
Abstract
Background:
Many clinicians release patients to return to activity after anterior cruciate ligament reconstruction (ACLR) based on time from surgery despite deficits in muscle strength and function. It is unclear whether symmetry or unilateral performance is the best predictor of subjective outcomes after ACLR.
Purpose:
To determine physical performance predictors of patient-reported outcomes after reconstruction.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
A total of 88 participants (49 males, 39 females; mean ± SD height, 174.0 ± 9.6 cm; weight, 76.1 ± 18.5 kg; age, 19.4 ± 3.7 years) who underwent primary, unilateral ACLR volunteered for this study. Participants had undergone reconstruction a mean of 6.9 ± 1.8 months (range, 5.0-14.1 months) before the study. All participants underwent strength testing as well as hop testing and then completed the International Knee Documentation Committee (IKDC) and Knee injury and Osteoarthritis Outcome Score (KOOS) questionnaires. Stepwise linear regression models were used for symmetry and unilateral performance to identify the proportion of variance explained in the IKDC score, KOOS total score, KOOS-sport subscale, and time from surgery, as well as receiver operating characteristic (ROC) curve analyses on those variables that explained the most variance in patient-reported outcomes to determine cutoff thresholds.
Results:
No significant correlations were found between time from surgery and objective performance. The only significant predictors of IKDC score were single-hop limb symmetry index (LSI) and age (R 2 = 0.177) and unilateral triple-hop performance and age (R 2 = 0.228). The cutoff for single-hop symmetry was 0.92 (area under the curve [AUC], 0.703; P = .012), and the cutoff for normalized triple-hop distance was 3.93 (AUC, 0.726; P = .005). When stratified by age, the cutoff for single-hop symmetry was 0.81 (AUC, 0.721; P = .051) for younger patients (age <19.1 years) and was not significant for older patients (age ≥19.1 years). The cutoff for normalized triple-hop distance was 3.85 (AUC, 0.832; P = .005) in older patients and was not significant for younger patients. The only significant predictors of KOOS-sport subscale were single-hop LSI (R 2 = 0.140) and normalized knee extensor power at 180 deg/s (R 2 = 0.096). When subjective outcomes were predicted based on KOOS-sport subscale, the cutoff for single-hop symmetry was 0.85 (AUC, 0.692; P = .018).
Conclusion:
Hopping performance is the most predictive functional variable of subjective outcomes after reconstruction. Single-hop symmetry was most important for younger patients and unilateral triple-hop distance was most important for older patients. Clinicians should consider hopping performance when making return-to-activity decisions after ACLR.
Approximately 130,000 anterior cruciate ligament reconstructions (ACLRs) are performed annually in the United States. 22 This surgery remains the gold standard for treatment of primary anterior cruciate ligament (ACL) injuries, as approximately 98% of surgeons recommend ACLR in athletes who desire to return to sport. 23 Approximately 81% of athletes return to sport; however, only 65% return to their preinjury level and 55% return to a competitive level. 3 Patient characteristics including younger age, elite sport, male sex, and positive psychological response favor a return to preinjury level of activity. Unfortunately, this population of patients who return to high-level activity have 6 times the risk of a second ACL injury within 2 years after their surgery. 30
More than half of orthopaedic surgeons indicate time since surgery as a part of their return-to-activity criteria, and in some cases, 6 months following surgery is the only determinant. 7,11,13 Objective criteria, including isokinetic muscle strength, dynamic function (ie, single-leg hop tests), range of motion, presence of an effusion, stability testing, and validated patient-reported outcome questionnaires, have been reported in only 13% of studies regarding return-to-activity decision-making, 7 despite information suggesting that increased quadriceps strength symmetry and time from surgery decrease the risk of reinjury. 10 Along with decreased risk of reinjury, increased subjective and objective function has been associated with increased patient satisfaction after ACLR. 19
Clinicians who use objective measures often compare the involved limb with the contralateral limb for a measure of limb symmetry. 8,35 Patients present with knee extensor strength asymmetry after injury and at 6 months after reconstruction, 9,18 and these deficits have been identified in both isometric and isokinetic movements. 15,18,29,39,42 Quadriceps strength asymmetry has been associated with decreased subjective function after ACLR, 42 suggesting that high patient-reported outcome scores may be predictive of symmetrical quadriceps strength. However, asymmetry is also present in functional tasks that require explosive power in the quadriceps, such as single-leg hop for distance. 25 It is currently unclear whether asymmetry in strength or functional performance, or a combination of measures, best predicts patient-reported outcomes after ACLR. Therefore, the purpose of this study was to determine physical performance predictors of patient-reported outcomes after reconstruction. The information may inform surgeons making return-to-activity recommendations for individual patients by determining threshold values on functional tests for good patient-reported outcomes.
