
Abstract
Background:
Athletes display persistent muscle deficits and altered limb-loading mechanics at the time of return to sport (RTS) after anterior cruciate ligament reconstruction (ACLR).
Purpose:
To compare an objective profile of adolescent athletes at RTS after ACLR to matched healthy controls.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
Included were 124 participants; 62 patients who underwent ACLR (15.4 ± 1.7 years) and 62 healthy controls (15.3 ± 1.7 years). Motion capture and force plates were used to capture joint motions during jump landing (JL) and single-limb squat (SLS) tasks. Energy absorption contribution (EAC) was calculated, and repeated-measures analysis of variance was used to assess for EAC differences between groups. Participants completed an International Knee Documentation Committee (IKDC) Subjective Knee Form, and isokinetic quadriceps and hamstring strength testing was performed on each limb. Independent t tests were run to examine age, height, weight, and IKDC scores as well as compare differences between groups for quadriceps and hamstring strength.
Results:
A significant group × joint interaction was found for JL (P < .001) and SLS (P < .001). For JL, patients who underwent ACLR utilized significantly greater hip (P < .001) and significantly less knee (P < .001) EAC on the surgical limb compared with controls. During SLS, patients who underwent ACLR utilized significantly greater hip (P < .001) and significantly less knee (P < .001) EAC on the surgical limb compared with controls. The ACLR cohort demonstrated lower IKDC scores (P < .001) and significantly lower quadriceps strength on the surgical limb (P < .001) than controls. There were no differences in surgical limb hamstring strength between the ACLR cohort and healthy controls (P = .701).
Conclusion:
Compared with matched healthy controls, the participants who underwent ACLR in this study demonstrated an inferior objective profile at RTS, consisting of deficits in surgical limb loading, self-reported outcomes, and strength.
Keywords
The timing of return to sport (RTS) after anterior cruciate ligament reconstruction (ACLR) involves a complex, multifactorial decision-making process and is often challenging for clinicians. Patient expectations for RTS are high, as 91% expect to return to their preinjury level of sport 8 ; however, contrary to this perception, RTS rates for competitive sports are relatively low, reporting at 55% at 1 year and approximately 65% at 2 years. 1,31 These findings may be related to multiple factors, including persistent deficits in muscle strength, 28 athletic performance/level, 21 and altered limb-loading strategies during squatting, 10,22 jumping, and landing activities. 4,6,12,26,27 Many of these alterations in lower extremity characteristics and compensatory strategies are frequently not identified until after patients return to high-level activity. 30
Considering these suboptimal outcomes, RTS decision-making has recently been scrutinized, with an emphasis on the use of objective measures regarding strength and functional status in addition to utilizing traditional time-based recommendations. Objective parameters, including strength assessment and performance-based functional testing (eg, double- or single-limb squat, hop tests), patient-reported outcomes, and psychological factors have all documented evidence regarding their impact on RTS.
Alterations in joint loading at the time of RTS after ACLR have been previously studied. Decreased knee extension moments and smaller knee flexion and hip adduction angles are present during the single-limb squat (SLS) in patients who have undergone ACLR when compared with healthy controls at approximately 7 months postoperatively. 3 Likewise, when 24 patients were tested between 3 and 6 months post-ACLR, the surgical limb exhibited lower vertical ground-reaction force, decreased energy absorption, and deficits in external knee extension moments compared with the nonsurgical limb during a drop jump landing (JL) task. 20
Energy absorption has previously been described as a means of using both kinematic and kinetic data to estimate lower extremity muscle activity–producing movements throughout the entire landing activity. 23,24 This can be further extrapolated to calculate the contribution of each specific joint to the overall energy expenditure across the kinetic chain during an athletic movement. The use of energy absorption contribution (EAC) to examine joint loading allows for investigation of intralimb load sharing between the different joints (hip, knee, ankle) during dynamic tasks and, as such, may provide greater depth of knowledge into the compensatory patterns on the surgical limb. While previous studies 9,10 have described surgical limb joint loading through the use of EAC in the early stages of rehabilitation (3-6 months), there is little information regarding EAC during double- and single-limb activities at the time of RTS.
