
Abstract
Background:
Despite the prevalence of patient-reported outcomes (PROs) to evaluate results after anterior cruciate ligament (ACL) reconstruction, there exists little standardization in how these metrics are reported, which can make wider comparisons difficult.
Purpose:
To systematically review the literature on ACL reconstruction and report on the variability and temporal trends in PRO utilization.
Study Design:
Systematic review.
Methods:
We queried the PubMed Central and MEDLINE databases from inception through August 2022 to identify clinical studies reporting ≥1 PRO after ACL reconstruction. Only studies with ≥50 patients and a mean 24-month follow-up were considered for inclusion. Year of publication, study design, PROs, and reporting of return to sport (RTS) were documented.
Results:
Across 510 studies, 72 unique PROs were identified, the most common of which were the International Knee Documentation Committee score (63.3%), Tegner Activity Scale (52.4%), Lysholm score (51.0%), and Knee injury and Osteoarthritis Outcome Score (35.7%). Of the identified PROs, 89% were utilized in <10% of studies. The most common study designs were retrospective (40.6%), prospective cohort (27.1%), and prospective randomized controlled trials (19.4%). Some consistency in PROs was observed among randomized controlled trials, with the most common PROs being the International Knee Documentation Committee score (71/99, 71.7%), Tegner Activity Scale (60/99, 60.6%), and Lysholm score (54/99, 54.5%). The mean number of PROs reported per study across all years was 2.89 (range, 1-8), with an increase from 2.1 (range, 1-4) in studies published before 2000 to 3.1 (range, 1-8) in those published after 2020. Only 105 studies (20.6%) discretely reported RTS rates, with more studies utilizing this metric after 2020 (55.1%) than before 2000 (15.0%).
Conclusion:
There exists marked heterogeneity and inconsistency regarding which validated PROs are used in studies related to ACL reconstruction. Significant variability was observed, with 89% of measures being reported in <10% of studies. RTS was discretely reported in only 20.6% of studies. Greater standardization of outcomes reporting is required to better promote objective comparisons, understand technique-specific outcomes, and facilitate value determination.
Keywords
Anterior cruciate ligament (ACL) tears occur in an estimated 250,000 athletes each year, most commonly in those 15 to 25 years of age. 15 The knee instability that results from an ACL injury is a source of significant morbidity, as it has been estimated that the ACL provides >85% of the restraining force against anterior tibial translation. 35 Secondary restraint provided by the iliotibial band, medial collateral ligament, and fibular collateral ligament is insufficient to compensate, making arthroscopic surgical reconstruction the gold standard in most athletes. Alternative approaches, including ACL repair and nonsurgical treatment, have demonstrated acceptable short-term patient-reported outcomes (PROs) but higher rates of adverse events and repeat surgery. 23,27 Despite an understanding of ACL reconstruction—surgery that is estimated to be successful in 75% to 97% of cases—there remains little consensus on the most effective reconstruction techniques. 1,4,40 Uncertainty regarding graft type, fixation, and tunnel placement technique continues to motivate a large volume of research. The difficulty seen in measuring the relative effectiveness of reconstruction techniques is likely influenced by the many outcome measures used to define and compare results.
Despite agreement regarding the importance of prioritizing patient outcomes, traditional compensation models have centered on reimbursement on the services rendered by an organization. A recalibration has led to the development of value-based models in which reimbursement is contingent upon the ratio of cost to quality. An integral part of quality assessment is a patient’s subjective evaluation of outcome. In an effort to help practicing surgeons navigate this evolving landscape and meet the demands for lower costs and quality improvement, the American Academy of Orthopaedic Surgeons published a value-based continuum in 2020. 3 Furthermore, the Patient-Reported Outcomes Measurement Information System (PROMIS) developed by the US National Institutes of Health serves as example of how national organizations are emphasizing the role of PROs in defining the concept of value. 5,9
Much of the influential literature on outcomes after ACL reconstruction has utilized PROs in the analysis and determination of effectiveness. The wide variety of PROs used in this space to evaluate pain, function, and satisfaction limits our ability to compare results. As health care payer models continue to increase their focus on PROs, there is now greater emphasis on standardized reporting such that results from multiple studies can be objectively compared. Thus, the purpose of this study is to survey the current ACL reconstruction outcomes literature and quantify the variability in PRO reporting, as well as understand temporal and study design–related trends. We hypothesize that there are a large number of PROs used and that the number of PROs per study is increasing over time.