Methods
Participants
Eighty-eight participants (49 males, 39 females; mean ± SD height, 174.0 ± 9.6 cm; weight, 76.1 ± 18.5 kg; age, 19.4 ± 3.7 years) with a primary, unilateral ACLR volunteered for this study. Preinjury level of activity was not recorded.
Participants had undergone reconstruction a mean of 6.9 ± 1.8 months (range, 5.0-14.1 months) before the study, receiving either an ipsilateral patellar tendon autograft (n = 65) or a hamstring tendon autograft (n = 23), and they completed testing before clearance to return to activity. Any patient with a contralateral graft harvest, allograft, or other concomitant ligament injury including medial collateral ligament, posterior cruciate ligament, or lateral collateral ligament tear was excluded from the study. Patients completed physical therapy according to their surgeon’s recommendation, and this was not recorded or controlled. All patients completed testing around the time of clearance to return to unrestricted activity.
Procedures
All participants came to the laboratory for a single session wearing athletic clothing and shoes. After providing written informed consent approved by the university’s institutional review board for health sciences research, participants completed a 5-minute warm-up walking on the treadmill at a self-selected speed. After the warm-up, participants were seated in the Biodex System III dynamometer chair (Biodex Medical Systems) in approximately 85° of hip flexion, and the axis of the dynamometer was aligned to the lateral femoral epicondyle in line with the sagittal plane knee joint center. The distal end of the dynamometer arm was secured to the distal shank with a padded Velcro strap. Range of motion was set from approximately 0° to 110° of knee flexion for isokinetic testing. Participants crossed their hands on their shoulders and kept their head and shoulders back against the chair; a belt was then secured over the participant’s lap. Participants completed practice trials before completing 8 concentric repetitions of knee extension and knee flexion at 90 deg/s followed by 8 concentric repetitions of knee extension and knee flexion at 180 deg/s, with 45 seconds of rest between each set. The tester provided encouragement throughout the test to ensure the participants were providing maximal effort.
Following isokinetic testing, participants completed isometric testing at 90° of knee flexion. Participants were instructed to isometrically extend their knee maximally and maintain the contraction for 5 seconds. No visual or auditory feedback was provided during isometric contractions. Following the maximal voluntary isometric quadriceps contraction, participants were instructed to isometrically flex their knee maximally for 5 seconds. The maximal 1-second average from the contraction was recorded as the maximal isometric contraction by use of AcqKnowledge software (Biopac Systems). Participants completed all testing on the uninvolved limb before completing testing on the involved limb. Peak torques, average torques, total work, and average power were mass-normalized and presented as a limb symmetry index (LSI) by dividing the involved limb by the uninvolved limb.
After strength testing, participants completed 3 single-leg hopping tasks: the single hop for distance, triple hop for distance, and crossover hop for distance. 28 Participants were instructed to hop as far as possible, complete 3 consecutive hops for maximal distance (triple hop), and complete 3 consecutive zig-zag hops for maximal distance crossing over a 15-cm-wide line on each hop (crossover hop). Practice trials were encouraged to minimize a learning effect. All participants completed 3 trials on each leg, starting with the uninvolved leg and alternating to the involved leg, and the average distance of the 3 trials was calculated. Distance was measured from the start line to the participant’s heel. If participants were unable to hold the single-leg landing, the trial was disregarded and repeated. Participants were encouraged to rest between trials to minimize the effect of fatigue. Hop distances were converted to LSI by dividing the distance hopped on the involved limb by the distance hopped on the uninvolved limb. Hop distances on the involved limb were normalized to leg length, defined as the distance from the anterior superior iliac spine to the medial malleolus. 26 Following testing, all participants completed the International Knee Documentation Committee (IKDC) subjective knee evaluation form 2,14 and the Knee injury and Osteoarthritis Outcome Score (KOOS). 36,37 The KOOS-sport subscale was included in analyses because it measures subjective function on some of the most functional tasks, including squatting, running, jumping, twisting, pivoting, and kneeling.