To our knowledge, no study has created a singular objective profile for the young athlete after ACLR at RTS with regard to parameters of strength, lower extremity loading assessment, and patient-reported outcomes. We therefore compiled a profile that includes isokinetic quadriceps and hamstring strength; hip, knee, and ankle EAC in SLS and during double-limb JL; and International Knee Documentation Committee (IKDC) scores. The purpose of this study was to compare the objective profile of postoperative adolescent athletes at RTS after ACLR to age- and activity-matched healthy controls. We hypothesized that at the time of RTS, adolescent athletes would demonstrate the following characteristics: (1) diminished quadriceps strength; (2) increased hip, decreased knee, and similar ankle EAC during an SLS; (3) increased hip, decreased knee, and decreased ankle EAC during a drop JL; and (4) deficits in IKDC scores when compared with age- and activity-matched healthy controls.
Methods
Participants
A total of 124 participants who met inclusion criteria were enrolled in the study between August 20, 2015, and September 17, 2018; included were 62 patients who underwent ACLR and 62 healthy age-, sex-, height-, weight-, and limb-matched controls. All participants were screened before enrollment by the study staff to assess inclusion eligibility. For both groups, participants were considered for the study if they were between the ages of 13 and 18 years and if they were involved in a level 1 sport (eg, basketball, football, or soccer). For this study, no participants older than 18 years were included
After study enrollment, each participant completed an IKDC questionnaire and a demographic information sheet that included injury history and sports participation. Participants who underwent ACLR received either a bone–patellar tendon–bone (BTB) autograft or hamstring autograft per the operating surgeon’s discretion. All participants who underwent ACLR were tested at the time of RTS as part of a larger ongoing study examining clinical outcomes across the continuum of care. On average, RTS testing was performed at 6.9 months after surgery. RTS progression was granted to postoperative patients who underwent ACLR once patients had met a number of biometric and functional testing parameters in collaboration with the patient’s orthopaedic surgeon and sports physical therapist, as well as objective information obtained from the Lower Extremity Assessment and Performance (LEAP) laboratory testing. For further details on the RTS criteria, see Appendix A (available as supplemental material). The healthy group was tested at a single point in time as part of a separate ongoing study examining movement profiles of healthy athletes. Both groups completed the same testing protocol. Each participant in the ACLR group followed a standardized rehabilitation program that was developed collaboratively by the orthopaedic surgeons and the sports physical therapists at the institution in which the study was occurring. For additional details on the rehabilitation protocol, see Appendix B (available as supplemental material).
Testing
An 8-camera Motion Capture System (Qualisys AB) with a sampling rate of 120 Hz was used to capture joint motions in all 3 planes during the double-limb JL and SLS tasks. Thirty-three reflective markers were adhered to each participant’s skin/clothing with double-sided tape. Two force plates capturing at 1200 Hz (Advanced Mechanical Technology Inc) were used to obtain joint kinetics and to allow accurate time sequencing during data collection and data processing.
Double-Limb JL Task
Each participant completed 3 trials of a JL task. The trial began with the participant standing on top of a box that was placed at a distance of 50% of their height from the force plate. The JL task consisted of 2 double-leg jumps: 1 jump forward off a 30-cm box onto both legs, and then immediately into a vertical jump for maximal height (Figure 1).

Double-limb jump landing maneuver.
Single-Limb Squat Task
Each participant was asked to stand with feet shoulder width apart with their hands on their waist, with 1 foot on each force plate. Participants were then asked to lift the nontesting limb to 90° of hip and knee flexion and were instructed to perform an SLS as if they were sitting down onto a chair to a self-selected depth. A metronome set at 60 bpm was used to ensure consistent pace across testing as participants completed 5 SLSs. If participants experienced a loss of balance or loss of position during the 5 consecutive squats, then the test was repeated until they could complete 5 consecutive SLSs.
Isokinetic Testing
The Biodex Multi-Joint Testing and Rehabilitation System (Biodex Medical Systems) was used for testing knee extensor and flexor peak torque. For this study, knee extensor peak torque will be referred to throughout the paper as quadriceps strength and knee flexor peak torque as hamstring strength. Participants were seated on the Biodex system and secured with padded straps around the thigh, pelvis, and torso to minimize accessory and compensatory movements during testing. 7,16 The test limb femoral condyle was aligned with the Biodex axis of rotation as per the manufacturer’s instructions. Participants performed 5 submaximal knee extension/flexion repetitions to familiarize themselves with the testing motion. To measure quadriceps strength at 60 deg/s, participants performed 5 consecutive concentric contractions. 5 The same protocol was applied when testing hamstring strength. All participants began testing on their nonsurgical limb followed by the surgical limb, and the average of the 5 trials for each limb was normalized to body weight (BW) and used for data analysis.
