
Abstract
Background:
Trochlear dysplasia is a primary risk factor for patellar instability and leads to loss of the osteochondral constraint of the patella. Trochleoplasty techniques include the Peterson grooveplasty, which alters the length of the trochlea; however, a radiographic measurement of trochlear length to support this has not been described.
Purpose:
To describe measurements to quantify trochlear length on sagittal magnetic resonance imaging in patients with and without patellar instability and to correlate trochlear length with measurements of trochlear dysplasia.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A total of 66 age- and sex-matched knees (36 female and 30 male; mean age, 20.8 ± 4.8 years) were included in this study, of which 33 had patellar instability. Trochlear extension length (TEL) and trochlear alpha angle (TAA) were measured on 3 sagittal magnetic resonance imaging scans (center of the knee, center of the medial condyle, and center of the lateral condyle), and measurements were compared between symptomatic and control knees. Receiver operating characteristic curve analysis was performed, and the area under the curve (AUC) was calculated to describe the accuracy of each measurement to distinguish between knees with and without patellar instability. Linear and multivariate regression analyses were performed to assess the relationship between sagittal measurements and axial measurements of trochlear dysplasia, including lateral trochlear inclination, sulcus angle, and trochlear depth, as well as patient size reflected by the epicondylar distance.
Results:
In symptomatic knees, the central trochlea extended more proximally than in control knees, as determined by the TEL (14.0 ± 3.0 vs 11.5 ± 2.3 mm, respectively; P < .001) and TAA (68.4° ± 3.8° vs 70.5° ± 3.4°, respectively; P = .017). AUC calculations showed that a TEL ≥11 mm at the central trochlea was predictive of patellar instability in both male and female knees (AUC = 0.83 and 0.77, respectively), as was a TAA ≤67° in female knees (AUC = 0.72). An independent association between the central TEL and sulcus angle was found. The central TEL showed a weak correlation with patient size, as measured by the epicondylar distance, while the TAA did not.
Conclusion:
In knees with symptomatic patellar instability, the central trochlea was found to extend 2.5 mm more proximally than in control knees, and this increase in length correlated with severity of trochlear dysplasia. As radiographic examinations of the trochlea and grooveplasty procedures are often based on the proximal extent of the cartilaginous trochlea, further studies are needed to identify the role of trochlear length in the assessment and treatment of trochlear dysplasia in the setting of patellar instability.
Keywords
Trochlear dysplasia is a primary contributor to patellar instability and has been identified in 96% of patients with patellar dislocations. 13 It is characterized by flattening of the trochlear groove, which can reduce the bony constraint of the patellofemoral joint. The shape of the trochlea provides stability to the patellofemoral joint in knee flexion >30°, while the soft tissue restraints play a prominent role in extension. 3 The abnormal shape of a dysplastic trochlea has been described on axial imaging as a decreased slope of the medial or lateral condyle as well as a decreased depth of the trochlear floor and abnormalities in trochlear width. 2,8,14,15,26
Several studies 5,6,17,23 have assessed patients who sustained first-time patellar dislocations and identified trochlear dysplasia as a primary risk factor for recurrent instability. While the cause of patellar instability is multifactorial, Christensen et al 10 noted in a retrospective study of 584 patients that the presence of trochlear dysplasia was the primary risk factor (odds ratio, 18.1) for the recurrence of instability after a first-time patellar dislocation episode. Furthermore, the time to recurrence was decreased by 23.0 months in patients with trochlear dysplasia.
Given the association between abnormal trochlear morphology and patellar instability, there has been increased interest in addressing the geometry of the trochlea in the surgical treatment of patellar instability. Trochleoplasty has been described to address dysplasia in severe cases, with multiple techniques proposed to increase the osteochondral constraint of the patellofemoral joint. 19 Albee 1 described a trochleoplasty technique that increases the height of the lateral condyle. The Dejour deepening trochleoplasty increases the depth of the trochlea in cases of a shallow or convex sulcus. 12 The Peterson technique 20 is another trochleoplasty procedure that involves removal of the proximal trochlea and coverage with a synovial flap. This procedure is designed to remove a supratrochlear spur that can prevent proper patellofemoral articulation in early knee flexion. Arendt 4 recently discussed the benefits of this technique as a safe alternative to deepening trochleoplasty but emphasized that very little guidance exists on the exact indications for the procedure. Such limitations can be attributed to the fact that understanding of normal anatomy regarding trochlear length, and a method to assess the amount of resection needed, has not been described. Furthermore, Arendt 4 noted that “improved imaging measurements are needed to help characterize the most proximal trochlea sulcus.”