Statistical Analyses
Bivariate Pearson correlations were calculated to identify relationships among patient-reported outcomes (IKDC and KOOS) and objective measures of function. Isokinetic strength outcomes included mass-normalized peak torque, average torque, total work, and average power for knee extension and flexion. Isometric strength outcomes included mass-normalized peak torque for knee extension and flexion. Mass-normalized variables were presented as LSI, where 1 represents perfect symmetry and 0 represents no symmetry. Functional measures included average hop distance on the single, triple, and crossover hop for distance. Distances were presented as LSI as well as normalized to leg length for the involved limb. Age and sex were also correlated with patient-reported outcomes. All significant correlations (P < .05) were retained for a multiple regression analysis.
A stepwise linear regression model was used to identify the proportion of variance explained by the IKDC (model 1), KOOS total score (model 2), KOOS-sport score (model 3), and time from surgery (model 4) for all LSI measures. Stepwise linear regression models were used for normalized performance on the involved limb to identify the proportion of variance explained by the IKDC (model 5), KOOS total score (model 6), KOOS-sport score (model 7), and time from surgery (model 8). We performed receiver operating characteristic (ROC) curve analyses on those variables that explained the most variance in patient-reported outcomes to determine cutoff thresholds. We used previously published thresholds for the KOOS-sport (75.0) and IKDC (75.9) 24 to stratify the patients. A successful outcome was defined as patients who scored greater than the published thresholds. Only those ROC curves that were statistically significant were evaluated for cutoff thresholds. We reported area under the curve (AUC) (which ranges from 0.5 = random guess to 1.0 = perfect predictive ability), sensitivity, and specificity for all significant ROC curves. The significance level was set a priori at P ≤ .05 to enter the regression model. All analyses were run by use of SPSS (version 24.0; SPSS Inc).
Results
Limb Symmetry Index
Means and standard deviations for all patient-reported outcomes, strength, and hopping performance are reported in Table 1.
Means and Standard Deviations for All Patient-Reported Outcomes, Strength Symmetry, Hopping Symmetry, Involved Limb Strength, and Involved Limb Hopping Performance a

a Limb symmetry was calculated as the involved limb (the limb that had anterior cruciate ligament reconstruction) divided by the uninvolved limb (contralateral). All involved limb strength values were normalized to body mass (kg), and hopping was normalized to leg length (cm). A symmetry value of 1.0 was interpreted as perfect symmetry and a value less than 1.0 indicates the uninvolved limb outperformed the involved limb. IKDC, International Knee Documentation Committee Subjective Knee Evaluation Form; KOOS, Knee injury and Osteoarthritis Outcome Score.
No significant correlations were found between time from surgery and any strength or hop LSI (P = .133-.991). As well, no significant correlations were found between time from surgery and IKDC, KOOS total, or KOOS-sport scores (P = .137-.455). The only significant correlations with IKDC were age (r = –0.243, P = .002), single-leg hop for distance (r = 0.346, P = .002), triple hop for distance (r = 0.282, P = .011), and average knee extensor power at 180 deg/s (r = 0.222, P = .038). These 4 variables were entered into the stepwise linear regression model, and age and single-leg hop symmetry were retained in the model (P = .022); this explained 17.7% of the variance in IKDC score (Table 2).
