
Abstract
Background:
Mechanoreceptors in the posterior cruciate ligament (PCL) can produce proprioception, which is an important reason why patients choose cruciate-retaining total knee arthroplasty (TKA). The number of mechanoreceptors in the PCL of patients with knee osteoarthritis (OA) is unknown.
Purpose:
To provide a theoretical basis for estimating the number of mechanoreceptors in the PCL by evaluating the relationship between this number and patient age or OA severity.
Study Design:
Cross-sectional study; Level of evidence, 3.
Methods:
An overall 28 PCLs from patients with knee OA were collected at the time of TKA and grouped according to patient age (group A, 60-69 years [n = 8]; group B, 70-79 years [n = 12]; group C, ≥80 years [n = 8]) and OA based on Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) score (group I, ≤80 [n = 8]; group II, 81-120 [n = 10]; group III, >120 [n = 10]). Hematoxylin and eosin and S-100 immunohistochemical staining were performed on the slices near the tibial attachment of the PCL, and the number of mechanoreceptors in each slice was counted. Multifactor analysis of variance was used to evaluate the relationship between the number of mechanoreceptors and patient age or WOMAC score.
Results:
The number of mechanoreceptors (mean ± SD) in groups A, B, and C was 24.00 ± 15.19, 30.92 ± 11.41, and 23.38 ± 11.39, respectively, with no significant between-group differences. The number of mechanoreceptors in groups I, II, and III was 43.50 ± 4.99, 25.00 ± 5.27, and 15.20 ± 5.61, with significant differences between groups I and II, groups I and III, and groups II and III (P < .001 for all).
Conclusion:
In patients with knee OA, age had no significant effect on mechanoreceptor count, but the number of mechanoreceptors in the PCL decreased significantly with higher (worse) WOMAC score. These findings suggest that in patients of any age with high WOMAC scores, there may be little value as it relates to knee proprioception in performing a PCL-retaining TKA.
Keywords
As one of the most common chronic diseases in the world, the incidence of osteoarthritis (OA) is increasing year by year. At present, the prevalence rate for adults aged ≥65 years in the United States is 33.6%. 15 Risk factors for OA include advanced age, female sex, obesity, genetic factors, race, and heavy physical work or activity. 15 Its pathogenesis is complex, involving mechanical overload, an increase of inflammatory mediators, metabolic changes, cell senescence, and so on. 24 Among these, with the aggravation of knee joint degeneration, the meniscus, cartilage, anterior and posterior cruciate ligament (PCL), and other tissues in the joint may be gradually destroyed.
Total knee arthroplasty (TKA) is a common surgical treatment for severe or end-stage knee OA. There are mainly 2 types of prostheses: posterior stabilized (PS) and cruciate retaining (CR). CR prostheses can reduce intercondylar osteotomy, restore posterior condylar eccentricity and joint line, and retain stress conduction function and the PCL, but surgery is more complicated and includes the risk of injuring the PCL. We believe that surgery for PS prostheses is easier than for CR prostheses because of the better exposure of the operative field, but the amount of osteotomy is larger and the PCL is removed. For patients who need TKA, there are still no exact criteria for choosing the type of prosthesis. Although Verra et al, 23 Jiang et al, 13 and Mayne et al 17 proposed that there was no significant difference in functional score and range of motion between the types of prosthesis, these studies did not examine the changes in proprioception after surgery. We believe that proprioception should be included when discussing the clinical efficacy of CR and PS prostheses, because one of the important differences between them is that CR prostheses retain the PCL. In addition to limiting the backward movement of the tibia relative to the femur during knee flexion and extension, preventing knee joint hyperextension, and providing rotational stability, a normal PCL plays an important role in enhancing the proprioception of the knee joint. 6
Proprioception is the ability to perceive the position of joints, which can be summarized as position perception and motion perception. The structural basis of proprioception in histology is the mechanoreceptor,7,9 and the number of mechanoreceptors determines the sensitivity of proprioception. 1 The normal PCL has abundant mechanoreceptors.1,5 But it is unclear if the PCLs of patients with OA who need TKA surgery contain enough mechanoreceptors, because the ligament may have undergone histological changes with increased age and degree of OA.14,16,20
The purpose of this study was to evaluate the relationship between the number of mechanoreceptors in the PCL and either patient age or degree of OA to evaluate the value of retaining the PCL during TKA. We hypothesized that the number of PCL mechanoreceptors will be low in older patients and those with severe OA.