A dysplastic trochlea can be characterized in terms of depth and length, with the combination of an inadequate depth and an excessive length contributing to the characteristic appearance of a supratrochlear spur. While many radiographic measurements of trochlear dysplasia exist, the majority of measurements assess the geometry and depth of the groove in the axial view. However, considerable variability in trochlear measurements has been reported based on the axial slice on which the measurement is performed. 2 Currently, no consensus exists on the optimal axial slice on which to measure trochlear anatomy. The most proximal axial cut demonstrating the trochlear cartilage is commonly utilized for measurements; however, the position of this cut may vary between patients if the trochlear length is not consistent.
The aim of this study was to describe the sagittal length of the trochlea and its relationship to trochlear dysplasia in knees with and without symptomatic patellar instability. We hypothesized that the trochlea would demonstrate greater proximal extension in patients with patellar instability. Furthermore, we hypothesized that these measurements would correlate with the severity of traditional radiographic measurements of trochlear dysplasia and may serve as an additional tool when evaluating or surgically correcting trochlear morphology in the management of patellar instability.
Methods
After obtaining institutional review board approval, we reviewed the records of consecutive patients with symptomatic patellar instability, aged 15 to 40 years, who underwent magnetic resonance imaging (MRI) of the affected knee between 2019 and 2021. Patients with a history of surgical treatment and those with degenerative or traumatic changes that affected the morphology of the trochlea were excluded. Knees were compared with MRI of age- and sex-matched controls with a diagnosis of an isolated meniscal injury, which were obtained from an institutional database. Images, radiology reports, and hospital charts were reviewed to confirm that the patients had no current or previous patellofemoral symptoms or injuries, and those who did were excluded from the control group.
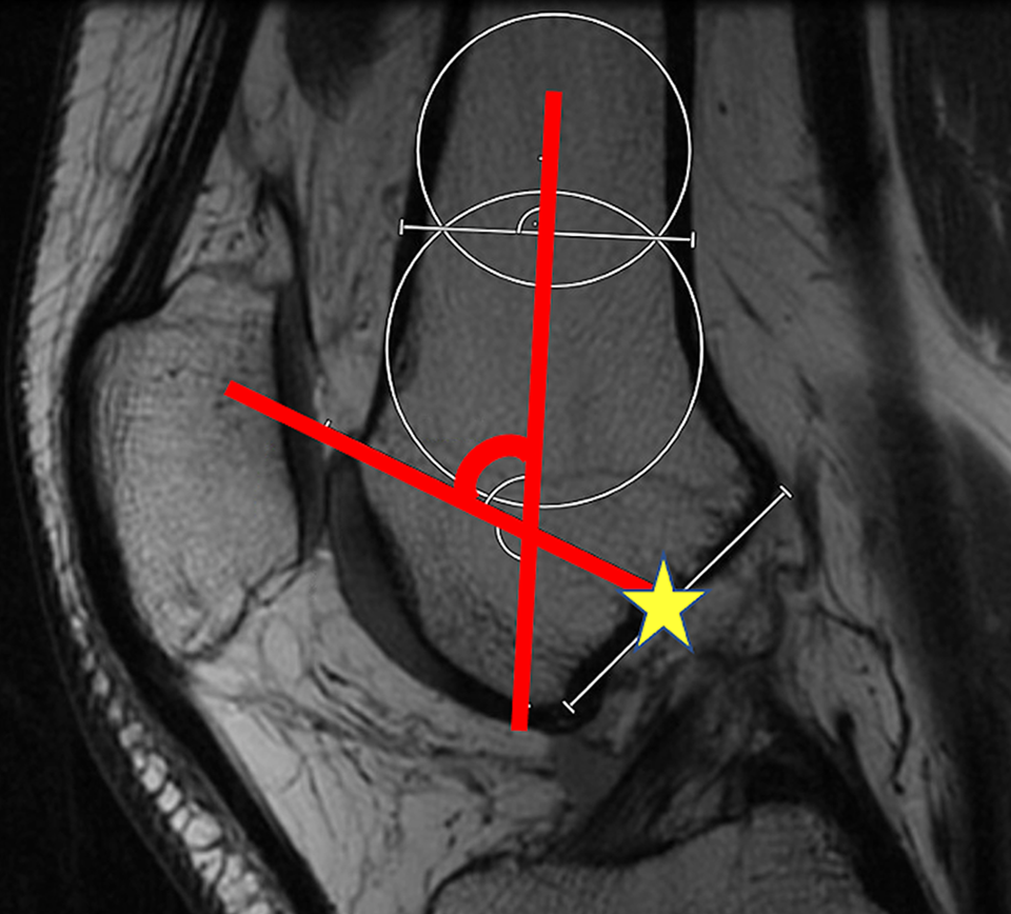
MRI measurements were performed using software with a sensitivity of 0.1 mm (Visage Imaging) by a sports medicine orthopaedic fellow (N.P.J.P.) and a graduate student (Z.L.L.) trained to perform the measurements. The central sagittal cut through the knee was identified as the image on which the most proximal aspect of the intercondylar notch was visualized. On this image, the axis of the femoral shaft was identified as a line perpendicular to the line connecting the overlap of 2 circles (shown in blue in Figure 1) that spanned the diameter of the femoral shaft, as previously described by Biedert et al. 7 A reference plane was identified perpendicular to the axis of the femoral shaft, through the midpoint of the Blumensaat line. The midpoint was defined as the bisecting point on the line that represented the most proximal aspect of the notch in the sagittal view (Figure 1).

The axis of the femoral shaft (red line) was identified based on a line perpendicular to the line connecting the overlap of 2 circles (blue) that spanned the diameter of the femoral shaft. A reference plane (yellow line) was identified perpendicular to the shaft, through the midpoint of the Blumensaat line (yellow star).