Final Stepwise Regression Models in Patients After Anterior Cruciate Ligament Reconstruction a
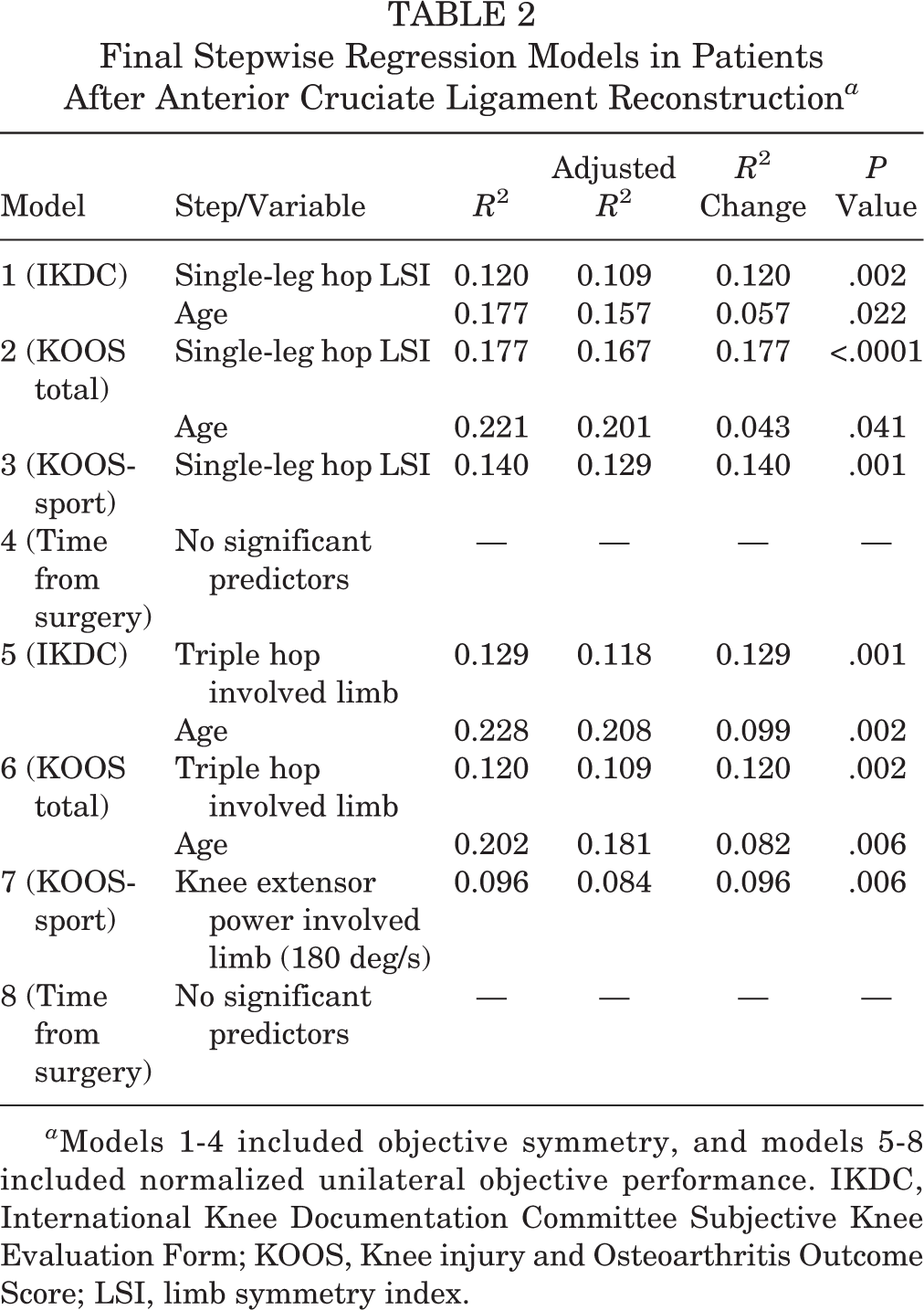
a Models 1-4 included objective symmetry, and models 5-8 included normalized unilateral objective performance. IKDC, International Knee Documentation Committee Subjective Knee Evaluation Form; KOOS, Knee injury and Osteoarthritis Outcome Score; LSI, limb symmetry index.
