
Abstract
Background:
The femoral trochlea is considered the most significant osseous factor affecting stability in the patellofemoral joint. The true prevalence of trochlear dysplasia in the general population is largely unknown.
Purpose/Hypothesis:
To investigate the prevalence of trochlear dysplasia in the general population. Our hypothesis was that, while trochlear dysplasia is not uncommon, there is a low prevalence of severe dysplasia in the general population.
Study Design:
Descriptive epidemiology study.
Methods:
Five observers were asked to evaluate 692 skeletally mature femoral specimens from 359 skeletons for trochlear dysplasia at 2 time points. We further subclassified the dysplastic trochlea in 62 femora with the highest rated degree of dysplasia.
Results:
Sex (P = .11) and race (P = .2) had no effect on the severity of dysplasia. Interobserver reliability was excellent (0.906 and 0.904), and intraobserver reliability was good to excellent (0.686 to 0.808). The percentages of trochlea graded as normal, mildly dysplastic, moderately dysplastic, and severely dysplastic were 61.5%, 21.4%, 12.7%, and 4.4%, respectively, in the first evaluation, and 58.5%, 23.7%, 12.7%, and 5.1% in the second evaluation. Of the 62 trochlea with the highest scores for dysplasia, 36 had trochlear dysplasia without a supratrochlear spur, 8 had trochlear dysplasia with medial femoral condyle hypoplasia, and 18 had trochlear dysplasia with a supratrochlear spur.
Conclusion:
Observers with differing degrees of clinical experience had similar opinions on the degree of trochlear dysplasia. Also, our cohort showed that moderate to severe dysplasia is not uncommon, as it is present in approximately 17% of knees in our cohort. Our findings also suggest that clinicians are speaking the same language when identifying and describing trochlear dysplasia on gross inspection.
Trochlear dysplasia refers to a pathologic variation in the shape and depth of the femoral trochlear groove. Trochlear dysplasia was first described by Richerand in 1802 14 and has been shown to have a principal role in controlling the patellofemoral gliding mechanism. 11 The normal trochlea is concave, which helps with proper patellar tracking throughout the range of knee motion. Conversely, in knees with trochlear dysplasia, the trochlear groove can be insufficient because of either an elevated trochlear floor or a deficient lateral condyle. 22 Trochlear dysplasia can predispose the patella to lateral subluxation or dislocation. 22 In fact, trochlear dysplasia has been proposed to be one of the most significant factors implicated in recurrent patellar instability. 25,27 The trochlea plays the most significant role when the knee is flexed beyond 30°. Therefore, the morphology of the femoral trochlea is extremely important for patellofemoral stability as the knee moves from full extension into greater degrees of flexion. 17
Normal trochlear development and morphology have been observed and documented in several studies. 12,13,29 Glard et al 12 suggested that there was no significant difference in the trochlear sulcus angle between fetuses and adults. The absence of change in trochlear morphology with age was further supported by Nietosvaara, 23 who reported that there was no significant change in the cartilaginous sulcus angle from birth to 18 years of age. In another study, Parikh et al 25 suggested that the dysplastic trochlea maintained its abnormal shape during the adolescent growth years. These studies indicate that the shape of the trochlea is largely maintained during growth and development and does not change significantly after birth.
Trochlear dysplasia is defined by both clinical and radiologic criteria. To help with communication and guide management for patellofemoral instability, several authors have attempted to categorize trochlear morphology. Biedert and Bachmann 3 grouped trochlear dysplasia into 2 morphologic types. In the first, patients had an isolated abnormal lateral trochlear height with normal central and medial heights. The second type comprised patients with abnormal trochlear height in the central and/or medial trochlea with normal lateral height. It is still unclear whether pathologic trochlear dysplasia is caused by hypoplasia of the lateral condyle or whether it can be attributed to excessive bone in the central and/or medial trochlea. 3 These authors reported that the majority (83.4%) of dysplastic trochleae were predominantly caused by an elevated trochlear floor and had normal lateral condylar height, and a minority (16.6%) of trochlear dysplasia cases were secondary to a deficient lateral condylar height but had normal trochlear height.