Methods
A systematic review of the literature was conducted according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines. 9 A comprehensive search of the PubMed Central and MEDLINE databases was performed from inception through August 2022. The search strategy utilized Medical Subject Headings and keywords for ACL reconstruction and PROs.
Clinical outcome studies were included if they met the following criteria: they (1) were outcome-based studies after primary or revision ACL reconstruction reporting ≥1 PRO, (2) were written in the English language, and (3) analyzed ≥50 patients with a mean follow-up of ≥24 months. This decision was made a priori to limit our analysis to larger, high-quality studies reporting outcomes beyond the acute postoperative period. Studies were excluded if they (1) were systematic reviews/meta-analyses, letters to the editor, elemental analyses, or case reports; (2) had a primary radiographic focus; (3) did not report PROs; (4) were not printed in the English language; and (5) did not have available text. Studies were included regardless of the level of evidence.
After the removal of duplicates, the title and abstract of 2296 articles were screened, of which 1697 were determined to not meet inclusion criteria, leaving 599 articles in the full-text review (Figure 1). After full-text review, 510 studies met eligibility criteria and were included.
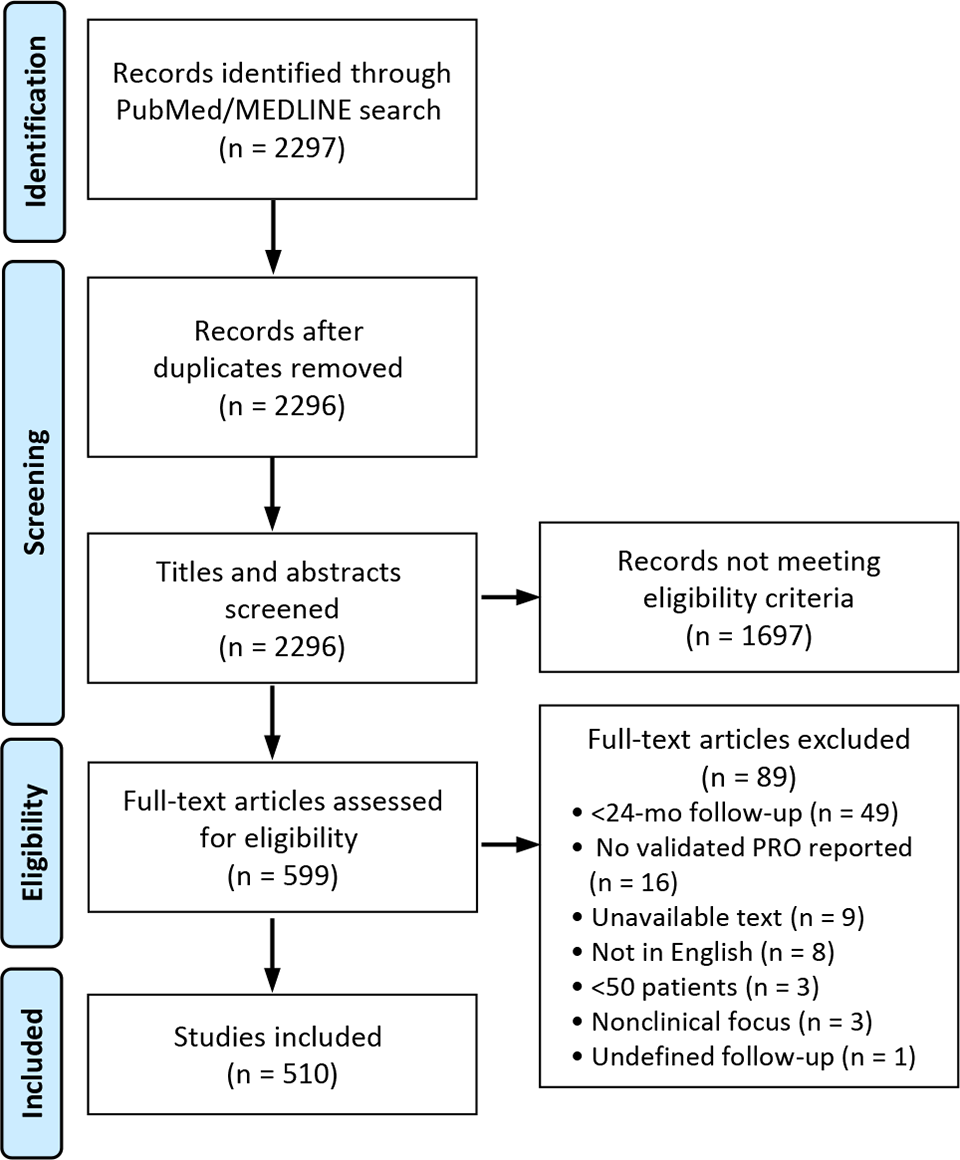
Study-selection process per a PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) diagram. PRO, patient-reported outcome.
Data were extracted from each study and organized into a spreadsheet for further analysis. Extracted data included title, year of publication, journal of publication, design, PROs, and whether discrete rates of return to sport (RTS) were reported (yes/no).
Results
Study Characteristics and PRO Measures
A total of 510 studies published between 1991 and 2022 met inclusion criteria and were included in this analysis (Table 1). Overall, 40.6% were retrospective studies, 27.1% prospective cohort studies, and 19.4% prospective randomized studies. The number of studies published demonstrated a positive trend over time, with significantly more studies published after 2020 (n = 138) than before 2000 (n = 23). Only 105 (20.6%) studies discretely reported rates of RTS at any level (same, higher, or lower).