Ten symmetry variables were significantly correlated with KOOS total score, including age, average knee extensor power at 90 and 180 deg/s, average knee flexor power at 90 and 180 deg/s, peak and average knee flexor torque at 90 deg/s, total knee flexor work at 90 deg/s, single-leg hop, and triple hop for distance (Table 3). When these variables were entered into the stepwise linear regression model, the only 2 variables remaining in the model were age and single-leg hop for distance (P < .041), which explained 22.1% of the variance in the KOOS total score (Table 2).
Correlation Coefficients and Associated P Values for Relationship Between KOOS Total Score and Functional Performance Symmetry and Unilateral Measures a

a Boldfaced values indicate statistical significance (P < .05). KOOS, Knee injury and Osteoarthritis Outcome Score.
Fifteen symmetry variables were significantly correlated with the KOOS-sport score, including peak and average knee extensor torque at 90 and 180 deg/s, peak and average knee flexor torque at 90 deg/s, average knee extensor and flexor power at 90 and 180 deg/s, total knee extensor and flexor work at 90 deg/s, total knee extensor work at 180 deg/s, single-leg hop, and triple hop for distance (Table 4). These variables were entered into the stepwise linear regression model, and the only variable retained in the model was single-leg hop symmetry (P = .001), which explained 14.0% of the variance in the KOOS-sport score (Table 2).
Correlation Coefficients and Associated P Values for Relationship Between KOOS-Sport Score and Functional Performance Symmetry and Unilateral Measures a

a Boldfaced values indicate statistical significance (P < .05). KOOS, Knee injury and Osteoarthritis Outcome Score.
Cutoff thresholds were calculated for single-hop symmetry and age using IKDC score higher than 75.9 and KOOS-sport score higher than 75.0 to define successful outcomes. When IKDC was used, the cutoff threshold for single-hop symmetry was 0.92 (AUC = 0.703, sensitivity = 0.5231, specificity = 0.750, P = .012) and for age the threshold was 19.1 (AUC = 0.338, sensitivity = 0.400, specificity = 0.500, P = .045). Using this age threshold of 19.1 years, we then stratified patients by age to compare single-hop symmetry cutoffs on the IKDC based on age. The cutoff threshold for single-hop symmetry for younger patients (age <19.1, n = 49) was 0.81 (AUC = 0.721, sensitivity = 0.897, specificity = 0.625, P = .051). For older patients (age ≥19.1, n = 39), the cutoff threshold for single-hop symmetry was 0.87 (AUC = 0.683, sensitivity = 0.731, specificity = 0.625, P = .123). When predicting successful outcomes based on the KOOS-sport subscale, the cutoff score for single-hop symmetry was 0.85 (AUC = 0.692, sensitivity = 0.769, specificity = 0.625, P = .018).
Unilateral Performance
No significant correlations were noted between time from surgery and any of the unilateral measures (P = .137-.666). Thirteen variables were significantly correlated with the IKDC, including age, peak and average knee extensor torque at 90 and 180 deg/s, average knee extensor power at 90 and 180 deg/s, total knee extensor work at 90 and 180 deg/s, peak knee extensor isometric torque, single-leg hop, triple hop, and crossover hop for distance. These variables were entered into the stepwise linear regression model, and the only variables retained in the model were normalized triple-hop distance and age (P = .002), which explained 20.8% of the variance in the IKDC.
Eighteen variables were significantly correlated with KOOS total score, including age, peak and average knee extensor torque at 90 and 180 deg/s, average knee extensor power at 90 and 180 deg/s, total knee extensor work at 90 and 180 deg/s, peak knee extensor isometric torque, average knee flexor torque at 90 and 180 deg/s, total knee flexor work at 90 deg/s, average knee flexor power at 90 and 180 deg/s, single-leg hop, triple hop, and crossover hop for distance (Table 3). When these variables were entered into the stepwise linear regression model, the only 2 variables remaining in the model were age and single-leg hop for distance (P = .006), which explained 18.1% of the variance in the KOOS total score (Table 2).
