
Abstract
Background:
The coronavirus disease 2019 (COVID-19) pandemic significantly disrupted athletic activities, including those in the Pacific 12 (Pac-12) Conference of the National Collegiate Athletic Association. It is currently unknown how the disruption in training and competition impacted athletes’ risk of injury upon resumption of activities.
Purpose:
To describe and compare the rate, timing, mechanism, and severity of injuries among collegiate athletes across multiple sports in the Pac-12 Conference before and after the COVID-19 pandemic–associated hiatus of intercollegiate athletic activities.
Study Design:
Descriptive epidemiology study.
Methods:
Descriptive and injury data among intercollegiate athletes from both the season before the hiatus and the season after the hiatus were acquired from the Pac-12 Health Analytics Program database. Injury elements (timing of injury onset, injury severity, mechanism, recurrence, outcome, need for procedural intervention, and event segment during which the injury took place) were compared by time using the chi-square test and a multivariate logistic regression model. Subgroup analyses were performed on knee and shoulder injuries among athletes participating in sports with traditionally high rates of knee and shoulder injuries.
Results:
A total of 12,319 sports-related injuries across 23 sports were identified, with 7869 pre-hiatus injuries and 4450 post-hiatus injuries. There was no difference in the overall incidence of injury between the pre-hiatus and post-hiatus seasons. However, the proportion of noncontact injuries was higher in the post-hiatus season for football, baseball, and softball players, and the proportion of nonacute injuries in the post-hiatus season was higher among football, basketball, and rowing athletes. Finally, the overall proportion of injuries sustained by football players in the final 25% of competition or practice was higher in the post-hiatus season.
Conclusion:
Athletes competing in the post-hiatus season were observed to have higher rates of noncontact injuries and injuries sustained in the final 25% of competition. This study demonstrates that the COVID-19 pandemic has had varied effects on athletes from different sports, suggesting that many factors must be considered when designing return-to-sports programs for athletes after an extended absence from organized training.
The coronavirus disease 2019 (COVID-19) pandemic in 2020 spurred health officials worldwide to enact public health measures to reduce the risk of infection, such as social distancing, closing of communal spaces, and cessation of group activities including organized sports. Consequently, the pandemic caused delays in major sporting events and disrupted training for athletes across the United States, with many athletes finding themselves with limited access to training facilities, sports performance personnel, and other resources typically available to them. In the Pacific 12 (Pac-12) Conference of the National Collegiate Athletic Association (NCAA), all competitions and practices across all 24 sports were canceled from March 2020 until November 2020.
One of the potential consequences of this type of disrupted training and competition period is the increased risk of injury that may occur because of alterations in an athlete’s physical strength, endurance, and sports-specific skills.14,16,31,33 For example, Gabbett et al 9 found that rugby players with less finely tuned running ability and lower upper body strength were at higher risk of injury. They hypothesized that players with poor running ability were more prone to fatigue, leading to reductions in tackling technique and consequently injury. A decline in maximal oxygen intake and cardiac output can be seen after as few as 4 weeks of detraining, with reduced muscle force and decreased endurance seen over longer periods.15,20,21 After the months-long detraining period resulting from the pandemic, it is reasonable to hypothesize that athletes’ loss of strength, speed, and other specific skills may lead to increased rates of injury upon return to play.
Prior studies have demonstrated an increased risk of injury after long periods of detraining. Before the 2011 National Football League (NFL) season, failure to reach a collective bargaining agreement led to an 18-week period during which athletes could not access training facilities and medical personnel. After the resumption of play, Myer et al 22 found that players experienced a significant increase in Achilles tendon ruptures upon return to play, which may have been related to the extended period of time players went without typical training regimens. And just last year, Seshadri et al 32 reported a 3-fold increase in injury rate in the Bundesliga (a top-flight German professional soccer league) after they resumed play after a COVID-19–imposed hiatus.
The impact of the COVID-19 pandemic on sports injury epidemiology among collegiate athletes has not yet been explored. Furthermore, while previous studies exploring the effects of detraining have focused on specific high-intensity sports such as rugby, football, and soccer, the effect of long periods of altered training has not been assessed among athletes who participate in certain Olympic sports such as swimming and track and field.
