
Abstract
Background:
There is no clear consensus as to which intervention to prioritize for midportion Achilles tendinopathy (AT), although recent clinical practice guidelines have recommended eccentric exercises.
Purpose/Hypothesis:
The purpose of this study was to (1) compare exercise loading protocols with passive treatment modalities for the management of midportion AT and (2) compare different exercise loading protocols. We hypothesized that loading exercises would be associated with a greater decrease in pain and symptoms compared with passive treatment modalities but that no loading protocols would be associated with improved results.
Study Design:
Systematic review; Level of evidence, 1.
Methods:
Following the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines, we searched the MEDLINE, EMBASE, CINHAL, and Web of Science databases for randomized controlled trials (RCTs) and compared eccentric loading protocols with passive treatment modalities or different eccentric loading protocols as an intervention for midportion AT. A total of 5126 articles were identified after the initial search. After selection, the risk of bias (RoB) and the Grading of Recommendations, Assessment, Development and Evaluation approach were applied to pooled studies for quantitative analysis. The outcomes of interest were pain and function, which were measured using the visual analog scale and the Victorian Institute of Sport Assessment–Achilles scale. Mean differences (MDs) and 95% CIs were calculated using random effects (significant heterogeneity) or fixed effects (nonsignificant heterogeneity) inverse variance models.
Results:
In this study, 12 RCTs (N = 543 participants) were included, of which 2 had a high RoB and 10 showed some concerns of bias. Passive interventions resulted in greater pain reduction in the short term compared with eccentric loading protocols (n = 4 studies; n = 212 participants; pooled MD, 10.22 [95% CI, 2.18 to 18.25]; P = .01). For function, there was a nonsignificant trend in favor of eccentric loading in the short- (n = 3 studies; n = 144 participants; pooled MD, –7.91 [95% CI, –16 to 0.19]; P = .06) and midterm follow-up (n = 5 studies; n = 258 participants; pooled MD, –6.78 [95% CI, –14.23 to 0.68]; P = .07). Meta-analyses of RCTs comparing different types of exercise loading protocols showed no significant differences in the short, mid-, and long term with regard to pain and function.
Conclusion:
Our meta-analyses did not highlight the superiority of one treatment over another for midportion AT.
Achilles tendinopathy (AT) is a common lower limb pathology that accounts for 10% of lower extremity pathologies. 16 It is characterized by local pain, morning stiffness, and reduced function. 12 AT can occur at 2 different locations in the Achilles tendon—at the calcaneal insertion or at its midportion, where the tendon cross-sectional area is smaller. 27 While insertional AT represents only 25% of AT diagnoses and generally affects older or less active people, midportion AT accounts for 60% to 75% of diagnoses and is more common in an active population, such as long-distance runners. 11,30 Persistent symptoms related to midportion AT may interfere with the patient’s ability to exercise and work, which can affect their quality of life. 12,13
Although numerous interventions, such as loading exercises, 3,14,19,34,44,45 activity modification, 41 extracorporeal shockwave therapy (ESWT), 48 corticosteroid injections, 8,9 platelet-rich plasma (PRP), 29 or surgery, 26 are available for the management of midportion AT, nearly 25% still report significant symptoms after the intervention. 2 There is currently no consensus about which conservative intervention to prioritize for the management of midportion AT. 33,36,40,50 A recently published clinical practice guideline recommended with high levels of evidence the inclusion of mechanical loading, which can be either in the form of eccentric or a heavy-load, slow-speed (concentric/eccentric) exercise program. 32 Exercise loading is a low-cost and noninvasive intervention that is easy to perform. Previous studies showed that eccentric exercises lead to significant pain reduction and function improvement in patients with midportion AT. 23,43,52 There are no recent reviews comparing the effectiveness of an exercise loading protocol to so-called passive modalities, nor are there reviews comparing different loading protocols among themselves.
The first aim of this systematic review with meta-analyses was to compare exercise loading protocols with passive treatment modalities on pain and function for the management of midportion AT. The second aim was to compare different loading protocols on the same outcomes. We hypothesized that loading exercises would be associated with a greater decrease in pain and increase in function in the mid- and long term compared with passive modalities because active loading may induce positive physiological adaptations within the tendon, leading to an increased load tolerance. 35 We also hypothesized that different loading protocols would lead to similar results since previous literature could not conclude on an optimal exercise protocol for AT. 31
Methods
We followed the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) 4 recommendations when reporting this prospectively registered systematic review (PROSPERO database identifier: CRD42022330901). The Cochrane Handbook was also used to guide the realization of this systematic review. 20 No protocol was published for this review.