Study Characteristics (N = 510) a

a PRO, patient-reported outcome; RCT, randomized controlled trial; RTS, return to sport.
b Instances of reporting as a discrete, freestanding measure.
PRO Measures
Across all studies, 72 distinct PROs were identified. The mean number of PROs per study was 2.89 (range, 1-8). Across studies, 14% reported 1 PRO; 24%, 2 PROs; 36%, 3 PROs; and the remaining 26%, ≥4 PROs (Figure 2).

Number of PROs reported per study, across all studies. PRO, patient-reported outcome.
The most commonly reported PROs, regardless of study type or period, were the International Knee Documentation Committee (IKDC) score (63.3%), Tegner Activity Scale (52.4%), Lysholm score (51.0%), and Knee injury and Osteoarthritis Outcome Score (KOOS; 35.7%) (Figure 3).

The 14 most frequently reported PROs across studies. ACL-QoL, Anterior Cruciate Ligament Quality of Life; ACL-RSI, Anterior Cruciate Ligament–Return to Sport after Injury; EQ-5D, EuroQol 5 Dimensions; IKDC, International Knee Documentation Committee; KOS-ADLS, Knee Outcome Survey–Activity of Daily Living Subscale; KOOS, Knee injury and Osteoarthritis Outcome Score; PRO, patient-reported outcome; SANE, Single Assessment Numeric Evaluation; VAS, visual analog scale; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index. *Either the 12- or the 36-Item Short Form Health Survey.
No other PRO measure was utilized in >12% of studies. With the exception of registry-based studies, the 4 most frequently cited PRO measures did not change when results were stratified by study type (Table 2). Among registry-based studies, the EuroQol 5 Dimensions was the third-most common PRO, in 6 (16.7%) studies.
Patient-Reported Outcome Use Stratified by Study Type a

a Data in parentheses are the number of studies. ACL-QoL, Anterior Cruciate Ligament Quality of Life; EQ-5D, EuroQol 5 Dimensions; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; VAS, visual analog scale.
b From most to least common.
c Either the 12- or the 36-Item Short Form Health Survey.