In this study, we aimed to assess whether the trends noted by previous studies would be replicated in the intercollegiate athlete population. Furthermore, we aimed to describe the timing, mechanism, and severity of injuries sustained by high-level intercollegiate athletes before and after the COVID-19 pandemic–associated hiatus of intercollegiate athletic activities (hereafter referred to as the “hiatus”). The characterization of the pandemic’s impact on athletic injury may inform future recommendations for maintaining an athlete’s health and performance during and after a long period away from organized training.
Methods
Data Elements
For the current study, we used the comprehensive Pac-12 Health Analytics Program (HAP) database, which contains data collected by allied health personnel regarding health events among intercollegiate athletes within the Pac-12 Conference. The database includes all injury events that take place during official NCAA competitions or practices. A request was submitted to the HAP data custodians for all injuries that occurred across all sports between January 2019 and June 2021. After approval and execution of a data use agreement between our institution and the Pac-12 Conference, a de-identified data set containing our requested data elements was made available via the Pac-12 HAP secure, cloud-based file-sharing system. This study was determined to be exempt from ethics approval, as we used de-identified data in an aggregate form.
Collected athlete data elements included sex, sport, and calendar year of injury occurrence. Collected injury-specific data elements included anatomic location of injury, injury recurrence (new injury vs recurrence of past injury), injury mechanism (contact vs noncontact; eg, accelerating, decelerating, jumping, running), injury outcome (able or unable to return to competition within the same season), need for procedural intervention, the timing of injury onset, and event segment in which the injury took place (eg, fourth quarter of competition or final 25% of competition or practices).
We defined injuries with symptoms that presented within 24 hours of the injury event as acute, and those with symptoms that presented >24 hours after the injury event as nonacute. All events, including practices, were divided into quarters, and the quarter in which the injury took place was recorded for each injury. Injuries were categorized as pre-hiatus or post-hiatus based on the calendar year of injury and sports-specific schedule. For example, injuries occurring in 2020 were categorized as post-hiatus for the majority of fall sports (eg, football) since they largely resumed competition by October 2020. Since spring sports such as baseball resumed competition later, baseball injuries occurring in 2021 were categorized as post-hiatus. Finally, the location of injury was categorized as upper or lower extremity.
Pre- and post-hiatus injury incidence rates (IRs) per 1000 athlete-exposure hours (AEH) were determined by taking the total number of in-season injuries and dividing by the total athlete-time at risk. Similar to previous literature,24,30 the pre- and post-hiatus IRs for each team were calculated using the following equation:

To estimate time at risk, the total season length in weeks was multiplied by 20 hours per week (the maximum duration of sports-related activity according to NCAA bylaws). Team rosters as well as season start and end dates were obtained from publicly available schedules on the Pac-12 website (www.pac-12.com). Weekly training volume and season start and end dates for each sport were then confirmed by comparison with known NCAA and corresponding Pac-12 mandates regarding practice schedules, as documented with the intercollegiate athletics compliance office at our institution.
Statistical Analysis
All recorded injury-specific data elements were compared between the pre- and post-hiatus seasons. Subgroup analyses were performed by extremity (upper vs lower) as well as specific sport. Subgroup analyses were also performed on characteristics of knee and shoulder injuries among athletes competing in sports with historically high rates of knee (football, soccer, basketball, lacrosse, gymnastics) 11 or shoulder (football, wrestling, baseball, softball, volleyball) 2 injuries, respectively. Finally, the IR of fourth-quarter injuries (injuries that occurred in the fourth quarter of competition or final 25% of competition or practice), season-ending injuries, noncontact injuries, and overall injuries were compared between pre- and post-hiatus seasons for the 10 sports with the highest number of reported injuries overall.
The Pearson chi-square test was used to analyze all data consisting of categorical variables. A logistic regression model was used to conduct multivariate analyses with sex included as a covariate. All data were analyzed using Stata 12 software (StataCorp). P values <.05 were deemed as statistically significant.
Results
A total of 12,319 sports-related injuries across 23 sports were identified, with 7869 injuries in the pre-hiatus season and 4450 injuries in the post-hiatus season. Male athletes accounted for 60.3% of injuries in the prepandemic season compared with 62.5% of injuries in the postpandemic season (P = .022). The 10 sports with the highest number of reported injuries overall were football, basketball, track and field, soccer, rowing, volleyball, baseball, tennis, softball, and gymnastics. Overall, there was no difference in the incidence of injury between the pre-hiatus and post-hiatus seasons across all athletes captured in the database in aggregate.