Literature Search and Study Identification
Under the supervision of a research librarian, the following databases were searched from their inception to April 26, 2022: MEDLINE (via Ovid); Cumulative Index to Nursing and Allied Health Literature (via EBSCO CINAHL); EMBASE; and Web of Science. The Medical Subject Headings (MeSH) and keywords were as follows: (1) the painful area (Achilles or calcaneal) and the intervention (isometric or isotonic or eccentric or “high-volume injection*” or PRP or loading or “Hyaluronic acid” or Rehabilitation or “physical therap*” or “Resistance Training” or strengthen* or Rest* or Stretching or Surger* or “Platelet-rich Plasma” or Glucocorticoid* or tap* or “Acupuncture” or “Shockwave Therap*” or “ultrasound therap*” or Pharmaceutical* or Drug* or Pharmacolog* or Cryotherap* or “Cold Therap*” or exercise* or physiotherapy or pharmacology or “manual therap*” or operation or treatment* or “heavy slow resistance”); and (2) the outcome measures (visual analog scale or VAS or numeric pain rating scale or NPRS* or “Victorian Institute of Sport Assessment-Achilles” or VISA-A). Each search strategy was adjusted to the specific database. Complete searches, MeSH, and keywords are available separately (Supplemental Table S1). References from relevant studies, systematic reviews, and included studies were screened for additional potential trials.
Study Selection
The studies were selected using Covidence software (Veritas Health Innovation Ltd company, Melbourne, Australia). After removing duplicates, 2 authors (out of M.-O.D., R.M., F.P., A.T.) independently screened each title and abstract. All relevant full-text articles were then obtained and screened to determine whether they met the inclusion criteria. Disagreements were resolved by discussion with a third reviewer (J.-S.R.). The inclusion criteria were as follows: (1) midportion AT; (2) loading exercises as one of the interventions compared with passive treatment modalities or another loading protocol; (3) randomized controlled trials (RCTs); (4) visual analog scale (VAS)/Numerical Pain Rating Scale (NPRS) and/or the Victorian Institute of Sport Assessment–Achilles (VISA-A) as an outcome measure; and (5) written in English, French, or German. Exercise loading protocols could be compared with any other intervention (eg, acupuncture, massage, surgery, exercises, in-shoe heel lift, ESWT, PRP, ultrasound) as long as those interventions were not combined with loading exercises. The minimal follow-up length was 1 week after the start of the intervention since we were not comparing the immediate effect of interventions.
Outcomes of Interest
The outcomes of interest were pain and function, which were assessed by the VAS, NPRS, and VISA-A scales, respectively. The VAS and NPRS are pain rating scales that provide a range of scores from 0 to 100, where 0 represents no pain and 100 represents the worst pain imaginable. 21 There are currently no minimal clinically important difference (MCID) values for its use in a midportion AT population. The VISA-A score quantifies pain and activity level and can range from 0 to 100, with a score of 100 indicating no pain with full activity level and a score of 0 indicating severely limited activity levels and severe levels of pain. The MCID for the VISA-A score is 14 points. 25 Outcome assessments were performed at the following time points: short (<12 weeks), mid- (12 weeks to 6 months), and long term (>6 months). 20,50
Methodological Quality Assessment
The risk of bias (RoB) of included studies was assessed by 2 reviewers (M.-O.D., R.M.) using the 5 criteria of the Cochrane RoB tool 20 : (1) RoB arising from the randomization process; (2a) RoB due to deviations from the intended interventions; (2b) RoB due to deviations from the intended interventions; (3) RoB due to missing outcome data; (4) RoB in the measurement of the outcome; and (5) RoB in the selection of the reported result. Each criterion has its own algorithm to assess the quality, and the result is reported as low risk, with some concerns, or high RoB. Major flaws included but were not restricted to major conflicts of interest of authors, major methodological shortcomings, or inadequate funding bodies. A study was considered to be at low RoB if all domains were at “low RoB.” A study was considered to have some concerns of bias if ≥1 domain showed “some concerns of bias” but none were at “high RoB.” A study was considered to be at high RoB if a minimum 4 of 6 items of the RoB tool were deemed as “some concerns” or if a major flaw was detected (“high RoB” in ≥1 domain).