Temporal Trends
The mean number of PROs increased from 2.1 (range, 1-4) per study before 2000 to 3.1 (range, 1-8) after 2020 (Table 3). Similarly, the proportion of studies discretely reporting RTS as a stand-alone metric increased from 3 studies (15.0%) before 2000 to 49 (55.1%) after 2020. The relative use of the KOOS, Marx scale, visual analog scale for pain, and 12- or 36-Item Short Form Health Survey increased over time, while utilization of the IKDC, Tegner, and Lysholm scales remained relatively constant. Use of the Cincinnati/Noyes rating system decreased over time. PRO and RTS stratified by year are detailed in Table 3.
PRO and RTS Use Stratified by Publication Year a
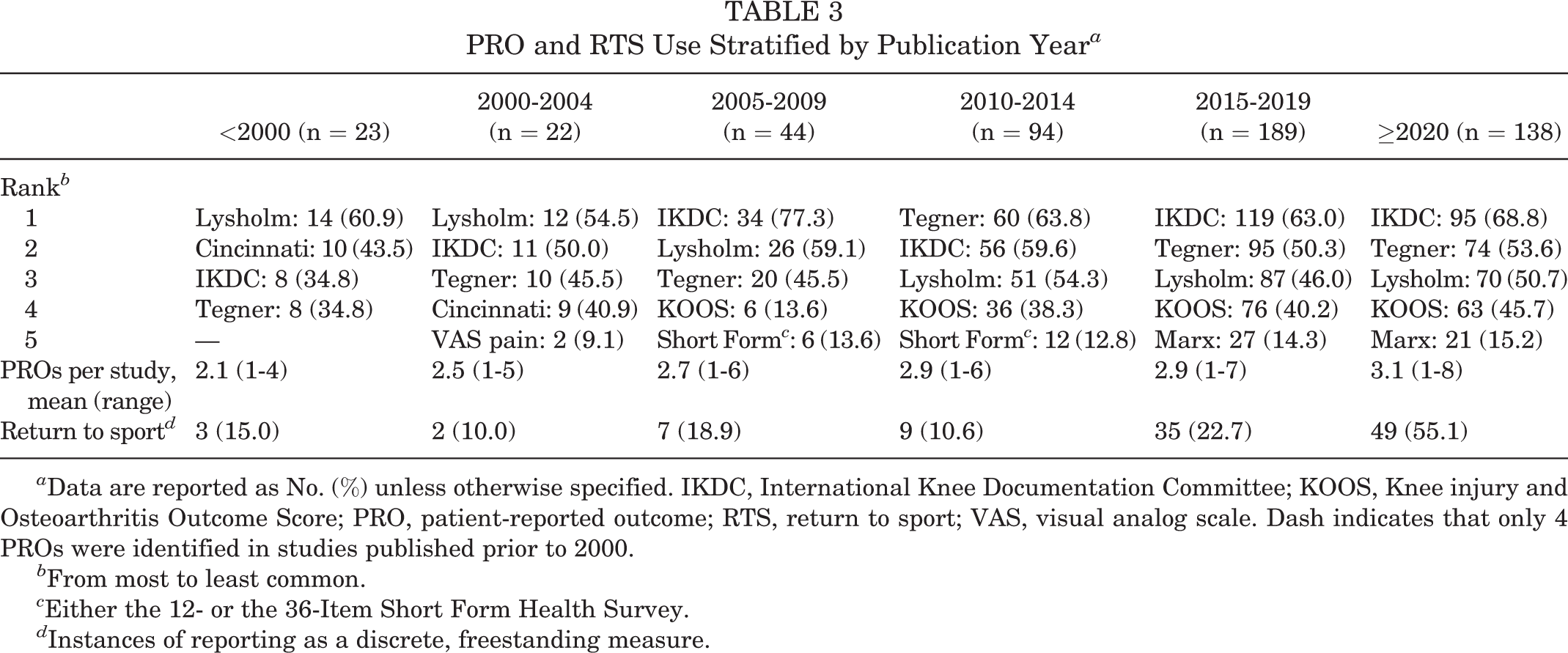
a Data are reported as No. (%) unless otherwise specified. IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; PRO, patient-reported outcome; RTS, return to sport; VAS, visual analog scale. Dash indicates that only 4 PROs were identified in studies published prior to 2000.
b From most to least common.
c Either the 12- or the 36-Item Short Form Health Survey.
d Instances of reporting as a discrete, freestanding measure.