Radiographically, trochlear dysplasia is defined by a sulcus angle of greater than 145° as seen on axial radiographic images of the patellofemoral joint. 6,20 On the lateral knee radiograph, it is defined by the crossing sign, 25 which refers to the crossing over of the trochlear floor condensation with the condensation of the most prominent aspect of the lateral trochlea and is found in 96% of the population with a history of true dislocation but in only 3% of healthy controls. 8,9 Two additional signs of trochlear dysplasia seen on plain radiography are the supratrochlear spur, which is a global prominence of the trochlea, and the double contour sign, a radiographic line representing the hypoplastic medial facet on the lateral view. 19,30
Dejour and colleagues 6,7 classified trochlear dysplasia into 4 types (Figure 1). In type A dysplasia, trochlear morphology is preserved with a fairly shallow trochlea. Type B represents a flat or convex trochlea. Type C dysplasia is demonstrated by asymmetry of the trochlear facets with a convex lateral facet and hypoplastic medial facet. Finally, type D dysplasia has asymmetry of the trochlear facets with medial hypoplasia, the so-called cliff pattern. The Dejour classification is widely referred to in the literature and currently considered the gold standard for the description of trochlear dysplasia in clinical practice. The inter- and intraobserver reproducibility of this classification remains controversial, however, probably because identifying these typical signs depends on subjective visual appraisal. 17

Dejour classifications of trochlear dysplasia. Type A: Crossing sign, trochlear morphology preserved (fairly shallow trochlea, >145°). Type B: Crossing sign, supratrochlear spur, flat or convex trochlea. Type C: Crossing sign, double contour (projection on the lateral view of the hypoplastic medial facet). Type D: Crossing sign, supratrochlear spur, double contour, asymmetry of trochlear facets, vertical link between medial and lateral facet (cliff pattern).
Different surgical techniques have been developed to correct the pathologic morphology seen in patients with recurrent patellofemoral instability. 3,6,31 These techniques involve elevation of the lateral facet, deepening of a flat trochlear groove, and/or removal of a prominent trochlear bump. 1,5 In recent years, there has been an increased interest in directly addressing the trochlear pathology during surgical treatment of recurrent patellofemoral instability. To date, there is no well-defined, agreed-upon criteria to dictate when trochlear morphology should be addressed at the time of surgery for patellar instability. Some authors have suggested that procedures addressing trochlear morphology are performed too commonly based on the true prevalence of trochlear dysplasia in the general population. To our knowledge, there is no study evaluating the prevalence of trochlear dysplasia in the general population. The purpose of the present study is to investigate the prevalence of trochlear dysplasia in the general population. We hypothesize that there is a low prevalence of severe dysplasia in the general population.
Methods
We obtained 698 skeletally mature femoral specimens from the Hamann-Todd Osteological Collection at the Cleveland Museum of Natural History. With more than 3000 complete human skeletons with complete specimen information, the Hamann-Todd Collection is the largest collection of human skeletal specimens in the Western hemisphere. Height, weight, sex, race, and age at time of death are all contained in the institution’s database. We excluded 4 femora because of their poor condition, which precluded proper evaluation. Two additional femora were excluded because their photographs were considered inappropriate for evaluation. Thus, we included a total of 692 femora from 359 skeletons. The mean age at the time of death was 30.58 years. Table 1 lists the specimen information.
Data of the Study Specimens

Photos of the 345 right femora and 347 left femora were taken according to a standard protocol. Each femur was placed on a hard, flat surface with the distal femur and camera perpendicular to each other to get the best axial image of the trochlea (Figure 2). (Photos were taken by the study authors.)