All authors first met for a calibration review, where they independently reviewed 2 articles and then discussed each item to clarify the meaning and interpretation of critical appraisal items. Then, the raters independently evaluated an assigned subset of articles. A consensus meeting was held to produce a consensus statement on each rated criterion of every included study. The Gwet AC2 coefficient (quadratic weights) was used to evaluate the consensus agreement on the Cochrane RoB tool between reviewers. 53
GRADE Evaluation
The overall quality of the summarized evidence was evaluated by 2 independent reviewers (M.-O.D., R.M.) using the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach, as recommended by Cochrane 20 :
High quality: Further research is very unlikely to change our confidence in the estimate of effect. Consistent findings among 75% of pooled participants in RCTs with low RoB are generalizable to the population in question. Sufficient data, with narrow confidence intervals, are available. No reporting biases are known or suspected (all domains are met).
Moderate quality: Further research is likely to have an important impact on our confidence in the estimate of effect and may change the estimate (1 domain is not met).
Low quality: Further research is very likely to have an important impact on our confidence in the estimate of effect and is likely to change the estimate (2 domains are not met).
Very low quality: We are very uncertain about the estimate (3 domains are not met).
Domains that may decrease the quality of the evidence include study limitations, consistency of effect, imprecision, indirectness, and reporting biases. We defined high-quality evidence as reported by RCTs with low RoB that provided consistent, direct, and precise results for the outcome. The quality of evidence was reduced by 1 level for each domain not met.
Data Extraction
The first reviewer (R.M.) extracted the data. Two other reviewers (A.T., F.P.) then corroborated or completed the extraction if data were found to be missing. Data were extracted for participants’ characteristics (number of patients per arm, sex/gender, duration of symptoms, and age), characteristics of interventions (duration, frequency, and type of treatment), and outcomes of the interventions for the variables of interest (VAS and VISA-A). Authors of the included RCTs were contacted for additional unpublished data when needed. When encountering missing data, we also used an online software (WebPlotDigitizer) to pick up the data from graphics and we used statistical methods to extract outcomes. The timing of the intervention used in each study about the duration of symptoms was also documented as acute (<3 weeks), subacute (3 weeks to 3 months), and chronic (>3 months).
Data Analysis
Descriptive statistics were used to describe intervention groups, outcomes, and adverse effects. Mean differences (MDs) with 95% CIs were calculated for continuous data outcomes. When data were not extractable and authors could not be contacted, the statistical significance reported in the original study was used.
Heterogeneity Assessment
Studies were assessed for heterogeneity in preparation for the meta-analyses by considering specific clinical features (population, intervention, comparison, and outcome). Review Manager 5.4 software (Cochrane) was used to perform the meta-analyses. Statistical heterogeneity was evaluated by the χ2 test for trend (P > .10; I 2 < 40%). Results were calculated as pooled MD using a random model effect for meta-analyses displaying a statistically significant heterogeneity while a fixed effect was used for those that did not. 20
Results
Literature Search and Study Selection
The search flow diagram is presented in Figure 1. The literature search revealed a total of 5126 citations. After removing duplicates, the titles and abstracts of 3142 studies were screened and 52 papers were retained for full-text review. During the full-text review, 40 studies were excluded for the following reasons: 20 articles used the wrong comparator; 9 were conference proceedings; 5 were not RCTs; 4 had the wrong patient population (insertional AT); and 2 used the wrong outcome measures (tendon stiffness and range of motion). Thus, 12 RCTs ¶ (N = 543 participants) were included in the systematic review and 10 RCTs 1,5,6,10,19,22,37 –39,55 (n = 486 participants) in the meta-analyses.

PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flowchart of study selection.