Across all sports, the proportion of noncontact injuries was higher in the post-hiatus season than in the pre-hiatus season (46.1% vs 39.8%, P < .0001). The proportion of fourth-quarter injuries was also higher in the post-hiatus season compared with the pre-hiatus season (28.5% vs 25.9%, P = .015). There was no significant difference in the rate of requiring procedural intervention, rate of season-ending injury, proportion of nonacute injuries, or rate of recurrent injuries between the pre- and post-hiatus seasons (Table 1). Stratification by upper versus lower extremity yielded similar findings.
Pre- and Post-hiatus Injury Characteristics in Pac-12 Athletes a
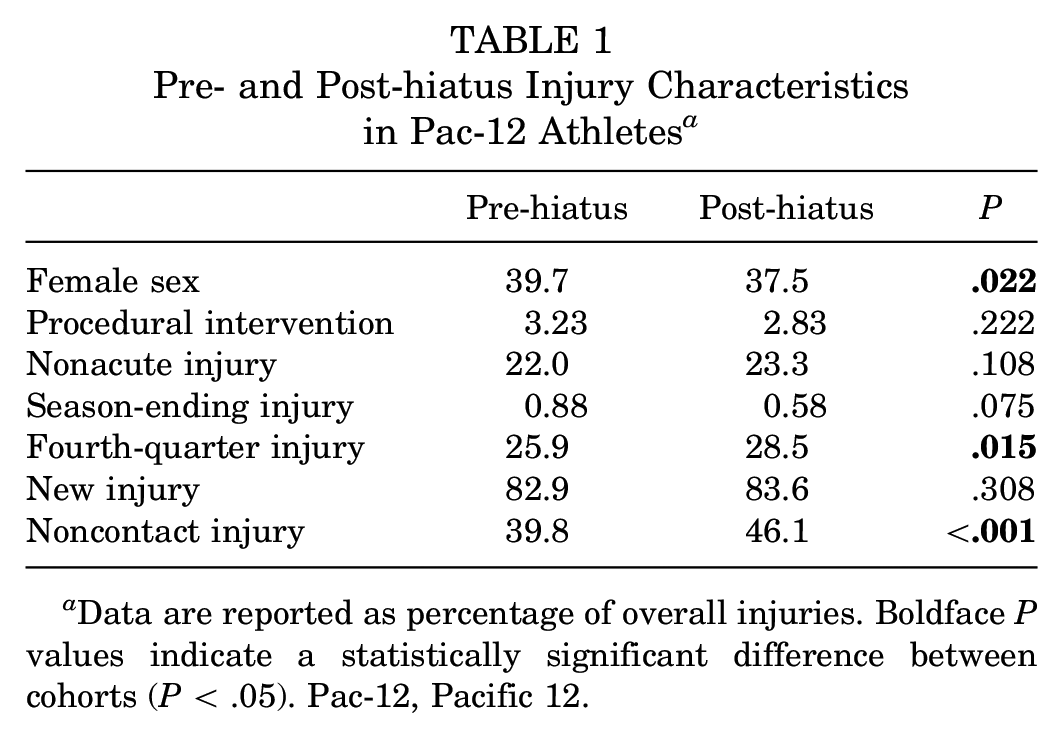
Data are reported as percentage of overall injuries. Boldface P values indicate a statistically significant difference between cohorts (P < .05). Pac-12, Pacific 12.
The proportion of upper extremity injuries sustained during the fourth quarter of competition or practice (26.8% vs 20.4%, P = .002) and the proportion of upper extremity noncontact injuries (30.1% vs 23.1%, P < .0001) were both found to be higher in the post-hiatus season. The proportion of noncontact lower extremity injuries was also higher in the post-hiatus season (59.9% vs 52.8%, P < .0001). No significant differences were noted with respect to proportion of nonacute injuries, recurrent injuries, season-ending injuries, or injuries requiring procedural intervention. Stratification by sport revealed higher proportions of nonacute injuries, noncontact injuries, and fourth-quarter injuries in the post-hiatus season for football players (Table 2).
Proportion of Nonacute, Noncontact, and Fourth-Quarter Injuries in the 10 Largest Pac-12 Sports a

Boldface P values indicate a statistically significant difference between cohorts (P < .05). Pac-12, Pacific 12.