Methods
Patient Information
The study protocol received institutional review board approval. Inclusion criteria were age 60 to 85 years and TKA with PS prosthesis for knee OA from August 2021 to February 2022. Exclusion criteria were other forms of arthritis (eg, rheumatoid, suppurative, traumatic), previous knee surgery or trauma, loss of the PCL, and other diseases that affected the PCL and its mechanoreceptors. Knee OA was determined according to the diagnostic criteria established by the American College of Rheumatology:
Knee pain most of the time in the previous month
Osteophytes on radiograph
Age ≥40 years
Knee joint fluid test showing OA
Cracking or grinding noise with joint movement
Morning stiffness for ≤30 minutes
OA is indicated if patients have symptoms 1 and 2; 1, 3, 5, and 6; or 1, 4, 5, and 6 at the same time.
This study enrolled 26 patients who fit the study criteria. Of these, 24 had undergone unilateral TKA and 2, bilateral TKA. Because the conditions of OA may be different in the knees of patients who underwent bilateral TKA, each knee was treated as a separate case. Therefore, 28 knees in 26 patients were evaluated in this study.
Study Groups
Patient Age
Patients were grouped according to age: group A (60-69 years; n = 8), group B (70-79 years; n = 12), or group C (≥80 years; n = 8).
OA Severity
Before TKA, each patient completed the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC) score, which evaluates knee OA severity with 24 items regarding pain, stiffness, and joint function. The score of each item ranges from 0 to 10. A WOMAC score ≤80 is considered mild OA; 81 to 120, moderate; and >120, severe OA. Patients were grouped according to WOMAC score as belonging to group I (≤80; n = 8), group II (81-120; n = 10), or group III (>120; n = 10).
Sampling and Fixing the PCL
The entire PCL sampling process was performed by the same surgeon (S.C.). After anesthesia, the patient was set in the supine position, and a pneumatic tourniquet was applied on the thigh. An anterior median incision was made on the diseased knee; the joint capsule was cut open in the medial parapatellar approach and valgus patella; and the anterior cruciate ligament and the medial and lateral meniscus were resected. Osteotomy was performed on the femoral condyle and tibial plateau, fully exposing the PCL and its end (Figure 1A), and the ends of the PCL that attached to the tibia and femur were sharply separated (Figure 1B). A knot was tied at the end of the PCL that attached to the tibia to facilitate the distinction between the ends, and the PCL was immediately soaked in 4% paraformaldehyde solution for 48 hours.
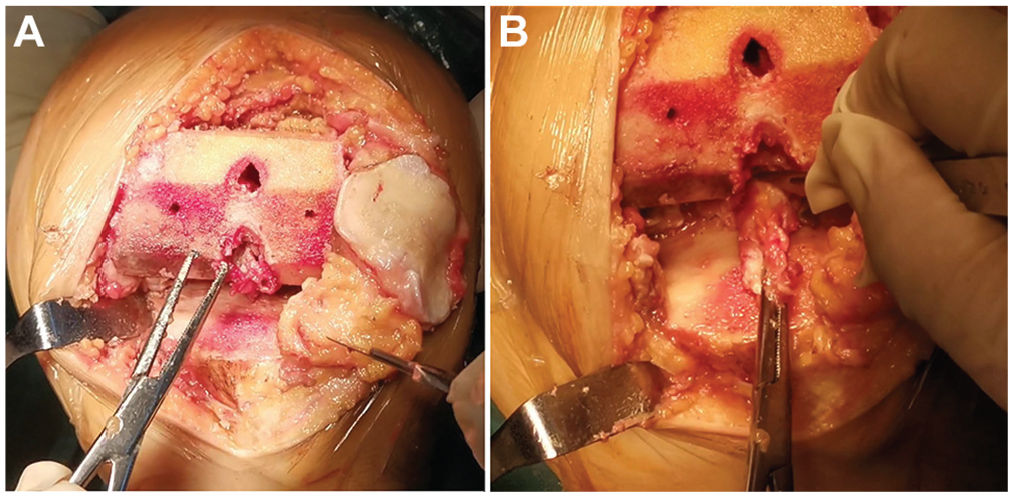
(A) The femoral intercondylar fossa and the posterior cruciate ligament were exposed after osteotomy. (B) Sharp separation of the posterior cruciate ligament.