The sagittal length of the trochlea was described based on the most proximal extension of the trochlea relative to these reference lines. The trochlear extension length (TEL) was defined as the distance from the plane through the midpoint of the Blumensaat line to the proximal extent of the trochlea; this distance was measured in line with the axis of the femoral shaft and reported in millimeters (Figure 2). The trochlear alpha angle (TAA) was defined as the angle between the femoral axis and a line from the intercondylar midpoint through the most proximal extent of the trochlea (Figure 3); a smaller angle indicates more proximal extension of the trochlea and greater trochlear length.

The trochlear extension length (red line) was defined as the distance between the plane (yellow line) through the midpoint of the Blumensaat line (yellow star) to the proximal extent of the trochlea, measured parallel to the axis of the femoral shaft (blue line).
The trochlear alpha angle was defined as the angle (red lines) on the sagittal image between the femoral axis and a line from the intercondylar midpoint (yellow star) through the most proximal extent of the trochlea.
Each measurement was performed on 3 sagittal MRI scans using constant reference points on the femur to account for variability in the trochlear position on the femur. 24 Measurements were performed on sagittal images through the center of the knee, center of the medial compartment, and center of the lateral compartment. The center of the knee was defined in the sagittal view as the image best demonstrating the linear roof of the intercondylar notch and was confirmed in the axial view as the center of the Roman arch appearance of the posterior condyles. The centers of the medial and lateral compartments were identified by choosing the cut that best demonstrated the greatest diameter of the posterior medial and lateral condyles, respectively. To aid in identification of the sagittal slices, the axial view was used to identify the sagittal slice that corresponded with the center of the medial and lateral condyles.
On axial MRI, standard measurements of trochlear dysplasia were performed. The axial cut demonstrating the classic Roman arch between the posterior condyles was selected for the measurements to account for variability in the trochlear length and position between knees (Figure 4, A-C). Lateral trochlear inclination (LTI) was measured as the angle formed by a line from the deepest portion of the cartilaginous trochlear groove to the most anterior point on the cartilaginous lateral femoral condyle with a line along the posterior condylar axis (Figure 4A). 9 Sulcus angle was measured as the angle formed between the deepest portion of the cartilaginous trochlear groove and the 2 most anterior points on the cartilaginous trochlea (Figure 4B). 11 Trochlear depth was calculated by subtracting the distance between the posterior condylar axis and the deepest point of the trochlear groove from the mean anteroposterior distance of the medial and lateral femoral condyles (Figure 4C), 21 with a depth <3 mm considered to be abnormal. 21

(A) Lateral trochlear inclination was measured as the angle formed by a line from the deepest portion of the cartilaginous trochlear groove to the most anterior point on the cartilaginous lateral femoral condyle with a line along the posterior condylar axis (dashed line). (B) Sulcus angle was measured as the angle formed between the deepest portion of the cartilaginous trochlear groove and the 2 most anterior points on the cartilaginous trochlea. (C) Trochlear depth was calculated by subtracting the distance between the posterior condylar axis and the deepest point of the trochlear groove from the mean anteroposterior distance of the medial and lateral femoral condyles: ((A + C)/2) – B.