Regarding study design, the number of registry-based and retrospective studies generally increased over time, while the number of prospective cohort studies decreased (Figure 4). The number of prospective randomized controlled trials fluctuated, and the number cross-sectional studies remained steady.

Study designs stratified by publication year. RCT, randomized controlled trial.
Discussion
A comprehensive understanding of the risks, outcomes, and complications associated with any surgical procedure requires the use of standardized methods of evaluation. Although radiographic and objective clinical assessments remain important, the increasingly integral role of subjective PROs in outcome evaluation must be acknowledged. The topic of ACL reconstruction is highly debated, with little consensus among the orthopaedic literature. The significant heterogeneity in outcome measures impedes comparison and stalls the evolution of reconstruction technique.
We hypothesized that there would be significant variability in the PROs within the ACL reconstruction literature and that this trend would become increasingly prevalent over time. Despite limiting studies to those with ≥50 patients and a mean follow-up of 24 months, an overwhelming 72 PROs were identified. The mean number of PROs per study increased over time, confirming their growing importance while clarifying the lack of standardized reporting.
Prior reviews have evaluated outcome measures reported in the ACL literature. 25,31 Unlike our review, these were significantly more confined in terms of the number of journals, number of articles, and time frame analyzed. In their 2001 publication, Johnson and Smith 25 identified 54 unique outcome measures across 4 journals between 1984 and 1997, a small number of which were valid and reliable. Among the 197 articles identified, the Lysholm (42.6%), Tegner (21.3%), Cincinnati/Noyes (15.2%), and IKDC (8.6%) were the most common. In their 2015 review, Makhni et al 31 found significant variability in objective and subjective outcome reporting patterns in 119 studies published between 2010 and 2014 in 4 high-impact orthopaedic journals. Regarding subjective outcomes, the authors documented a total of 16 PROs. Despite more stringent inclusion criteria, the most commonly reported PROs were the same as those in our study—the IKDC, Lysholm, Tegner, and KOOS. A total of 29 studies (24%) cited return to activity or sport, a higher proportion than the 20.6% observed in our study.
The most popular of the PROs, the IKDC score, is a product of a collaboration among international experts affiliated with the AOSSM and European Society for Sports Traumatology, Knee Surgery and Arthroscopy. 2 The IKDC Standard Knee Evaluation Form, designed for knee ligament injuries, was first published in 1993 and revised in 1994. 10,22 The IKDC Subjective Knee Evaluation Form was developed in 1997 as a revision of the Standard Knee Evaluation Form and has undergone several minor revisions and validation across multiple languages since its publication in 2001. 21,24,37 The IKDC Subjective Knee Evaluation Form consists of 18 items across the domains of symptoms (7 items), sports and daily activities (10 items), and function (1 item). Scores range from 0 (low function, highly symptomatic) to 100 (high function, minimally symptomatic). The IKDC Subjective Knee Evaluation Form was initially validated among a group in which the majority of patients were young adult Caucasian athletes. 24 ACL injury was present in 129 of the 533 patients (24.2%). Nonetheless, the IKDC score has been shown to have adequate test-retest reliability, responsiveness, and validity across multiple knee pathologies: an important consideration given that patients undergoing ACL reconstruction often experience a multitude of concomitant injuries.
The second- and third-most utilized PROs in our review were the Lysholm score and Tegner Activity Scale. The Lysholm score was first published in 1982 to evaluate outcomes of knee ligament surgery, specifically symptoms of instability. 30 The Lysholm score measures outcomes across 8 domains: limp, locking, pain, stair climbing, support, instability, swelling, and squatting. The Tegner Activity Scale was developed as a complement to the Lysholm score after it was observed that function scores evaluated by the Lysholm score may be influenced by activity level. 43
To determine the Tegner score, patients are presented with a list of 11 activities, ranging from those of daily living to competitive professional sports. The level of activity (0-10) that best describes the patient’s current level is used to determine the score.