Statistical Analysis
All data analyses were performed using SPSS version 25 (IBM Corp). To compare the characteristics of the participants between the 2 groups, independent t tests were used to examine age, height, weight, and IKDC scores, and chi-square tests were used to examine sex and limb dominance. Before statistical analyses, all kinetic data were assessed for normality and outliers. To assess our first aim (to examine differences during JL in surgical and nonsurgical hip, knee, and ankle EAC between the ACLR and healthy groups), a 2 (group) × 3 (joint) repeated-measures analysis of variance (ANOVA) was used to assess for differences between and within groups, with the α level set at 0.05. If there was a significant interaction, post hoc pairwise comparisons were performed. To address our second aim (to examine differences during an SLS in surgical and nonsurgical hip, knee, and ankle EAC between the ACLR and healthy groups), a 2 (group) × 3 (joint) repeated-measures ANOVA was used to assess for differences between and within groups, with the α level set at 0.05. If there was a significant interaction, post hoc pairwise comparisons were performed. While the matching of cases and controls did add an additional level of dependency within the data, this was not incorporated into the analyses. Finally, to compare differences between groups for quadriceps and hamstring peak force between the surgical and nonsurgical limbs, independent t tests were run with the alpha level set at 0.05.
Results
Characteristics and IKDC Scores
Table 1 displays the characteristics of the participants for both groups. Of the 62 patients who underwent ACLR, 92% received a BTB autograft, while 8% received a hamstring autograft.
Characteristics of Participants for Each Group a

a Data are reported as mean ± SD or absolute values. Bolded P value indicates a statistically significant difference between groups (P < .05). ACLR, anterior cruciate ligament reconstruction; IKDC, International Knee Documentation Committee; NA, not applicable.
Jump Landing
There was a significant group × joint interaction (F(1.50, 177.6) = 54.92; P < .001). Post hoc tests revealed that the ACLR cohort demonstrated significantly greater surgical limb hip EAC (ACLR = 52.1% ± 21.3%, healthy = 20.4% ± 10.9%; P < .001) and significantly less surgical limb knee EAC (ACLR = 28.1% ± 23.1%, healthy = 60.6% ± 10.75%; P < .001) (Table 2). On the nonsurgical limb, there were also significant group differences at the hip (ACLR = 40.3% ± 20.9%, healthy = 52.9% ± 11.3%; P < .001), knee (ACLR = 37.8% ± 25.1%, healthy = 18.6% ± 13.5%; P < .001), and ankle (ACLR = 21.7% ± 7.7%, healthy = 28.4% ± 10.0%; P < .001).
Between-Group Differences in EAC During Jump Landing a

a Data are reported as mean ± SD (in percent). Bolded P values indicate a statistically significant difference (P < .05). ACLR, anterior cruciate ligament reconstruction.
Single-Limb Squat
There was a significant group × joint interaction (F(2.39, 181.9) = 17.53; P < .001). Post hoc tests revealed that the ACLR cohort demonstrated significantly greater surgical limb hip EAC (ACLR = 39.2% ± 11.1%, healthy = 24.5% ± 8.7%; P < .001) and significantly less surgical limb knee EAC (ACLR = 45.1% ± 9.9%, healthy = 57.4% ± 7.5%; P < .001) (Table 3). There were also significant differences between groups for nonsurgical limb ankle EAC (ACLR = 16.2% ± 4.9%, healthy = 18.9% ± 5.1%; P = .030).
Between-Group Differences in EAC During Single-Limb Squat a

a Data are reported as mean ± SD (in percent). Bolded P values indicate a statistically significant difference (P < .05). ACLR, anterior cruciate ligament reconstruction.