Characteristics of the Included Studies
The characteristics of included studies and their participants are presented in Table 1. The population in the included trials were adults aged 18 to 75 years, with either subacute (<3 months; 2 studies 54,55 ) or chronic (≥3 months; 10 studies 1,5,6,10,19,22,37-39,47 ) symptoms. Nine RCTs compared an eccentric loading protocol with a passive treatment modality and 3 RCTs compared different loading protocols. Passive interventions included ultrasound, PRP, ESWT, acupuncture, prolotherapy, radiofrequency microtenotomy, passive stretching combined with dietary supplements containing mucopolysaccharides, type I collagen, and vitamin C (PS + MCVC), and protective modalities such as the AirHeel brace and the in-shoe heel lift. Eleven studies used the Alfredson et al 3 protocol (180 daily repetitions of slow isolated isometric contractions [heel drops] with the noninjured limb performing the concentric contraction to return to the start position) as one of the included interventions. Studies comparing the standard Alfredson protocol with another active intervention used heavy slow resistance exercises, the Silbernagel protocol 19 (daily dose of concentric, eccentric, and plyometric loading of the Achilles tendon), and a “do-as-tolerated” Alfredson protocol. Ten studies 1,5,6,10,19,22,37-39,54 used a 12-week exercise intervention period while only 1 study 55 used an 8-week and 1 study 47 used a 6-week exercise intervention period. Nine studies used the VAS, while 9 studies used the VISA-A.
Characteristics of Each Included Study a

a EE, eccentric exercises; ESWT, extracorporeal shockwave therapy; F, female; HSR, heavy slow resistance exercises; M, male; NR, not reported; PRP, platelet-rich plasma; PS + MCVC, passive stretching plus a dietary supplement containing mucopolysaccharides type I collagen, and vitamin C; RFM, radiofrequency microtenotomy; US, ultrasound; VAS, visual analog scale; VISA-A, Victorian Institute of Sport Assessment–Achilles.
b Median [interquartile range].
Risk of Bias
The assessment of RoB (Figure 2) showed a moderate overall consensus agreement between the 2 reviewers (Gwet AC2 coefficient, 0.53; P < .00001; observed agreement, 80.95%; agreement by chance, 59.52%). Ten studies showed some concerns of bias, # while 2 studies had a high RoB. 10,37 Reasons for high RoB ratings were as follows: a study by Chester et al 10 was given a “some concerns” score in 4 items and a study by Petersen et al 37 had missing outcome data. Only 1 of the 12 studies 38 followed a previously published protocol. Methodological weaknesses included low reporting during data measurement (50% [6/12]) and selection of reported outcomes (91.7% [11/12]). Methodological strengths included the randomization process (91.7% [11/12]) and little deviation from planned interventions due to intervention assignment (91.7% [11/12]) or adherence effects (83.3% [10/12]).

Risk-of-bias scores of the included studies.
Effects of Interventions (Quantitative Analysis: Meta-analyses)
Pain: VAS
Meta-analyses with low-quality evidence showed a statistically significant improvement of pain in the short term (n = 4 studies; n = 212 participants; pooled MD, 10.22 [95% CI, 2.18 to 18.25]; P = .01) in favor of passive treatment modalities (Figure 3). Those differences do not persist for the mid- (n = 5 studies; n = 276 participants; pooled MD, 9.95 [95% CI, –2.72 to 22.62]; P = .12) and long-term follow-ups (n = 2 studies; n = 110 participants; pooled MD, 9.59 [95% CI, –16.96 to 36.15]; P = .48) (Figure 3). When comparing different loading protocols, low-quality evidence showed no significant differences in pain either in the mid- (n = 2 studies; n = 87 participants; pooled MD, 2.18 [95% CI, –8.9 to 13.25]; P = .70) or long-term follow-ups (n = 2 studies; n = 87 participants; pooled MD, 4.90 [95% CI, –3.15 to 12.96]; P = .23) (Figure 4).