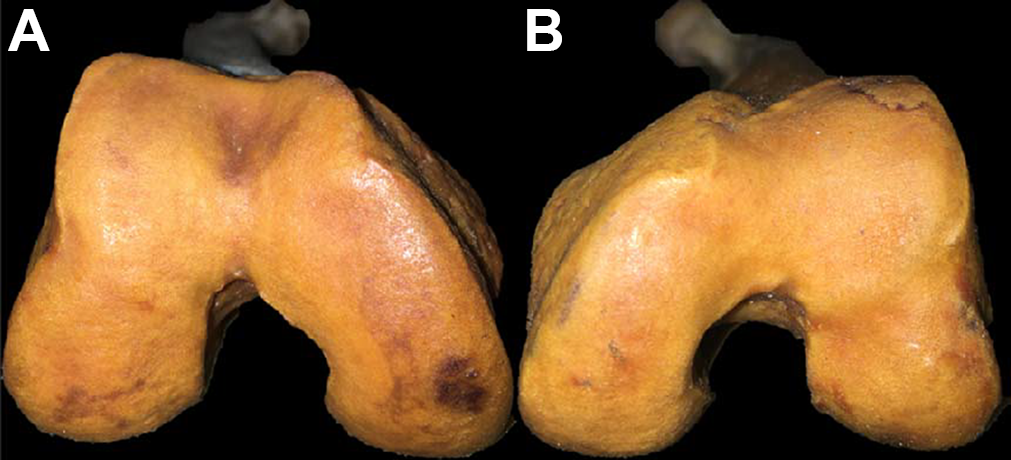
Images of the (A) right and (B) left trochlea, taken perpendicular to the trochlea.
We prepared a presentation in PowerPoint (Microsoft) using the specimen photographs in a random order and sent it to 5 observers of differing clinical expertise. Four observers (S.G.K., J.L.P., P.F., and L.D.F.) were experienced knee surgeons (3 of these surgeons have a patellofemoral practice focus), while 1 (G.I.O.) was a medical student. We asked observers to grade the trochlear dysplasia on a scale between 0 and 3. The degree of dysplasia was defined as follows: 0 = normal, 1 = mild dysplasia, 2 = moderate dysplasia, and 3 = severe dysplasia. A month later, we sent all 5 observers the same specimen photos in a different order and asked them to reevaluate each specimen. Before the image review, only the numbers and descriptors were providers; no special instructions were given to guide grading.
After the second evaluation, we performed gross analysis of each femoral trochlea to further characterize the type of dysplasia. We chose 62 of the femora with the highest grading (≥18) for dysplasia. Morphologic patterns were assessed and noted. Special attention was placed on the morphology of the medial and lateral aspects of the trochlea, central trochlea, and supratrochlear area. The type of dysplasia was described for each femur, and the femora were then placed in groupings based on their respective morphologies.
Statistical Analysis
All observers performed 2 evaluations at 2 different time points, and the inter- and intrarater reliability was assessed utilizing the Landis and Koch 16 interpretation of the kappa statistic (κ), where κ values were classified as follows: ≥0.81, almost perfect (excellent) correlation; 0.61 to 0.8, substantial (good); 0.41 to 0.6, moderate; 0.21 to 0.4, fair; and ≤0.2, slight correlation. The Mann-Whitney U test was used for nonparametric variables. Statistical analysis was performed using SPSS (Version 25; IBM).
Results
There was no statistically significant difference in severity of dysplasia between the male and female specimens (P = .11). Moreover, there was also no statistically significant difference between femora from White versus Black individuals with respect to the severity of dysplasia (P = .2).
The interobserver intraclass correlation coefficients (ICCs) of the first and second evaluations of all observers were found to be 0.906 and 0.904, respectively, indicating excellent reliability. The intraobserver ICCs for reviewers 1 through 5 were 0.799, 0.686, 0.808, 0.787, and 0.778, respectively, indicating good to excellent reliability (Table 2).
Inter- and Intraobserver Correlations a

a ICC, intraclass correlation coefficient.
