect size; postop, postoperative; preop, preoperative; R&S, Recreational Activities and Sport Participation or Competition; SE, Social and Emotional Concerns; SPC, Symptoms and Physical Complaints; SRM, standardized response mean; WRC, Work-Related Concerns.
b Data are reported as mean ± SD. All scores improved significantly at 12 and 24 weeks postoperatively when compared with first-round preoperative scores (P ≤ .05 for all, Student t test).
Discussion
The ACL-QOL-C was found to have excellent internal consistency (Cronbach α = .905 and .975), excellent test-retest reliability (ICC, 0.864-0.985), no floor or ceiling effects, good construct validity, and a high degree of responsiveness (SRM and ES >0.8). Thus, the simplified Chinese version of the ACL-QOL questionnaire was found to be sufficient to evaluate the health-related quality of life of patients with ACL injury.
In the validation studies of the ACL-QOL in Turkey, 6 Brazil, 13 and Iran, 3 all versions showed a strong correlation among all items of the questionnaire. In our study, the total scores and scores for each of the 5 domains had excellent internal consistency (Cronbach α value >0.9). Most of the Cronbach α values between each item in a domain and the overall domain were >0.7; only items 13, 16, and 18 in the R&S domain had lower values (α = .6859, .696, and .663, respectively). These 3 items describe the patients’ degree of fear, depression, and caution when it comes to physical and recreational activities. As Chinese culture discourages emotional expression 8 and Chinese people generally downplay their emotions, this may be the reason for the lower α values in the R&S domain.
The ACL-QOL-C showed excellent test-retest reliability, with 4 of the 5 domains having an ICC of >0.9. As there are 32 items in the ACL-QOL-C, it is not easy for patients to remember their previous answers. We believe that the main reason for this result is that the patient’s functional status and daily life did not change significantly within the 5- to 7-day interval between the first and second preoperative rounds. The verification results in other language versions are the same as ours. The MDC and the low values of SEM found in our study indicate that the ACL-QOL-C can detect small clinical changes and changes at the individual level.
Regarding construct validity, the correlation between the total score, every domain of the ACL-QOL-C, and the SF-12 MCS was weak but still significant (P < .05), indicating that the functional status of the knees of patients with ACL injury affects their psychological status. The reason for the weak correlation may be related to the psychological characteristics of Chinese people, as mentioned above. 8 In the Persian 3 and Brazilian 13 versions, the SF-36 PCS and MCS scores were moderately related to the ACL-QOL. This is the first time that a correlation analysis has been conducted between the KOOS and ACL-QOL. Results indicated that the SPC domain of the ACL-QOL-C was only moderately correlated with the KOOS–Quality of Life subscale (r = 0.533). This finding indicates that although there was some impact of ACL injury on the living habits and psychological state of the study patients, the impact was not significant.
The quality of scale responsiveness is an important factor in determining whether the scale can be used in prospective clinical research. 17 At 12 weeks after surgery, the patient’s basic knee function has not fully recovered. In addition, patients fear reinjury after surgery, which leads to a reduction or cessation of exercise participation after the operation 1 ; thus, the responsiveness of the questionnaire cannot be fully reflected. This is the reason for the small to intermediate ES values for the ACL-QOL-C at 12 weeks postoperatively (0.406-0.536). At 24 weeks postoperatively, the ES was high overall and for each domain (0.901-1.254), which indicates that the ACL-QOL-C was sensitive to the changes in the functional status of the patients in the weeks after ACL reconstruction. The Turkish translation of the ACL-QOL also had a high degree of responsiveness; however, when the 2-year postoperative scores were compared with those at 16 weeks postoperatively, it was found that the ES values for all domains except the SPC had decreased. 6 Responsiveness was not tested in the validation of the other translations. 3,6,13
Limitations
One limitation of this study was that our patients were recruited from a sports center in a military hospital; thus, most of the research participants were male patients and soldiers. Going forward, we will seek cooperation with other sports centers to recruit more participants to further test and improve the ACL-QOL-C. Second, the target language was simplified Chinese. However, China is a multiethnic country, with many ethnic minorities, each with their own language. Therefore, attention must be paid to national cultural differences when the ACL-QOL-C is used.
Conclusion
Our study indicate that the translated simplified Chinese version of the ACL-QOL is a reliable, valid, and responsive instrument for a Chinese population with chronic ACL injury.
Supplemental material for this article is available at https://journals.sagepub.com/doi/full/10.1177/23259671231175935#supplementary-materials.
Supplemental Material
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671231175935 - Translation and Validation of a Simplified Chinese Version of the Anterior Cruciate Ligament–Quality of Life Questionnaire
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671231175935 for Translation and Validation of a Simplified Chinese Version of the Anterior Cruciate Ligament–Quality of Life Questionnaire by Jun Kou, Bing Deng, Jinbiao Liu, Jun Wen, Li Yin, Qingyun Xie and Wang Wei in Orthopaedic Journal of Sports Medicine
Footnotes
Acknowledgment
The authors thank the College of Medicine, Southwest Jiaotong University, and the Department of Orthopedics, General Hospital of Western Theater Command, People’s Republic of China for technical and equipment support.
Final revision submitted February 14, 2023; accepted March 2, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: The present work was supported by the General Hospital of Western Theater Command Project (grant 2021-XZYG-B05), the Cadre health care project of Sichuan Province (grant 2017-1302), the Fundamental Research Funds for the Central Universities (grants 2682022ZTPY036 and 2682022ZTPY043), the Projects in the Management of Traditional Chinese Medicine in Sichuan Province (grant 2023MS215) and the Department of Science and Technology of Sichuan Province (CN) Project (grants 2023YFS0052 and 2019YFS0269). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the General Hospital of Western Theater Command (reference No.2021-XYZG-B05)
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.