To assess the trochlear position on the femur and its relationship to trochlear length, the medial and lateral margins of the trochlea were quantified as a medial-lateral percentage along the posterior condylar axis. In the axial view best demonstrating the Roman arch, the deepest point of the cartilaginous trochlea was identified as well as the most anterior points of the cartilaginous medial and lateral trochlea. All points were expressed as a percentage along the posterior condylar axis, with 0% representing the medial border of the femur and 100% representing the lateral border of the femur (Figure 5). Additionally, on the same axial slice, the epicondylar distance was measured as a reflection of patient size; this was measured as the maximal distance between the medial and lateral epicondyles at the margin of the subchondral bone.

To assess the role of the trochlear position on the femur, the deepest portion of the trochlear groove and medial and lateral margins of the trochlea (blue lines) were quantified as a percentage along the posterior condylar line (red line divided by white line).
Statistical Analysis
To test our hypothesis that measurements of trochlear length would vary between symptomatic and asymptomatic knees, an independent t test was used after assessing for normality. To achieve 95% statistical power for detecting a difference of 2.0 mm with a 3.0-mm SD in trochlear length between symptomatic and asymptomatic knees, with an overall 2-tailed type I rate of 5%, we calculated that a minimum of 60 knees was needed. Sample-size calculation was performed using G*Power (Version 3.1).
To assess for interobserver agreement, an orthopaedic surgeon (M.J.T.), a sports medicine orthopaedic fellow (N.P.J.P.), and a graduate student (M.V.V.) trained to perform the measurements conducted all measurements independently in 5 randomly selected knees. Intrarater reliability was determined by a single observer (M.V.V.) performing each measurement 3 times in 5 randomly selected knees on nonconsecutive days. Interobserver and intraobserver agreement were assessed using the intraclass correlation coefficient (ICC) through a 2-way mixed-effects model with absolute agreement. Absolute agreement in an ICC evaluates how much each measurement performed per observer differs from the other observer and was interpreted according to the guidelines proposed by Shrout and Fleiss 22 as follows: 0.00-0.10, virtually none; 0.11-0.40, slight; 0.41-0.60, fair; 0.61-0.80, moderate; and 0.81-1.00, substantial.
Descriptive statistics were used to present the measurements of trochlear morphology. The Shapiro-Wilk test was performed to assess for normality of the data, and an independent t test was performed to assess for significant differences in the TEL and TAA between symptomatic and asymptomatic knees.
Receiver operating characteristic curve analysis was performed, and the area under the curve (AUC) was calculated to describe the accuracy of each measurement to distinguish between knees with and without patellar instability. An AUC >0.7 was considered to be a valuable diagnostic test. The Youden J statistic was calculated (J = sensitivity + specificity – 1) to determine optimal cutoff values for each measurement to distinguish between knees with and without patellar instability.
Univariate linear regression analysis was performed to assess the relationship between each measurement and patient size, which was reflected by the epicondylar distance. Stepwise multiple regression analyses were performed to assess for independent relationships between sagittal measurements and axial measurements of trochlear dysplasia, including LTI, sulcus angle, and trochlear depth, as well as the medial-lateral positions of trochlear landmarks. All analyses were performed using Real Statistics Resource Pack software (Release 7.2) in Excel (Microsoft). P values <.05 were considered significant.
Results
A total of 66 knees were included in this study: 33 knees from 33 symptomatic patients (18 female and 15 male) were compared with 33 age- and sex-matched control knees. The mean age was 20.8 ± 4.8 years in both the symptomatic and control groups. The ICCs for interrater and intrarater reliability were 0.839 and 0.966 for the TEL, indicating excellent agreement. Similarly, the ICC was 0.887 and 0.907 for interrater and intrarater reliability, respectively, for the TAA.