Quadriceps and Hamstring Strength
For quadriceps strength, the ACLR group demonstrated significantly lower surgical limb values (ACLR = 1.49 ± 0.43 BW, healthy = 1.97 ± 0.48 BW; P < .001) (Table 4). The hamstring strength of patients who underwent ACLR was significantly greater compared with controls on the nonsurgical limb (ACLR = 1.06 ± 0.28 BW, healthy = .945 ± 0.24 BW; P < .001).
Between-Group Differences in Quadriceps and Hamstring Isokinetic Strength a
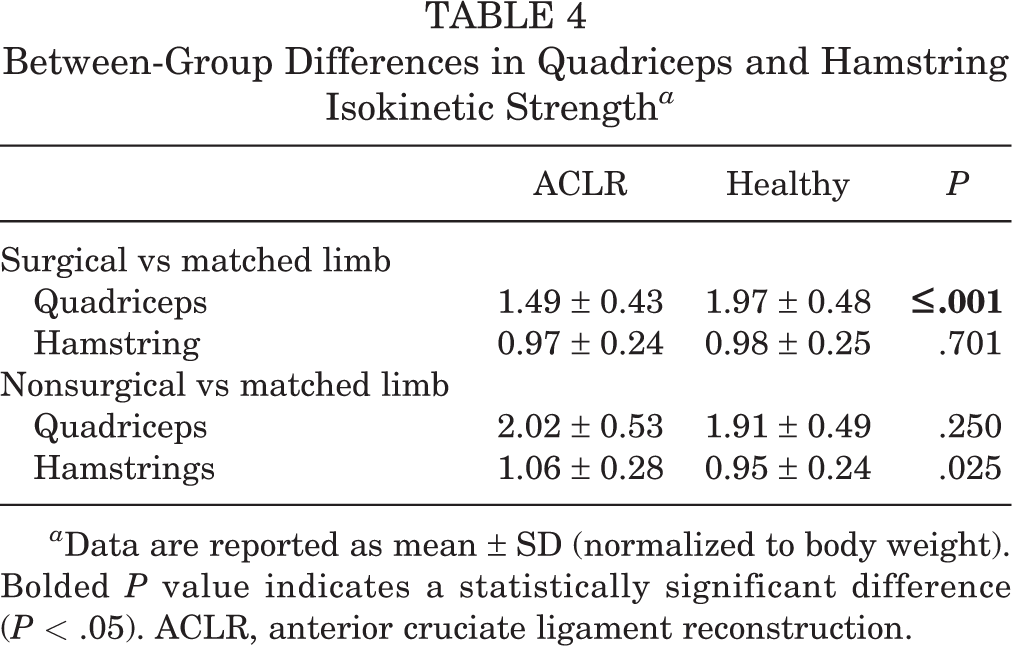
a Data are reported as mean ± SD (normalized to body weight). Bolded P value indicates a statistically significant difference (P < .05). ACLR, anterior cruciate ligament reconstruction.
Discussion
The findings of the current study are in line with our original hypotheses that participants at the time of return to sport (RTS) after ACLR would demonstrate alterations in surgical limb loading, and deficits in quadriceps strength values and self-reported measures of function when compared with matched healthy controls. Participants who had undergone ACLR demonstrated an increase in hip loading with a subsequent decrease in loading at the knee on the surgical limb compared with healthy controls during both the jump-landing (JL) and single-limb squat (SLS) tasks. These findings were in conjunction with lower surgical limb quadriceps strength values and IKDC scores after ACLR. Together, these data support the hypotheses of an inferior objective profile of adolescent athletes after ACLR at RTS in comparison to a healthy cohort.
Regarding energy absorption contribution (EAC) measured in our study, the surgical limb in patients who underwent ACLR demonstrated increased hip and decreased knee EAC during both SLS and JL tasks when compared with matched healthy individuals. Surgical limb knee EAC changes across the continuum of care in patients who have undergone ACLR, as there is a large increase in knee EAC from 12 weeks postoperatively to the time of RTS during a double-limb squat. 10 These findings highlight the importance of the last few months of rehabilitation in terms of progressive loading in conjunction with quadriceps strengthening for improving neuromuscular control of the knee joint. Likewise, earlier work from Garrison et al 9 demonstrated that at 12 weeks after ACLR, the surgical limb shifts loading demands from the knee to the hip in an effort to perform a functional squat. This abnormal pattern of load sharing (or abnormality) between the hip and knee continues to be prevalent in the double-limb squat at RTS, although discrepancies improve when compared with 12 weeks. 10 Similarly, after ACLR participants in the current study continued to demonstrate consistently diminished knee EAC in the surgical limb at the time of RTS with more demanding maneuvers, which may be explained by a lack of quadriceps strength as well as continued neuromuscular control deficits of the extremity. These findings may not be transferable to other populations or other dynamic tasks, but they do represent the continuation of the inability to load the surgical knee during a submaximal task such as a SLS. Something as simple as monitoring an athlete’s limb-loading pattern during a single-limb squat may provide clinical insight into an athlete’s strength and neuromuscular control of the postoperative extremity.