In sports with traditionally high rates of knee injuries (football, soccer, basketball, lacrosse, gymnastics), higher proportions of nonacute knee injuries (21.2% vs 14.5%, P = .003) and noncontact knee injuries (47.6% vs 37.4%, P < .0001) were sustained in the post-hiatus versus pre-hiatus season. In sports with high rates of shoulder injuries (football, wrestling, baseball, softball, volleyball), higher proportions of nonacute shoulder injuries (25.3% vs 19.1%, P = .043), fourth-quarter injuries (27.7% vs 17.5%, P = .004), and noncontact shoulder injuries (34.3% vs 18.4%, P < .0001) were sustained in the post-hiatus season. No significant trends were found with respect to proportion of recurrent injuries, season-ending injuries, or injuries requiring procedural intervention.
Multivariate logistic regression analysis supported the univariate findings. Post-hiatus season was associated with significantly higher rates of noncontact injuries (OR, 1.64; P < .0001), nonacute injuries (OR, 1.41; P < .001), and fourth-quarter injuries (OR 1.21, P = .007). Female sex was significantly associated with nonacute injuries (OR, 2.29; P < .0001), noncontact injuries (OR, 2.19; P < .0001), season-ending injuries (OR, 2.39; P = .002), and decreased likelihood of procedural intervention (OR, 0.74; P = .050).
When comparing injury IRs between the pre- and post-hiatus seasons stratified by sport, there was a higher rate of injury in the pre-hiatus season among basketball, volleyball, and tennis athletes, yet there was a higher rate of injury in the post-hiatus season among soccer and rowing athletes. Of note, there was no significant difference in injury rates between these seasons among football, track and field, baseball, softball, or gymnastics athletes (Table 3).
In-season Injury Incidence Rate in the 10 Largest Pac-12 Sports a

Boldface P values indicate a statistically significant difference in injury rate between cohorts (P < .05). Pac-12, Pacific 12.
Expressed as total injuries per 1000 athlete-exposure hours during the season, excluding the preseason and postseason.
Discussion
In this study of injuries observed among intercollegiate athletes across a major athletic conference, there was no significant difference in the incidence of overall injury between the pre-hiatus and post-hiatus seasons. However, the proportion of noncontact injuries was higher in the post-hiatus season for football, baseball, and softball. Also increased in the post-hiatus season was the proportion of nonacute injuries among football, basketball, and rowing athletes, as well as the overall proportion of injuries sustained by football players in the final quarter of competition or practice. Furthermore, compared with the season immediately preceding the COVID-19 pandemic, athletes competing in the postpandemic season were observed to have a higher rate of noncontact injuries and injuries near the end of competition (Table 1).
In our study, we assumed that the hiatus resulted in detraining. The negative impacts of detraining (a partial or complete loss of training-induced adaptations because of insufficient or inappropriate training stimuli) on athletic performance and injury risk have been demonstrated in numerous studies in the past3,19,25 and prompted some sports medicine practitioners to offer recommendations for athletes to help prevent deconditioning.10,31 Parallels have been made to other isolated incidences of long-term detraining, such as the NFL lockout, 22 but no studies have summarized the pandemic’s impact on injury timing and mechanism across a wide variety of sports at the elite intercollegiate level. As a result, our epidemiologic characterization of athlete injury risk profiles upon return to sports may be more applicable to a broader population of athletes and may help guide decisions regarding athlete workload upon the resumption of training.
This study evaluates a large collection of sports injury data across a multitude of different sports among high-level intercollegiate athletes both before and after the COVID pandemic. Although some authors have reported an increase in injury rate among athletes from specific sports after a COVID-19 pandemic–associated interruption of play, our study did not identify an overall increase in injury rate post-hiatus across all Pac-12 sports. Sports with higher injury incidence post-hiatus included soccer, women’s rowing, men’s volleyball, baseball, and softball. Sports with a lower injury incidence post-hiatus included basketball, women’s track, and tennis. Yet, no differences in injury rates were seen among football, track, or gymnastics athletes. The increased injury rate observed among Pac-12 soccer athletes in the post-hiatus season is concordant with the findings reported by Seshadri et al. 32 However, our results demonstrating no significant increase in overall injury rates post-hiatus among Pac-12 football players are distinct from the results reported by Myer et al, 22 who found an increased rate of Achilles injuries among NFL athletes. Our data suggest that these post-COVID changes may be sports specific or due to particular return-to-play paradigms partly imposed by the Pac-12 Conference, with further adjustments by the coaching staff of individual teams.