The results of trochlear length measurements are summarized in Table 1. In symptomatic knees, the central trochlea was found to extend more proximally than in asymptomatic knees, as determined by the TEL (14.0 ± 3.0 vs 11.5 ± 2.3 mm, respectively; P < .001) and TAA (68.4° ± 3.8° vs 70.5° ± 3.4°, respectively; P = .017).
TEL and TAA Measurements a
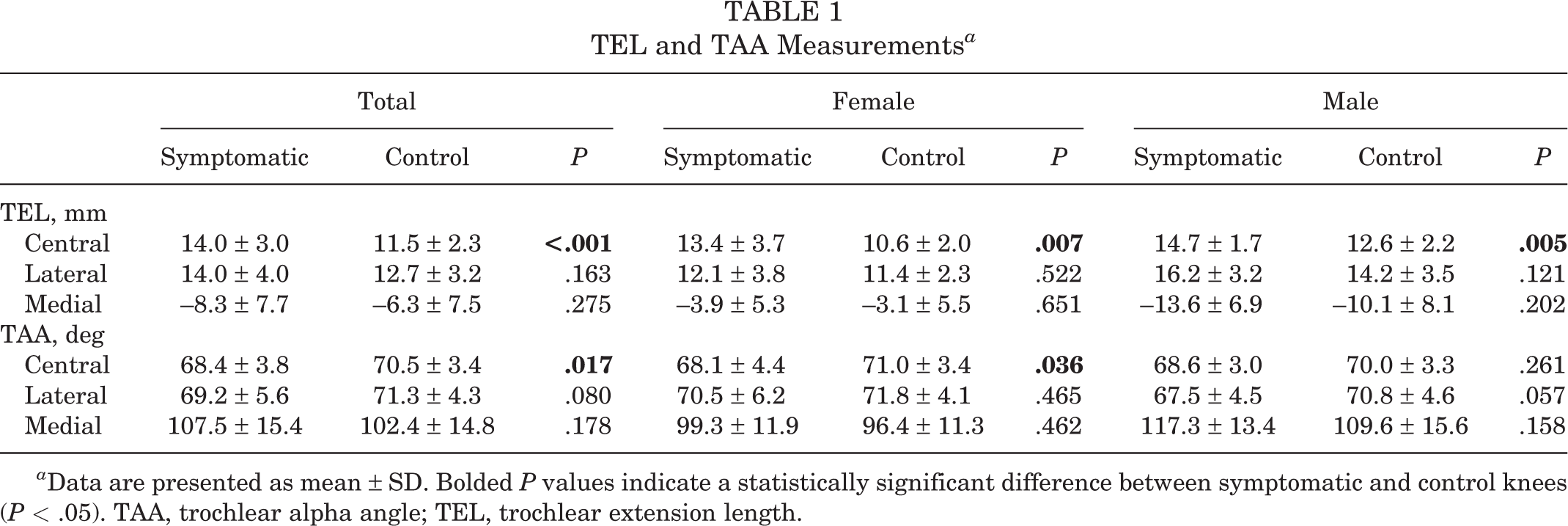
a Data are presented as mean ± SD. Bolded P values indicate a statistically significant difference between symptomatic and control knees (P < .05). TAA, trochlear alpha angle; TEL, trochlear extension length.
AUC calculations showed that a TEL ≥11 mm at the central trochlea was predictive of patellar instability in both male and female knees (AUC = 0.83 and 0.77, respectively), as was a TAA <67° in female knees (AUC = 0.72). The AUC values for each measurement are presented in Table 2. A TEL ≥11 mm was found to have a sensitivity of 75.8%, specificity of 66.7%, positive predictive value of 69.4%, and negative predictive value of 73.3% in identifying knees with patellar instability. In female knees, a TAA <67° at the central trochlea had a sensitivity of 88.9%, specificity of 55.6%, positive predictive value of 66.7%, and negative predictive value of 83.3%.