Detailed evaluation of the psychometric parameters in patients with ACL injury has demonstrated acceptable reliability, validity, and responsiveness of the Lysholm and Tegner scales. 7 Furthermore, multiple studies have commented on the lack of floor or ceiling effects, as well as correlation with other PROs, including the IKDC score and 12-Item Short Form Health Survey. 7,8,32,34,38 Regarding the Lysholm score, the high ceiling effects of the support and locking domains and the high floor effect of the squatting domain may limit our ability to discriminate differences in functional status among patients. The development of less invasive reconstruction techniques, the improved rehabilitation protocols, the limitations in preoperative activity, and the use of preoperative rehabilitation provide plausible explanation. 8 The Tegner Activity Scale has been shown to have a large effect size in patients with isolated ACL injury and a moderate effect size in those with concomitant injuries. 8 This should be taken into consideration with the Tegner Activity Scale, especially when comparing outcomes among patients being treated for multiple pathologies.
Perhaps the most important outcome parameter for athletes undergoing ACL reconstruction is the ability to RTS, specifically at preoperative levels. 26,44 Although an ACL-deficient knee can greatly compromise quality of life in nonathletes, there exists additional and important athlete-specific consequences associated with ACL injury. ACL injury in athletes can affect level and style of play, as well as attainment of career progression and career longevity. The sense of purpose and community provided by organized athletics may also be influenced by ACL injury. Despite the importance of RTS, only 20.6% of studies discretely reported this metric. Level of activity is encompassed in several PROs, including the Tegner Activity Scale; however, RTS is a more direct and relatable measure. Even with more studies reporting rates of RTS over time, we suggest further expansion and reporting of this metric given its significance in evaluating the quality of outcomes.
The landscape of ACL reconstruction and the methodology used to assess outcomes have changed considerably over the past 20 years, including the focus on the collection of PROs. Although the IKDC remains the most frequently reported PRO, our findings demonstrated an increase in the relative use of the KOOS, Marx, visual analog scale for pain, and 12- or 36-Item Short Form Health Survey. The KOOS, a newer PRO measure, is an extension of the Western Ontario and McMaster Universities Osteoarthritis Index and has been validated for younger, more active patients, including those with ACL injury. 39 The KOOS is a region-specific outcome measure used to capture the progression of knee-related symptoms from injury to the development of osteoarthritis. The IKDC has been shown to outperform the KOOS in the context of ACL reconstruction, although it is increasingly being used, especially in Europe. 18,42 The rising prevalence of the Marx scale is a reflection of its relative novelty (developed in 2001) and unique ability to evaluate activity exposure in addition to type of actiivty. 42 Postoperative pain contributes significantly to patient-perceived outcomes and is known to delay return to activities of daily living and rehabilitation. 36,48 Furthermore, the reporting patterns of postoperative pain are likely influenced by increased pressure to develop standardized opioid prescription protocols as well as multimodal analgesic pathways. 17,20 The increasing prevalence of the 12- and 36-Item Short Form Health Surveys is reflective of the evolving recognition of the importance of physical, social, and emotional health in those with ACL injury and their influence on patient outcomes. 12
The heterogeneity observed with regard to PROs is not unique to ACL reconstruction. Studies across different specialties, surgical and nonsurgical, have also reported on this phenomenon. 14,16,28,33,45,49 Furthermore, the PROs utilized in the assessment of patients undergoing ACL reconstruction are largely nonspecific to ACL injury itself. Nonetheless, substantial effort has been devoted to the validation of these outcome measures, creating a situation in which evaluation of outcomes is limited by heterogeneity and not availability of suitable metrics. As care delivery models shift away from fee-for-service systems to patient-centric value-based care systems, standardization and unification of outcome reporting become increasingly important. Fee-for-service systems create incentives for interventions over nonsurgical therapy and are thought to lead to billing errors, service inflation, treatment redundancy, and unnecessary testing. 