Thirteen variables were significantly correlated with the KOOS-sport score, including peak and average knee extensor torque at 90 and 180 deg/s, average knee extensor power at 90 and 180 deg/s, total knee extensor work at 90 and 180 deg/s, peak knee extensor isometric torque, average knee flexor power at 180 deg/s, single-leg hop, triple hop, and crossover hop for distance (Table 4). These variables were entered into the stepwise linear regression model, and the only variable retained in the model was normalized knee extensor power at 180 deg/s (P = .006), which explained 9.6% of the variance in the KOOS-sport score (Table 2).
Cutoff thresholds were calculated for normalized triple hop, age, and normalized knee extensor power for IKDC and KOOS-sport to define successful outcomes. When IKDC was used, the cutoff threshold for triple hop was 3.93 (AUC = 0.726, sensitivity = 0.800, specificity = 0.4377, P = .005) and for age the threshold was 19.1 (AUC = 0.338, sensitivity = 0.400, specificity = 0.500, P = .045). Using this age threshold of 19.1 years, we then stratified patients by age to compare single-hop distance cutoffs on the IKDC based on age. The cutoff threshold for the triple hop on the involved limb for younger patients (age <19.1, n = 49) was 4.21 (AUC = 0.657, sensitivity = 0.615, specificity = 0.625, P = .165). For older patients (age ≥19.1, n = 39), the cutoff threshold for triple hop on the involved limb was 3.85 (AUC = 0.832, sensitivity = 0.885, specificity = 0.500, P = .005). When predicting successful outcomes based on KOOS-sport, the cutoff score for normalized average knee extensor power was 2.09 (AUC = 0.636, sensitivity = 0.5735, specificity = 0.6111, P = .078).
Discussion
One of the most common criteria used when returning patients to sport after ACLR is time from surgery 7,11 ; however, in the current study we found no correlation between time from surgery and functional performance, strength, or LSI. These findings are supported by previous studies which noted that deficits in unilateral force and potential energy absorption are independent of time from surgery. 4,27 Although strength is independent of time, performance on functional tasks improves with time, with nearly all results greater than 90% at 12 months post-ACLR 1 and decreased risk of reinjury at 9 months post-ACLR, 10 suggesting that increased performance on functional tests was predictably seen as time increased following surgery. All patients in the current study were at least 5 months postsurgery, and more deficits may be present in a cohort less than 5 months postsurgery. This agrees with the findings from our current study where, on average, hopping symmetry greater than 85% to 90% was identified as a cutoff threshold for successful patient-reported outcomes and return to sport. 10 Reduced patient-reported outcome scores have previously been associated with inability to return to activity, 21 suggesting that this value may be useful to clinicians when using objective hopping data to guide return-to-play decision-making.
Hop testing is one of the most commonly reported functional tests following ACLR. 1 In the current study, single-leg hop symmetry and normalized triple-hop distance on the involved limb were the most predictive functional tests of subjective outcomes in the first 5 to 14 months following reconstruction. Single-hop symmetry was the most predictive of subjective outcomes in individuals younger than 19 years, while normalized triple-hop distance on the involved limb was most predictive of subjective outcomes in older individuals. Younger patients may perceive involved limb function through comparison to the uninvolved limb, while older patients may focus more on unilateral performance to assess function. Some evidence suggests that strength and gait asymmetry may be present in individuals who are college-aged and older 33,34 ; thus, these patients may not perceive asymmetry as decreased function. Establishing symmetry may therefore be more important in younger patients after ACLR, while unilateral performance on a more demanding task is more important for patients older than 19 years.
Interestingly, the cutoff point for single-hop symmetry in these middle school–age and high school–age individuals was much lower (81.0%) compared with when all individuals were included in analyses (92.0%). Although a lower LSI was predictive of higher subjective function in these young individuals, our findings may suggest that a combination of functional and subjective outcomes should be used when clinicians and athletes are making decisions about return to activity, considering that subsequent ACL injury is increased for patients younger than 19 who return to a high level of sport. 12,16,17,38 These young patients may report better subjective function faster after surgery and may perceive better function despite deficits in performance. The IKDC threshold used in this study was based on acceptable symptom state, 24 which may suggest that although perceived symptoms are resolved, this threshold may not necessarily indicate readiness to return to activity. A combination of good subjective knee function along with more symmetrical hop performance is associated with return to preinjury level of activity, 6 supporting a multifactorial approach to return-to-activity decision-making in young, active individuals after ACLR.