Cutoff and AUC Values for TEL and TAA a
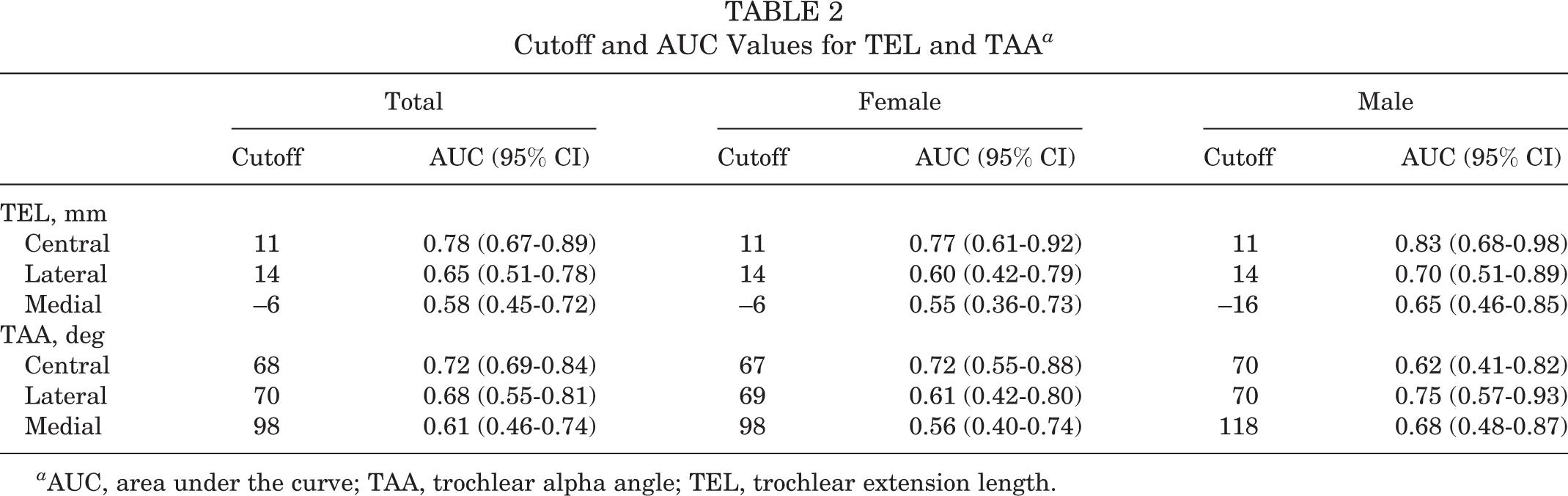
a AUC, area under the curve; TAA, trochlear alpha angle; TEL, trochlear extension length.
The symptomatic knees displayed a greater severity of trochlear dysplasia on all axial measurements, with a smaller LTI (12.0° ± 4.9° vs 16.9° ± 3.8°; P < .001), larger sulcus angle (158.9° ± 9.8° vs 146.7° ± 6.0°; P < .001), and smaller trochlear depth (3.1 ± 1.2 vs 4.4 ± 1.1 mm; P < .001). The assessment of the medial-lateral position of the trochlea showed a significant difference in the medial boundary of the trochlea (40.9% ± 3.9% vs 37.7% ± 3.2%, respectively; P < .001) and no differences in the central or lateral aspects. A summary of these measurements is shown in Table 3.
Medial-Lateral Position of Trochlear Landmarks a

a Data are presented as mean ± SD in percentages (0% = most medial aspect of femur; 100% = most lateral aspect of femur). Bolded P values indicate a statistically significant difference between symptomatic and control knees (P < .05).
To assess the association of measurements with patient size, linear regression analysis between trochlear length measurements and epicondylar distance was performed. This demonstrated a weak correlation between the central TEL and epicondylar length (R = 0.32; R 2 = 0.10; P = .009). No significant relationship between patient size and TAA was identified. Stepwise multiple regression analysis demonstrated an independent relationship between the central TEL and sulcus angle (coefficient = 0.12; R = 0.42; R 2 = 0.18; P < .001). Results of multiple linear regression analyses are shown in Table 4.