The timing and scheduling of sports seasons post-hiatus may also have contributed to the lack of change in injury rates observed among Pac-12 athletes. While formal practices were allowed to resume beginning in the fall of 2020, many fall sports such as soccer, swimming, and field hockey had their competition seasons delayed to 2021. 27 Seshadri et al 32 had investigated injury rates immediately after the COVID pandemic’s disruption of play in the Bundesliga, which matches as early as May 15, 2020, just 2 months after the league had suspended play in mid-March 2020. It is possible that the time period between November 2020 and spring 2021, when competition had not yet started but facilities had reopened, allowed the collegiate athletes who participated in fall sports (eg, men’s and women’s soccer, men’s water polo) more time to acclimate. In contrast to this acclimatization concept, Pac-12 football athletes, who were subject to only a relatively short delay to the start of their truncated fall 2020 season, 26 were found to have no increase in the rate of in-season injuries. In any case, our results and a review of the currently available relevant literature indicate that the pandemic has had varied effects on athletes from different sports within the intercollegiate athlete population.
Athlete age and experience may also have influenced injury rates. Our population of intercollegiate athletes is generally younger and has less playing experience than the professional athletes included in the Bundesliga or NFL. Rogalski et al, 29 in their study of Australian Football League athletes, reported that for any given training load, older athletes were at greater risk of injury than their younger teammates. Other studies have also provided evidence to suggest that the human body’s ability to tolerate rapid changes of force and recover from fatigue may decline with age.18,36 Older, experienced athletes are also more likely to have sustained previous injuries, which is another well-characterized factor associated with an increased risk of future injury. 6 Thus, the presumed increased likelihood of prior injury and decreased recovery capacity for strenuous training loads may contribute to the observed differences between our findings and those of prior studies.
Football and basketball athletes experienced a higher proportion of nonacute injuries after the post-hiatus period. This observation may be explained by literature describing how changes in an athlete’s workload can influence the risk of injury (ie, nonacute injuries). For example, increases in training volume, especially over a short period of time, have also been associated with an increased risk of nonacute injury.7,17 Furthermore, rapid increases in training intensity (ie, workload) also can increase the risk of injury. Even among collision sports athletes, players who exceed a prescribed weekly training load were noted to be up to 70 times more likely to experience a noncontact soft-tissue injury.7,8 Although we do not have workload data for each specific team, in the post-hiatus shortened return-to-play timeframe teams may have exposed athletes to a more rapid increase in training volume (ie, an increased acute-to-chronic workload ratio) in an attempt to achieve historically appropriate training volumes before resuming competition. In addition to these training workload changes, the truncated competition season resulted in a more congested competition schedule, including the loss of a bye week during football season, resulting in reduced recovery time between periods of high-intensity competition workloads. Bengtsson et al 1 found that football players with fewer days of recovery between matches were noted to have a significantly higher rate of hamstring and quadriceps injuries than players experiencing a longer recovery period. In addition, planned recovery time and training schedules were impacted by unpredictable cancellations as multiple competitions across multiple sports throughout the conference had to be rescheduled last minute because of COVID-19 outbreaks.
Analogous to the concept of acute-to-chronic workload changes, decreased preseason strength may further contribute to the observed changes in injury mechanism among baseball players. Associations between decreased preseason shoulder strength and increased risk of upper extremity injury have been reported in both adolescent and professional baseball athletes.4,34,35 Although preseason condition was not recorded in the Pac-12 HAP data set, it is plausible that athletes who had limited access to strength training facilities during the hiatus may have had decreased upper extremity strength upon resumption of training.
Another interesting finding in this study is the higher proportion of injuries sustained by football players during the fourth quarter of competitions or practices in the post-hiatus season compared with the pre-hiatus season. Most studies exploring the timing of injury have reported that more injuries occur in the second half of competitions, and in events divided into quarters, that injuries occur more frequently during the second and third quarters.5,12,23 Nagle et al 23 observed that although severe lower extremity injuries tended to occur early during games in most sports, most overall injuries occurred in the second half of practice or matches, possibly because of player fatigue. Cloke et al 5 found that ankle injuries among high school soccer players tended to increase toward the end of each half of a match, which was again attributed to poor endurance. The authors also noted that injuries were more prevalent in January and August after students returned to play after a school break. These findings, as discussed previously, further suggest that athletes may fatigue more easily because of deconditioning, and this fatigue may contribute to an increased risk of injury. Thus, the deconditioning experienced by athletes during the hiatus may have resulted in more pronounced injury risk in the final quarter of play.