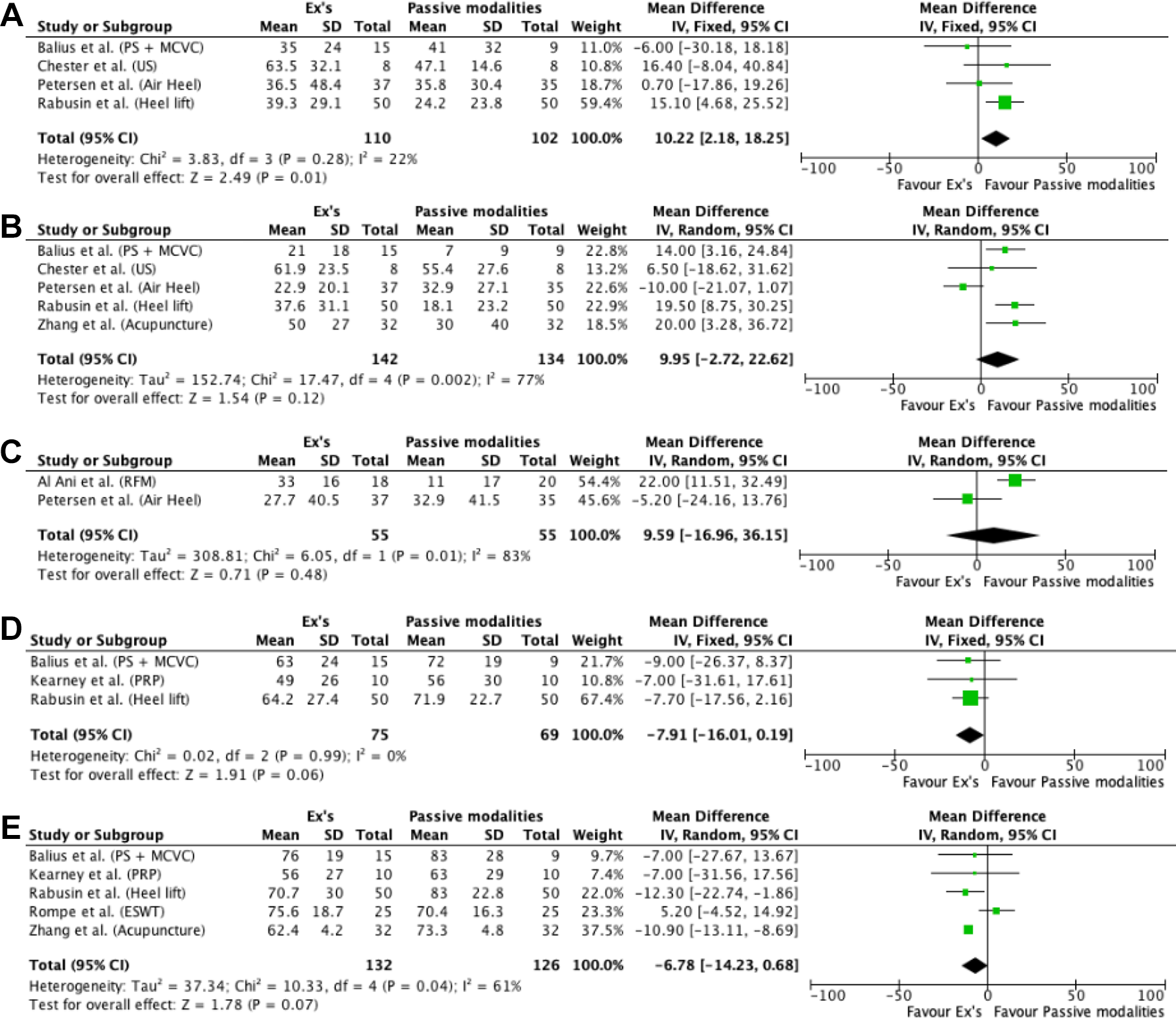
Forest plots of exercises versus passive modalities: (A) short-term pain; (B) midterm pain; (C) long-term pain; (D) short-term function; and (E) midterm function. ESWT, extracorporeal shockwave therapy; Ex’s, exercises; IV, inverse variance; PRP, platelet-rich plasma; PS + MCVC, passive stretching combined with dietary supplements containing mucopolysaccharides, type I collagen, and vitamin C; RFM, radiofrequency microtenotomy; US, ultrasound.