Results of Stepwise Linear Regression Analyses a
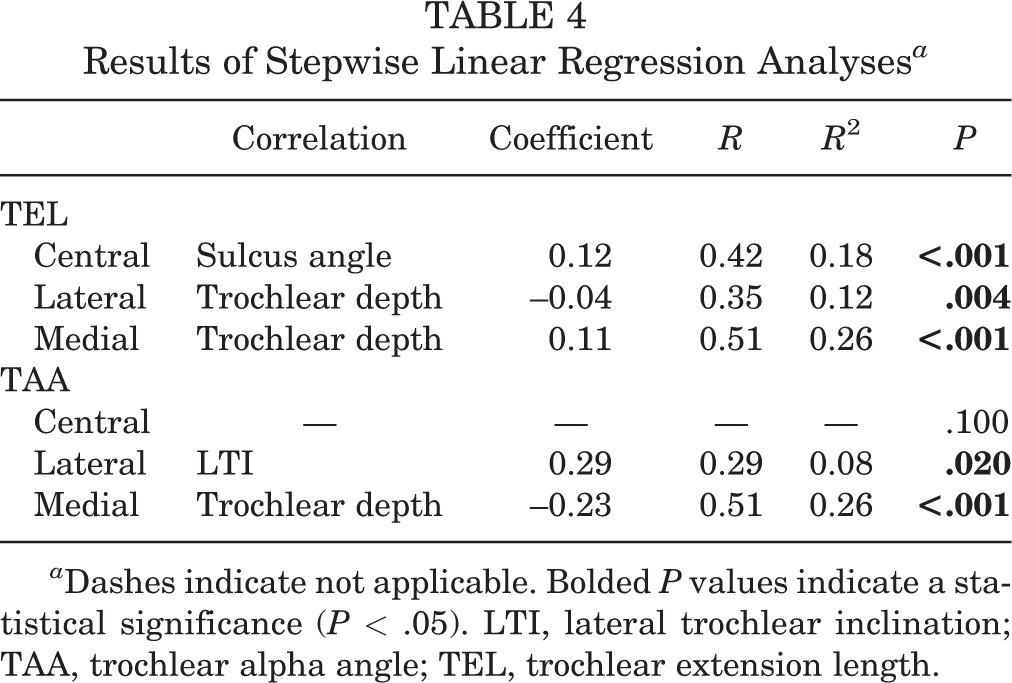
a Dashes indicate not applicable. Bolded P values indicate a statistical significance (P < .05). LTI, lateral trochlear inclination; TAA, trochlear alpha angle; TEL, trochlear extension length.
Discussion
The most important finding of this study was that proximal extension of the trochlea, as measured by the TEL and TAA, was greater in knees with patellar instability than in control knees. These measurements were found to be reliable and reproducible and may serve as a future tool for the evaluation of trochlear length on sagittal MRI. Identified TEL and TAA cutoff values were predictive of knees with patellar instability, demonstrating the role of trochlear length in the pathophysiology of patellar dislocations. Furthermore, the severity of trochlear dysplasia, as measured in the axial view, was found to correlate with these measurements, suggesting that procedures to address trochlear morphology should also consider an evaluation of the sagittal plane.
Currently, little is known about trochlear length in patients with patellar instability. Voss et al 25 quantified trochlear length and volume on computed tomography based on the distance between the first axial cut distal to the physeal scar and the final axial image on which the sulcus was visualized at the level of the intercondylar notch. In their study, they reported that the trochlear length was shorter in knees with dysplasia However, the patients were not matched by sex, and the authors reported that there was no significant difference in trochlear length when male patients were excluded from the analysis. In contrast, our study used an age- and sex-matched control group to identify differences in both the male and female populations. We also utilized MRI to accurately visualize the length of the cartilaginous trochlea. Furthermore, in establishing a reference plane through the midpoint of the Blumensaat line, we identified a consistent point relative to which trochlear length could be measured. This may have value when performing trochleoplasty procedures to normalize the shape of the distal femur. Future studies are needed to explore the utility of these measurements in identifying knees that may benefit from such procedures.
Biedert et al 7 aimed to describe the morphology of the trochlea on sagittal MRI using the lateral condyle index. In their study, the authors measured the distance from the most distal point of the femur to the proximal aspect of the anterior and posterior condyles, performing measurements at the most lateral aspect of the cartilaginous trochlea. These measurements were presented as a ratio, with a smaller ratio indicating a smaller trochlear length at the lateral condyle. The authors reported high interrater reliability with this measurement and indicated that this ratio was significantly smaller in symptomatic knees than in control knees (86% vs 93%, respectively). In our study, the primary difference was found to be at the central trochlea, where the trochlea was noted to be longer in knees with patellar instability. Our measurements in the lateral trochlea approached statistical significance and were found to be longer in the symptomatic group, in contrast to the findings of Biedert et al.