Conversely, during the SLS, the nonsurgical limb in the ACLR group was found to have similar hip and knee EAC but decreased ankle EAC when compared with the control group. During the JL, the nonsurgical limb utilized a strategy that included decreased hip, increased knee, and decreased ankle EAC. The differences in limb EAC during the JL across the matched nonsurgical limbs of the cohorts may illustrate variable intralimb compensation strategies depending on limb dominance. Likewise, because the task (JL) requires both limbs to absorb forces during landing, the nonsurgical/matched limb of both groups is essentially forced to compensate for alterations that might occur on the contralateral limb. For instance, in the surgical limb of the ACLR cohort, there was an increase in contribution at the hip (∼52%) and decrease at the knee (∼28%), while the nonsurgical limb demonstrated a slightly lower contribution at the hip (∼40%) with a higher contribution at the knee (∼38%) during the landing maneuver. Clinicians should recognize inherent “unseen” asymmetries and consider the intralimb and between-limb motor pattern alterations that may be used to achieve symmetry during a double-limb task. Additionally, the JL task may provide sufficient stimulus to identify deficits in nonsurgical limb loading, while the SLS task does not. Future research warrants further investigation into changes in limb EAC during dynamic tasks depending on limb dominance in both healthy and ACLR athletes.
Similar to previous findings in the literature, quadriceps strength deficits continued to persist at the time of RTS in the surgical limb (1.49 ± 0.43 BW) when compared with controls (1.97 ± 0.48 BW). 4,10,25,33 Additionally, there was a substantial interlimb difference in quadriceps strength between the surgical and nonsurgical limbs in the patients who underwent ACLR. The limb symmetry index was found to be 73.7% for quadriceps strength in patients who underwent ACLR. This is similar to previous findings of 25% and 30% quadriceps strength deficits depending on whether or not the patient was able to return to preinjury level of sport after ACLR. 25 Quadriceps strength deficits have also been associated with muscle atrophy throughout the postoperative period, with changes occurring from as early as 12 weeks 7,34 to as long as 5 years postoperatively. 15,17 In the current study, quadriceps strength deficits may have been directly linked to graft choice in our ACLR cohort, as the majority of patients (92%) received BTB autografts. In contrast, the hamstring strength of patients who underwent ACLR was not significantly different on the surgical limb when compared with the matched limb of the control group, although interestingly, it was significantly greater than that of the control group on the nonsurgical limb. The relative improvement in nonsurgical limb hamstring strength may be accredited to the postoperative strength rehabilitation program, which emphasizes hamstring strength training, although this small difference may not be clinically significant.
Although the focus of lower extremity strengthening in ACL rehabilitation seems to be centered on regaining quadriceps strength, much data support the use of muscle cocontraction to minimize dynamic knee valgus and knee abduction. Deficits in hamstring strength may ultimately diminish cocontraction about the knee and increase ligamentous stresses (ie, ACL shear stress) with the resulting dynamic instability. 13 Our patients were found to have adequate hamstring strength in both extremities, indicating that hamstring strength may not be a limiting factor for allowing adequate cocontraction of the knee joint, theoretically limiting shear forces on the ACL. Unfortunately, the persistent quadriceps strength deficit may lead to intralimb compensations and contribute to altered EAC patterns across the kinetic chain. Schmitt et al 30 previously demonstrated that increasing isokinetic quadriceps strength during the rehabilitation process leads to improvements in JL mechanics. Likewise, improvements in quadriceps and hamstring strength are associated with better patient-reported outcomes.