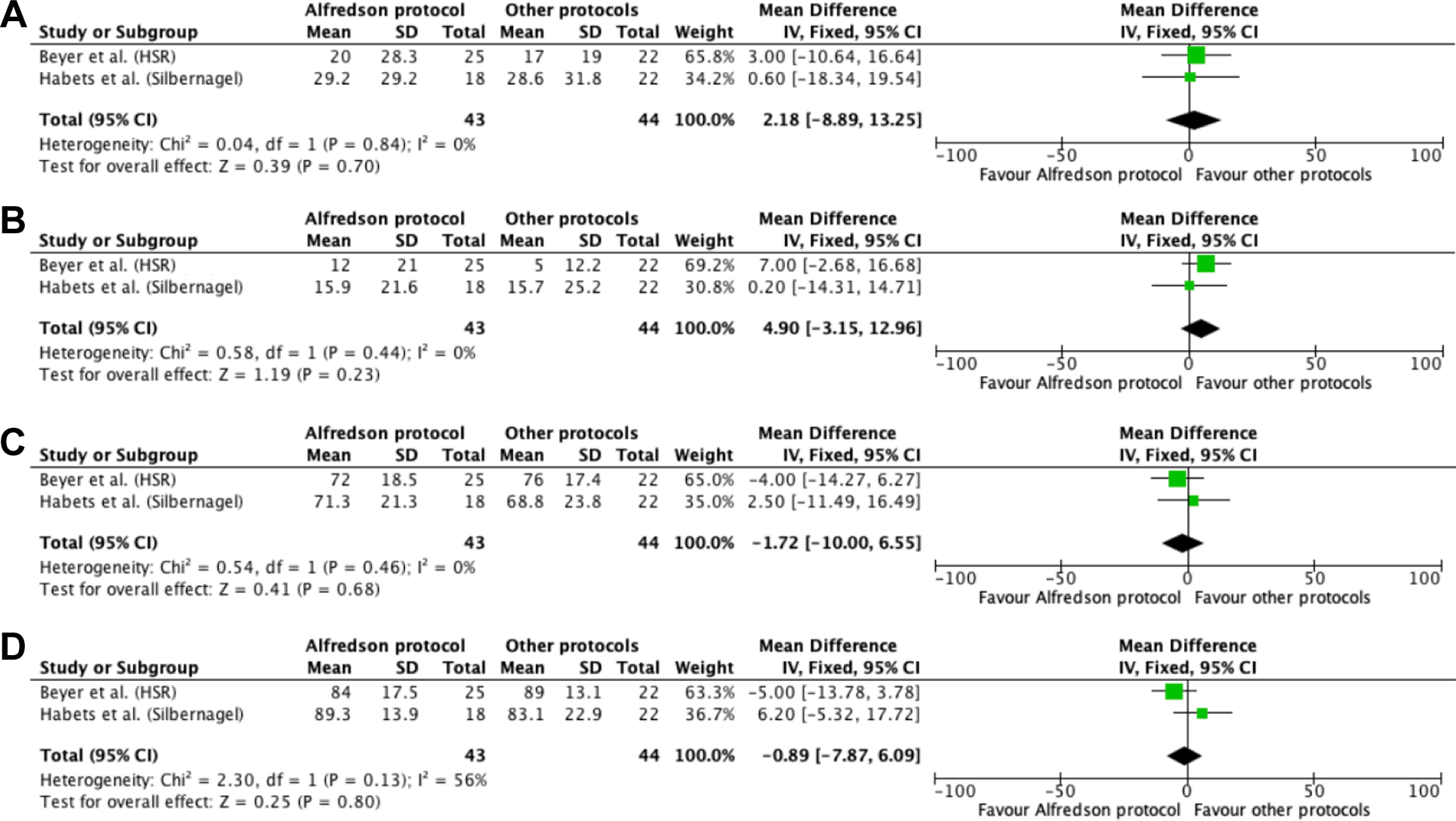
Forest plots of the Alfredson protocol versus other loading protocols: (A) midterm pain; (B) long-term pain; (C) midterm function; and (D) long-term function. HSR, heavy slow resistance exercises. IV, inverse variance.