While Biedert et al 7 described the lateral condylar index based on the most lateral sagittal image on which the articular cartilage can be visualized, our study performed lateral measurements at the center of the lateral femoral condyle. In utilizing a reference on the femur, as opposed to the trochlea, we accounted for the variability that can exist in the medial-lateral position of the trochlear sulcus on the femur 24 , allowing for comparisons between knees. In our study, the location of the medial boundary of the trochlea was found to differ between symptomatic and control knees on the axial cut. Although our study did not show significant differences in the position of the lateral margin of the trochlea, the utilization of different sagittal cuts to visualize the trochlear cartilage may have contributed to the discrepancy between our findings and those of Biedert et al. Given that our measurements at the central trochlea were able to identify knees with patellar instability with high accuracy, further studies are needed to understand the optimal measurements of trochlear length that can be applied to trochleoplasty and to describe the influence of trochlear position and length on the kinematics of patellofemoral instability.
The proximal extent of the cartilaginous trochlea is often utilized as a reference point when analyzing radiographic images. Many axial measurements of the patellofemoral joint rely on identifying the proper axial cut to ensure proper measurements of trochlear morphology. 2,18 Fucentese et al 16 reported on changes that occur after trochleoplasty for trochlear dysplasia in the treatment of patellar instability. They reported on 18 knees with trochlear dysplasia that had undergone trochleoplasty and described measurements on axial computed tomography before and after the procedure. After the procedure, they reported that trochlear depth, sulcus angle, and LTI improved, particularly in the proximal aspect of the trochlea, which they defined as the initial cut in which the trochlea is “completely covered with cartilage.” As our study demonstrates that this initial cut of the trochlea may vary in location between knees with and without patellar instability, further studies are needed to understand the optimal techniques for assessing and re-creating normal trochlear anatomy and length during the surgical treatment of patellar instability.
Surgical techniques to address trochlear length during trochleoplasty have previously been described. Although most trochleoplasty procedures have focused on increasing trochlear depth, the technique described by Peterson et al 20 addresses trochlear length, removing the excess bone and cartilage at the proximal margin of the trochlea. However, the ideal amount of resection during this procedure has not been previously described. In our study, we found that knees with patellar instability had an increased TEL of 2.5 mm at the center of the knee, and that the normal length was 10.6 and 12.6 mm in female and male knees, respectively. These values may serve as a reference for future studies to further refine guidelines for trochleoplasty techniques.
Limitations
This study has some limitations that should be considered. The study was performed retrospectively, and therefore, no physical examination or patient-reported outcomes were available to correlate to the images, as the patients were not contacted regarding their symptoms. We also did not differentiate between first-time and recurrent dislocations in this study. Moreover, the standard cut on MRI was 3 mm in thickness, which could lead to variation in the sagittal images selected for measurements. Imaging was conducted at 1 institution but was not performed on the same MRI scanner, which may contribute to variability in imaging protocols. Additionally, the status of the patients was not blinded to the observers who were performing the measurements. Last, while we standardized the central, medial, and lateral sagittal images on which measurements were performed based on condylar morphology, these locations may not necessarily correlate with the cartilaginous boundaries on the proximal trochlea, and further studies are needed to better understand the role of trochlear length, 3-dimensional morphology, and function as they relate to patellar stability.
Conclusion
In knees with symptomatic patellar instability, the central trochlea was found to extend 2.5 mm more proximally than in control knees, and this increase in length correlated with measurements of trochlear dysplasia. TEA and TAA measurements may have utility in defining the indications for surgical procedures that address trochlear length. As grooveplasty procedures and radiographic examinations of the trochlea are often based on the proximal extent of the cartilaginous trochlea, further studies are needed to identify the role of trochlear length in the assessment and treatment of trochlear dysplasia in the setting of patellar instability.
Footnotes
Final revision submitted January 18, 2023; accepted February 26, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: Funding for this study was received from the National Institutes of Health (grants R21EB031185, R01AR081344, and R01AR079442 to M.J.T. and F.L.). M.J.T. has received education payments from Kairos Surgical, has received consulting fees from DePuy Synthes, and has a spouse who has received consulting fees from Smith & Nephew. N.P.J.P. has received education payments from SportsTek Medical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Massachusetts General Hospital (No. 2019P003614).