46 Value-based systems such as accountable care organizations, bundled payments, and capitation have all been proposed as alternatives to the traditional fee-for-service model. In an accountable care organization model, patient care is coordinated among hospitals, physicians, and other providers to reduce expenditure and achieve a financial benchmark resulting in shared savings. 29 With bundled payments, total reimbursement for an episode of care is predetermined. 41 Although there is financial risk and liability assumed with bundled payments, this model promotes efficiency, quality, and accountability for acute and postacute care. Similar in nature, capitation models reimburse physicians a set amount per patient per unit time. 13 Regardless of the payer model used, value is frequently quantified using a cost-utility analysis, which defines value as the ratio of cost per improvement of a quality-adjusted life year. 6,11 These analyses almost universally utilize PROs. As such, a unifying measure for determining value after ACL reconstruction should be disease specific and include measures of satisfaction, employment/RTS, pain, and general health. 47
It is our recommendation that outcomes after ACL reconstruction be reported in a manner consistent with the guidelines developed at the ACL Consensus Meeting Panther Symposium 2019. 42 Three of the 9 consensus statements generated at the symposium pertain to PROs: (1) assessment of PROs should optimally include ≥1 knee-specific outcome tool, 1 activity rating scale, and 1 measure of health-related quality of life; (2) the IKDC Subjective Knee Evaluation Form is the recommended knee-related outcome measure for ACL injury and treatment; and (3) measurement of the Patient Acceptable Symptom State is valuable in the assessment of outcome after ACL injury and treatment. 42 Although these guidelines help to standardize reporting, the intrinsic shortcomings of individual PROs, including response burden and cost, need to be addressed and an emerging solution involves using PROs in the National Institutes of Health’s PROMIS program. PROMIS-derived PROs have been rigorously tested and represent a broad spectrum of outcome measures that can be reliably and efficiently obtained from patients, including those with ACL injury. 9,19
Limitations
This review is not without limitation. It should be noted that although this is a large-scale study, it is not exhaustive. Only studies with ≥50 patients and a mean 24-month follow-up were included. This decision was made in an effort to isolate larger, more impactful studies reporting outcomes beyond the acute postoperative period. There are certainly studies with smaller cohorts and shorter follow-up that have greatly influenced our understanding of ACL reconstruction. This study did not take into consideration the objective of each study, which likely influenced the relative selection of PROs. Additionally, this review was limited to studies published in the English language and did not incorporate gray literature. Furthermore, only named outcome metrics were analyzed, thus potentially excluding more informal modes of evaluation. Last, given the reporting bias among the studies, the true spectrum of PROs utilized is likely broader than what this review suggests.
Conclusion
The PROs used to report and evaluate patient outcomes after ACL reconstruction remain heterogeneous and inconsistent. When all 510 studies were examined together, 72 unique PROs were identified, with a mean 2.89 measures per study (range, 1-8). Significant variability was observed, with 89% of measures being reported in <10% of studies. RTS was discretely reported in only 20.6% of studies. Our goal was to survey the current literature on ACL reconstruction to better understand variability in PRO utilization. Our findings confirm the need for standardized reporting of PROs so that more definitive comparisons of postoperative outcomes can be made. Additionally, standardization will generate a more comprehensive understanding of technique-specific benefits and better facilitate value determination.
Footnotes
Final revision submitted January 5, 2023; accepted February 8, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: D.P.P. has received education payments from Peerless Surgical and consulting fees from Zimmer Biomet. J.E.F. has received education payments from Peerless Surgical, nonconsulting fees from Smith & Nephew, and hospitality payments from Arthrex. D.P.T. has received grant support from Arthrex and education payments from Arthrex, Peerless Surgical, and Smith & Nephew. B.M.S. has received grant support from Arthrex; education payments from Arthrex, Peerless Surgical, and Smith & Nephew; and consulting fees from Bioventus. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.