The percentages of specimens that each reviewer evaluated as having normal, mildly dysplastic, moderately dysplastic, and severely dysplastic trochleae were stratified according to first and second evaluations and are shown in Table 3. Table 4 shows the overall percentages of trochleae rated as normal, mild dysplasia, moderate dysplasia, and severe dysplasia.
Percentages of Trochleae Graded as Normal, Mildly Dysplastic, Moderately Dysplastic, and Severely Dysplastic According to Reviewer and Evaluation Period

Overall Percentages of Trochleae Graded as Normal, Mildly Dysplastic, Moderately Dysplastic, and Severely Dysplastic

Of the 62 trochleae with the highest scores for dysplasia (≥18), 36 (58.0%) had trochlear dysplasia without a supratrochlear spur, 8 (12.9%) had trochlear dysplasia with medial femoral condyle hypoplasia, and 18 (29.0%) had trochlear dysplasia with a supratrochlear spur (Figure 3).

Upper row: Images of a trochlear dysplasia without spur. (A) Lateral, (B) oblique, (C) axial. Middle row: Images of a trochlear dysplasia with spur. (D) Lateral, (E) axial, (F) condylar. Lower row: Axial image of a trochlear dysplasia with medial hypoplasia. The white arrow in panel G depicts the medially directed orientation of the trochlear groove.
Discussion
The principal findings of this study demonstrate that the prevalence of trochlear dysplasia in the general population is not uncommon, with moderate and severe dysplasia having a prevalence of around 17%. Another important finding is that physicians have a common agreement of whether dysplasia exists and also the degree of trochlear dysplasia, which was shown by the excellent interobserver and good to excellent intraobserver reliability.
In this epidemiological study, we aimed to investigate the prevalence of trochlear dysplasia in the general population. Trochlear dysplasia is strongly associated with patellar instability. 25,27 Therefore, it has been a subject of interest among knee surgeons. While trochlear dysplasia is well-recognized as the primary contributor to patellar instability, there is sparse literature regarding biomechanics, natural history, and pathophysiology. 9,12 Also, there is a lack of studies investigating the prevalence of trochlear dysplasia in the general population. Although several studies have investigated trochlear dysplasia in patients with knee complaints, this is the first study to investigate the overall prevalence of trochlear dysplasia in the general population.
Several studies have attempted to evaluate the prevalence of trochlear dysplasia in patients with and those without a history of patellar instability. In a radiologic study, Dejour et al 9 compared radiographs and computed tomography scans of patients with patellar dislocation and control knees. They showed that 96% of patients with a history of patellar dislocation and 3% of the control group had evidence of trochlear dysplasia. They defined 3 indicators of trochlear dysplasia on a true lateral radiograph, including the presence of the crossing sign, a trochlear bump ≥3 mm, and a trochlear depth ≤4 mm at 15° of flexion. While they reported the prevalence of the trochlear dysplasia, they did not report the severity of the dysplasia. In our study, we classified the severity of the dysplasia as mild, moderate, and severe and reported the prevalence of each. This study also differed from our study in that they reported the prevalence based on a radiologic assessment alone. By comparison, in the present study, we were able to grossly examine and categorize skeletal femoral specimens to grade the dysplasia. In addition, we analyzed a superior number of specimens with good to excellent intra- and interrater reliability.
In another study, Ntagiopoulos et al 24 investigated the prevalence of the trochlear dysplasia in 299 patients with anterior cruciate ligament (ACL) ruptures and reported it to be 14.7% (44 patients). The trochlear dysplasia was classified as type A in 93% and type C in 7% of patients. They concluded that the trochlear dysplasia was more prevalent in patients with ACL rupture compared with the general population. This study comprised a specific patient population and was not intended to investigate the overall prevalence of trochlear dysplasia in the general population. In another study, Sanders et al 26 investigated the long-term results of first-time patellar dislocation in 232 skeletally immature patients. In their study, they reported the incidence of trochlear dysplasia in patients with first-time patellar dislocation to be 23.3%. Again, both of these studies included a specific patient population and were not intended to investigate the overall prevalence of trochlear dysplasia in the general population. These studies are therefore not comparable with our study.