Function: VISA-A
There was a low level of evidence of a trend in favor of loading protocols in the short- (n = 3 studies; n = 144 participants; pooled MD, –7.91 [95% CI, –16 to 0.19]; P = .06) and midterm follow-ups (n = 5 studies; n = 258 participants; pooled MD, –6.78 [95% CI, –14.23 to 0.68]; P = .07) compared with passive treatment modalities, but those differences were not statistically significant (Figure 3). There were no long-term data for this outcome. Meta-analyses of RCTs comparing different types of loading programs showed a low level of evidence that there were no significant differences at mid- (n = 2 studies; n = 87 participants; pooled MD, –1.72 [95% CI, –10.00 to 6.55]; P = .68) and long-term follow-ups (n = 2 studies; n = 87 participants; pooled MD, –0.89 [95% CI, –7.87 to 6.09]; P = .80) (Figure 4). There was only 1 study reporting short-term data for this outcome. 47
Effects of Interventions (Qualitative Analysis: Studies Not Included in the Meta-analyses)
A study by Yelland et al 54 (n = 29 participants; some concerns of bias) could not be included in the meta-analyses because of missing outcome data. They showed a significant difference (P = .003) in the VISA-A score over 12 months in favor of prolotherapy compared with eccentric loading exercises, but no significant differences for pain. A study by Stevens and Tan 47 (n = 28 participants; some concerns of bias) was not included in the meta-analyses because it was the only one reporting short-term results when comparing different 6-week eccentric exercise protocols. When comparing the standard Alfredson eccentric protocol with a do-as-tolerated protocol, they reported no statistically significant between-group differences for the VISA-A and VAS at week 6. There was a statistically significant between-group difference in VISA-A scores at week 3 (P = .007) in favor of the do-as-tolerated protocol; however, this was partly explained by a within-group deterioration at week 3 in the standard group.
Discussion
The first objective of this systematic review was to compare exercise loading protocols with passive treatment modalities for the management of midportion AT. Meta-analyses did not highlight the superiority of one treatment over another, infirming our initial hypothesis that exercise loading protocols would lead to a better outcome. While passive interventions (in-shoe heel lift, AirHeel brace, ultrasound, and PS + MCVC) led to greater pain reduction in the short term (pooled MD, 10.22 [95% CI, 2.18 to 18.25]; P = .01), loading exercises led to greater short- (pooled MD, –7.91 [95% CI, –16 to 0.19]; P = .06) and midterm (pooled MD, –6.78 [95% CI, -14.23 to 0.68]; P = .07) function improvement—on the margin of statistical significance. There were no long-term differences between the 2 interventions (pooled MD, 4.90 [95% CI, –3.15 to 12.96]; P = .23).
The greater short-term pain reduction for passive interventions highlighted in our meta-analyses is mainly related to 1 study 38 (weight, 59.4%; MD, 15.10 [95% CI, 4.68-25.52) that included a protective intervention (heel lift) known to bring short-term pain relief. Another possible reason explaining the short-term pain decrease associated with passive modalities is that, while resorting to those passive treatments, patients may be asked to rest or minimize the load applied to the tendon so as not to aggravate the symptoms. 1,37,38 Since tendinopathy and its associated symptoms are often due to overuse, this early discharge period could be favorable to short-term pain reduction, unlike exercise loading protocols that aim to gradually increase stress induced on tendons. Thus, one might expect a slight transient increase in pain with protocols such as the Alfredson. This significant difference in pain reduction occurs in the short term but fades in the midterm as patients return to their activities. Loading exercises may have a better influence on short- and midterm function because of pain reduction and the remodeling of the tendon structure, respectively. Eccentric exercises are known to lead to increased tendon stiffness after loading protocols that last several weeks. 15,17 This progressively increased loading is even more important when considering the return to demanding activities, such as running, where a period of rest after pain onset may have led to a decrease in the Achilles tendon load tolerance. 24 Moreover, an outcome that was not present in the literature included in this review but that would be very relevant to compare these interventions, is whether patients returned to their sports and the time it required. Pain is not always an accurate indicator of patient evolution, as it may remain stable over time while they become increasingly active. In addition, it would be interesting to evaluate whether passive interventions without a progressive loading component leave patients at greater risk of symptom recurrence.