It is worth noting that an athlete’s risk of injury has been associated with several factors, including sex, age, training load, and sports specialization, and each of these factors should be considered when designing training protocols that not only prepare athletes for competition but also prevent injury.13,28 An athlete’s experience level, the effects of detraining, and an athlete’s response to the return-to-play workload after a period of detraining can each impact individual athletes differently.
Limitations
While our study offers a comprehensive summary of the impact that the COVID pandemic has had on high-level intercollegiate athletes, there are several noteworthy limitations. First, as noted above, we assume that loss of access to organized training and institutional training facilities did, in fact, lead to detraining; however, we lack any objective evidence of training levels during the hiatus. It is possible that athletes kept up or even surpassed their pre-hiatus fitness and skill levels via alternative training practices. It is also worth noting that some of our findings, while statistically significant, may not be clinically significant. For example, the proportion of fourth-quarter injuries being 28.5% in the post-hiatus season compared with 25.9% in the pre-hiatus season may not be of any significance clinically, as these values are quite similar. Furthermore, this is a retrospective study of data collected and entered by individuals from a variety of backgrounds (including physical therapists, certified athletic trainers, sports performance personnel, and physicians); thus, there are potential inaccuracies and/or inconsistencies concerning certain features of a given injury or diagnostic criteria.
Another shortcoming is the categorization of injury chronicity in the Pac-12 HAP database. Injuries are recorded as “chronic” if symptoms have been present >24 hours after the inciting event. This is an inherently flawed definition that may include truly acute injuries that were not reported within 24 hours. This can lead to a falsely elevated number of “chronic” injuries that may more aptly be characterized as acute or subacute, making the distinction between truly acute and more chronic injuries challenging. In response to this shortcoming, we used the term “nonacute” for all injuries that were not reported within 24 hours. In addition, in an effort to protect patient confidentiality, the specific date of injury was not included in the data set we analyzed. As a result, we are unable to determine exactly when in the season the observed injuries occurred, which has implications related to contributing injury risk factors such as training volume and acute-to-chronic workload ratio. Furthermore, given that we had estimated athlete-exposure values based on assumptions related to NCAA regulations, there is the potential for error in our quantification of athlete-exposures. Although the Pac-12 has funded ongoing research investigations of using modalities such as ultrasound imaging of Achilles tendons to detect precursors of injury and the use of enhanced documentation of nonacute injuries, the exact institutional and sports-specific return-to-play protocols are unknown; thus, comparisons and analysis of this factor was not possible. Despite these weaknesses, the multicenter comprehensive data capture using a uniform database framework makes this investigation a valuable contribution to our knowledge of athletic injury epidemiology associated with the COVID-19 pandemic.
Conclusion
While there was no significant change in the observed overall injury rate between the pre- and post-hiatus seasons in our data set, athletes competing in the post-hiatus season were observed to have a higher rate of noncontact injuries and injuries sustained in the fourth quarter of competition. There were no significant differences between the pre- and post-hiatus seasons with respect to proportion of recurrent injuries, season-ending injuries, or injuries requiring procedural intervention. This study demonstrates that the COVID-19 pandemic has had varied effects on athletes from different sports, suggesting that many factors must be considered when designing return-to-sports programs (or prescribed time away from sports participation) for athletes after an extended absence from organized training.
Footnotes
Acknowledgements
The authors thank the Pac-12 Health Analytics Program data custodians, including Kevin Robell, MA, ATC, for their assistance with review of the available data elements and for providing the data set used in this study. In addition, the authors thank the numerous certified athletic trainers, undergraduate volunteers, physical therapists, sports performance personnel, physicians, and other allied health team members for their invaluable contributions to this work through the input of the health event data points captured in the Pac-12 Health Analytics Program database.
Final revision submitted December 12, 2022; accepted January 24, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: Research support was provided by the US Department of Veterans Affairs (grant IK2BX005199 to T.J.K.). T.J.K. has received education payments from Micromed, consulting fees from Heron Therapeutics, honoraria from Fidia Pharma and Musculoskeletal Transplant Foundation, and hospitality payments from RTI Surgical. A.U.-B. has received hospitality payments from Globus Medical and Zimmer Biomet. K.J.J. has received education payments from Arthrex and Micromed; consulting fees from Linvatec; nonconsulting fees from Arthrex; honoraria from JRF Ortho, Musculoskeletal Transplant Foundation, and Vericel; and hospitality payments from Aesculap and DePuy. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto. Ethical approval for this study was waived by the University of California at Los Angeles (reference No. 21-000540).