Asymmetrical hop performance may also suggest asymmetry in knee extensor power after ACLR. 18 Individuals with ACLR often present with asymmetry in power movements, such as unilateral vertical jump. 15,27,41 This was further supported in our study considering that the only unilateral measure that was significantly correlated with the KOOS-sport score was normalized knee extensor power, with a cutoff score of 2.09 W/kg; however, this threshold was not statistically significant. Normalized knee extensor torque greater than 3.00 N·m/kg has been previously identified as a threshold for good patient-reported outcomes after ACLR 20 ; however, this threshold was established in an older patient population (mean age, 22.5 years) who were 31.5 months postreconstruction. The current study suggests that unilateral triple-hop performance may be a better predictor for subjective outcomes in this age group at the time when a decision to return to sport is made.
Although asymmetry in isokinetic strength testing was apparent in our study (Table 1), the side-to-side difference was not a significant predictor of subjective function. Another study, however, has reported that quadriceps strength symmetry is able to identify patients with an IKDC index of 90% and has suggested that rehabilitation guidelines may benefit from incorporating quadriceps strength to predict participants with high self-reported function. 32 IKDC score has also been reported to be a predictor of quadriceps strength, function, and symmetry. 42 Individuals with IKDC scores above 90 were 3 times more likely to demonstrate higher quadriceps LSI, and IKDC score of 94.8 predicted quadriceps LSI 90% with high sensitivity (0.813) and moderate specificity (0.493). 42 These studies did not include hop performance; however, hop performance has been positively correlated with knee extensor strength 31 and therefore may be appropriate to measure quadriceps strength along with subjective function.
The current study has limitations. The regression models in the study indicate that small proportions of variance were explained in patient-reported outcomes by single-leg hop performance. This also indicates that a large proportion of variance in patient-reported outcomes was not explained by the variables included in the regression models, suggesting that factors other than those measured in this study may influence the ability to predict patient-reported outcomes after ACLR. The cutoff thresholds calculated in the current study were associated with AUC values ranging from 0.65 to 0.85; this means that the predictive ability of these cutoff values is not perfect and suggests that other factors contribute to subjective outcomes after ACLR. In addition, this study did not consider kinesiophobia, which may be a contributing factor in return to sport. 5,21,40 Assessment of kinesiophobia along with hopping performance around time of clearance to activity after ACLR may help identify patients with poor outcomes. 21 Future studies should consider including a measure of kinesiophobia when predicting subjective function after ACLR. Another limitation in the current study was that patients represented a nonhomogeneous group including a range of individual activity goals, different rehabilitation protocols, and different surgical techniques. Future studies in this area should separate athletes from recreationally active individuals as well as differentiate between athletes returning to pivoting/cutting sports and athletes returning to other sports to compare differences in outcomes after ACLR. The current study did not include prospective data confirming optimal outcome after ACLR. Further research should include prospective analyses to confirm return-to-activity and reinjury rates. Last, the current study did not randomize testing procedures, always testing the uninvolved limb before the involved limb and completing patient-reported outcomes after hopping. This was a deliberate study design to introduce all procedures on the uninvolved limb first as well as to ensure that outcome scores reflected perceived performance and function from the current session.
Conclusion
Hopping performance is correlated with patient-reported outcomes in patients with ACLR around 6 months after reconstruction. Single-leg hop symmetry is the most predictive functional variable for patient-reported outcome from 5 to 14 months after reconstruction. Single-hop symmetry was the most predictive of subjective function in younger patients, while unilateral triple-hop distance was the most predictive of subjective function in older patients. Hopping symmetry greater than 85% to 90% may be a useful threshold for good subjective outcomes; however, clinicians should also consider other factors, such as age and sport, when making return-to-activity recommendations.
Footnotes
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution.
Ethical approval for this study was obtained from the University of Virginia Institutional Review Board for Health Sciences Research (HSR No. 17399).