More recent studies are focused on identifying the predictors of recurrent patellar dislocation. In a recent case-control study on 94 patients with patellar dislocation and 50 controls, Sundararajan et al 28 identified the predictors for recurrent patellar dislocation utilizing binomial logistic regression analysis and reported the trochlear dysplasia as an anatomic predictor with an odds ratio of 12.0. In a similar study, Jaquith and Parikh 15 identified risk factors for recurrent patellar dislocation in children and adolescents. The presence of trochlear dysplasia was found to be a risk factor on multivariate analysis with an odds ratio of 3.56. Lewallen et al 18 also reported trochlear dysplasia as a predictor of recurrent patellar dislocation in patients under 25 years of age with a hazard ratio of 3.06. These studies in different clinical settings and patient populations consistently reported trochlear dysplasia to be a risk factor for patellar instability. In our study, we were not able to report clinical information. However, the correlation between patellar instability and the severity of trochlear dysplasia is expected to align with the existing literature.
Trochleoplasty has been championed by some authors as a treatment for severe trochlear dysplasia. 2,4,7,8,10 While there are several different types of trochleoplasty procedures described in the literature, groove-deepening trochleoplasty is the most commonly performed type of trochleoplasty today. It basically aims to deepen the patellofemoral joint line and reorient the patellofemoral relationship, helping to prevent early degenerative changes and also improve patellofemoral joint stability. 21 Our results demonstrate that although trochlear dysplasia is not uncommon, the majority of the general population does not exhibit the most severe types of trochlear dysplasia. Given the low prevalence of high-grade dysplasia found, this provides a possible initial explanation as to why several studies report good short-term clinical outcomes with nontrochleoplasty procedures. While longer-term studies comparing similar patients undergoing either trochleoplasty or nontrochleoplasty procedures are needed to determine solid surgical indications, one could reasonably assume that trochleoplasty is not necessary for all patients with some degree of trochlear dysplasia and associated patellar instability.
Our study has several limitations. The primary limitation may be the classification system that we used in our study. Since there was no valid and widely accepted gross anatomic classification system regarding the severity of trochlear dysplasia, we asked our observers to grade the dysplasia according to their own clinical experience. It might be argued that the observers subjectively graded the dysplasia. However, the high concordance on the degree of trochlear dysplasia between observers refutes this. The lack of articular cartilage is another potential critique of this study. Also, although we had information on the sex and race of the femora, we did not have clinical information related to patellofemoral instability. Therefore, it was not possible to predict the actual prevalence of patellar instability.
Conclusion
This study demonstrated that although there were no absolute criteria to evaluate trochlear dysplasia, observers had similar opinions on the degree thereof. Our cohort shows that moderate to severe dysplasia is not uncommon, as it is present in around 17% of knees in our study population and based on our grading system. Our study is the first to investigate the overall prevalence of trochlear dysplasia in the general population. Our findings suggest that clinicians are on the same wavelength when discussing the presence and degree of trochlear dysplasia; however, it should be noted that trochlear dysplasia was evaluated by gross inspection of the femoral specimens, and no imaging techniques and measurements were utilized. This is an important consideration when evaluating and managing patients with recurrent patellofemoral instability.
Footnotes
Acknowledgment
The authors thank Lyman Jellema for his assistance with the performance of this study.
Final revision submitted September 24, 2020; accepted November 18, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.G.K. has received educational support from Arthrex and Elite Orthopedics, consulting fees from DePuy, and nonconsulting fees from Arthrex, Stryker, and Medical Device Business Services. J.L.P. has received education payments from Arthrex; consulting fees from Arthrex, Ceterix, and Smith & Nephew; and nonconsulting fees from Arthrex. L.D.F. has received educational support from Zimmer Biomet. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.