Scherer et al 29 found that individuals who had undergone ACLR displaying deficits of knee flexion or extension strength of greater than 20% scored significantly lower on the Knee injury and Osteoarthritis Outcome Score. It has also frequently been shown that athletes who RTS after ACLR had higher average IKDC scores than those who did not. 18,25 In comparison, our athletes had findings consistently lower than their matched controls (90.2 vs 99.4), but on par with the numbers found in the previous studies for those that were able to RTS. Pediatric and adolescent athletes also demonstrate improved IKDC scores when compared with young adults undergoing ACLR. 14 This may have contributed to our relatively improved IKDC numbers compared with those found by Novaretti et al, 25 who had a slightly older patient population. This demonstrates that even for high-performing adolescents at RTS, these athletes continue to display diminished patient-reported knee function when compared with their healthy peers.
In a recent meta-analysis, 31 only 23% of young patients passed the battery of RTS tests. This extraordinary low-pass-rate number for RTS, along with an equally perplexing high reinjury rate—especially in young athletes, suggests the potential for deliberate flaws in our RTS criteria. 32 Specifically, there is a lack of evidence supporting the use of these tests to increase a safe return of injured athletes back to sports and a lack of test components that challenge functional ability in planes other than the sagittal plane. 11 Thus, in order to continue to make advancements in reinjury risk reduction after ACLR, alterations and adaptations of current RTS testing should be challenged. 2,32,33
Continuing to utilize a cluster of RTS tests, including a variety of limb strength measures, analysis of frontal and sagittal plane biomechanics, joint range of motion, and patient-reported outcome measures such as the IKDC Subjective Knee Form, may provide the clinician with a better understanding of a patient’s readiness to RTS. The comparison of surgical limb objective data with the established values depicted in this study may provide more valuable insight into the preparedness of a young individual to RTS after ACLR. In addition to the use of the battery of RTS tests, comparing our average IKDC, strength, and EAC limb compensation patterns for JL or SLS to a comparable patient’s findings may give physical therapists and orthopaedic surgeons additional guidance in determining appropriate time for RTS for their athletes and patients.
Limitations
Although our patients passed our protocol for RTS progression, these patients will likely continue to improve throughout the postoperative course beyond 6 months. There may subsequently be improvements in quadriceps strength values and potential changes in EAC findings and intra- or interlimb compensation mechanisms over time. This may ultimately diminish the generalizability of these findings, especially in patients who are counseled to RTS later in their postoperative course. We hope to further evaluate and compare these findings in the 1- to 2-year postoperative time period after these patients have returned to high-level activity.
The majority of the patients in the current study underwent a patellar tendon autograft, which may have played a role in quadriceps strength values. Similarly, use of an autograft for ACLR has been previously identified as a risk factor for postoperative knee stiffness in the literature, 19 which could ultimately contribute to quadriceps strength deficits. Concomitantly, we did not document knee range of motion in this study or other clinical examination parameters such as the Lachman and pivot-shift maneuvers. However, in this patient population, we have found knee extension deficits to be rare.
Conclusion
The results of this study indicate that participants who underwent ACLR demonstrate an inferior objective profile consisting of deficits in surgical limb loading, self-reported outcomes, and strength compared with healthy controls at RTS. These changes in limb-loading mechanics are likely associated with quadriceps strength deficits that continue to be present at the time of RTS after ACLR. In addition, altered neuromuscular control patterns persist through the time when most athletes are allowed to RTS; as such, these biomechanical changes may increase stress on the reconstructed ACL graft and ultimately place these athletes at risk of a subsequent injury.
Supplemental material for this article is available at http://journals.sagepub.com/doi/suppl/10.1177/23259671211063576.
Supplemental Material
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671211063576 - Adolescent Athletes Demonstrate Inferior Objective Profiles at the Time of Return to Sport After ACLR Compared With Healthy Controls
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671211063576 for Adolescent Athletes Demonstrate Inferior Objective Profiles at the Time of Return to Sport After ACLR Compared With Healthy Controls by John D. Robinson, Joseph Hannon, Shiho Goto, Steven B. Singleton and J. Craig Garrison in Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted July 11, 2021; accepted August 24, 2021.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.B.S. has received education payments from Pylant Medical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Texas Health Resources.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.