The second objective of this study was to compare different loading protocols, and our meta-analyses included only 2 RCTs comparing different exercise protocols. 6,19 There were no statistically significant differences between the different protocols for pain and function. Those results are consistent with those of another recent systematic review that looked at interventions for midportion AT, where nonrandomized studies were included. 34 Murphy et al 34 concluded that there was no significant difference in the VAS and the VISA-A between heavy-load eccentric work and other types of exercise protocols. 6,46,47,49 Even though those protocols use different parameters (ie, load, speed, and number of repetitions), they all follow a similar pattern, which is to gradually increase the load induced on the musculotendinous unit to improve load tolerance. Hence, this is probably one of the reasons explaining the lack of a statistically or clinically meaningful difference between the different exercise regimens. No matter the protocol and the type of exercises used (heavy slow resistance, eccentric, concentric, or isometric), tendon loading remains an effective and recommended intervention for tendinopathy. 14,18,32 However, reweighting of a painful tendon should be monitored and tailored to one’s characteristics to avoid the worsening of symptoms. 42 Complete cessation of physical activity is not necessarily recommended because prolonged resting could lead to maladaptation of the tendon structures and increase the recurrence of injury. 43 If physical activity is adapted to pain and tissue tolerance levels, it does not compromise the integrity of the musculotendinous unit. Therefore, it is crucial to adequately quantify the load during physical activity and consequently during therapeutic follow-ups. 7,51 Besides leading to increased load tolerance, exercises—including eccentric exercises—remain a low-cost intervention and require limited resources, as they can be performed alone at home. 19,36
Clinical Implications
An array of treatments is available for the management of patients with midportion AT; however, there is no consensus on the intervention to prioritize. Since one of the main objectives of patients is to reduce pain as quickly as possible, clinicians could consider including a short period of passive protective modalities, such as heel lift, as part of the early treatment plan. Our results showed that they led to greater short-term pain reduction than exercises, although this pain reduction could be the byproduct of a mandatory rest period. However, this should be done in the context of comprehensive and active care, including exercises. A recent clinical practice guideline strongly recommends the prescription of loading exercises for the management of AT. 32 Results from our meta-analyses have also shown a trend, although not statistically significant, toward eccentric loading exercises, leading to greater short- and midterm function improvements compared with passive modalities. Although exercises may require a significant investment of time on the part of patients, they remain a low-risk, low-cost option, while only necessitating a limited amount of medical resources and being a more durable intervention compared with other options. Recommendations arising from this review should be considered in conjunction with the patient’s clinical profile and preferences regarding treatment selection.
Strengths and Limitations
This was the first systematic review of RCTs comparing eccentric loading exercises to passive modalities or other loading exercise regimens for the management of midportion AT. This review was conducted following rigorous methodological guidelines and only included RCTs that are generally defined as the most appropriate means of studying health care interventions' effectiveness. 28 The control intervention (eccentric loading exercises) chosen by the authors was the same (Alfredson protocol) in almost all the studies included, which allowed for more accurate comparisons between groups and made it possible for us to include 10 studies in the meta-analyses. The follow-up times of the included studies varied considerably for the short-, mid-, and long-term follow-ups, which could have had an impact on our meta-analyses. However, we used time intervals suggested in the literature to define short-, mid-, and long-term follow-up intervals. Only studies in English, French, or German were included, which could have led to a language bias, but we did not exclude any RCTs because of language. Finally, the limited number and lack of high-quality studies included in our meta-analyses limit the strength of the evidence from the results of this study.
Conclusion
Our meta-analyses did not highlight the superiority of one treatment over another for midportion AT. Those results should not stop clinicians from prescribing progressive loading exercises, either in the form of eccentric or a heavy-load, slow-speed (concentric/eccentric) exercise program, since they are recommended by recent clinical practice guidelines. Further research could investigate the different components of loading exercise protocols to identify which parameters have the most influence on pain and function (eg, the load, the speed, the time under tension, or the number of repetitions). This could allow clinicians to optimize the tailoring of loading exercise protocols for the management of midportion AT.
Supplemental material for this article is available at https://journals.sagepub.com/doi/full/10.1177/23259671231171178#supplementary-materials.
Supplemental Material
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671231171178 - Systematic Review and Meta-analyses of Randomized Controlled Trials Comparing Exercise Loading Protocols With Passive Treatment Modalities or Other Loading Protocols for the Management of Midportion Achilles Tendinopathy
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671231171178 for Systematic Review and Meta-analyses of Randomized Controlled Trials Comparing Exercise Loading Protocols With Passive Treatment Modalities or Other Loading Protocols for the Management of Midportion Achilles Tendinopathy by Renaud Maetz, Marc-Olivier Dubé, Arielle Tougas, Félix Prudhomme, Blaise Dubois and Jean-Sébastien Roy in Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted January 26, 2023; accepted February 22, 2023.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Acknowledgment
The authors thank Martine Gagnon for her help with search strategy elaboration.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.