Specimen Dehydration, Transparency, Wax Dipping, and Slicing
The fixed specimens were washed with running water for 24 hours and dehydrated for 2 hours with 80%, 90%, 95%, and 100% ethanol. The specimens were made transparent in the solvent of ethanol and xylene. The specimens were dipped into wax and embedded along the long axis until solidifying. Then we used a machine to make slices along the long axis of the PCL. To standardize the cross section of each case, we used the same sectional method for each PCL: 2 slices 4 μm thick that were 3 mm away from the farthest end, near the tibial attachment, were continuously cut perpendicularly to the long axis of each PCL; after which, they underwent histological staining with hematoxylin and eosin (HE) and immunohistochemical staining with S-100 protein. A total of 56 slices were obtained from the 28 cases.
HE and Immunohistochemical Staining
HE Staining
The steps for HE staining were as follows:
Drying the paraffin slices; adding xylene (10 minutes), 100% alcohol (1 minute), 100% alcohol (1 minute), 95% alcohol (1 minute), 80% alcohol (1 minute), 70% alcohol (1 minute), and 60% alcohol (1 minute); washing (1 minute).
Hematoxylin staining (15 minutes), then rinsing with running water (1 minute).
1% hydrochloric acid alcohol differentiation (controlled by naked eye or microscope), rinsing with running water (1 minute), saturated lithium carbonate solution (15 seconds), and rinsing with running water (2 minutes).
1% eosin alcohol solution (3 minutes), 70% alcohol (1 minute), 80% alcohol (1 minute), 90% alcohol (1 minute), 95% alcohol (1 minute), and 100% alcohol (1 minute).
Air-drying, optical resin sealing.
S-100 Protein Staining
The steps for S-100 protein staining were as follows:
Unfolding the slices in a water bath at 40°C; dewaxing in xylene I and II solution after drying; rehydrating step by step with anhydrous ethanol, 90% ethanol, and 70% ethanol for 2 minutes; and placing in distilled water for 2 minutes.
Boiling and repairing slices at high pressure, incubating at room temperature with 50 μL of peroxidase solution (10 minutes), and rinsing with phosphate-buffered saline (PBS; pH = 7.4; 3 × 5 minutes).
Incubating slices at room temperature with 50 μL of nonimmune animal serum (10 minutes), allowing excess liquid to be absorbed.
Incubating slices at room temperature with 50 μL of the first antibody, S-100 (1:1000; 60 minutes), and rinsing with PBS (3 × 5 minutes).
Incubating slices at room temperature with 50 μL of biotin-labeled second antibody (10 minutes) and rinsing with PBS (3 × 5 minutes).
Adding 50 μL of streptavidin-peroxidase into slices and incubating them at room temperature (10 minutes) and rinsing with PBS (3 × 5 minutes).
Adding 100 μL of freshly prepared 3,3′-diaminobenzidine solution and observing slices under microscope for 3 to 10 minutes.
Rinsing with tap water, redyeing with hematoxylin, and sealing with neutral gum.
Mechanoreceptor Evaluation and Count
All slices were scanned into pictures by a digital pathological section scanner (KF-PRO-005; Konfoong Biotech International) and read with K-Viewer software. The mechanoreceptors in each slice were classified into 4 types according to the method formulated by Freeman and Wyke 10 : Ruffini endings (REs), Pacinian corpuscles (PCs), Golgi tendon organ–like endings (GTOEs), and free nerve endings (FNEs). All slices were classified and counted by the same person (J.C.), who was blinded to patient identity. Çabuk et al 5 and Rajgopal et al 21 used S-100 staining to successfully classify the mechanoreceptors, so our counting observation was mainly based on the sections stained by S-100 protein, taking into account the multilayer structure of PCs. But it was difficult to clear and identify the multilayer membranes of PCs by S-100 staining. Therefore, when the morphology and size of the bodies stained by S-100 protein were found to be consistent with the structure of PCs described by Freeman and Wyke 10 , the adjacent section stained with HE was taken to look for the same body to confirm whether there was a multimembrane structure with the help of K-Viewer software; if there was no multimembrane structure, it would be classified as REs. Then counting and recording the number of mechanoreceptors were conducted for the whole slice.
Statistical Analysis
In SPSS 25.0 software (IBM), multifactor analysis of variance was used to evaluate the relationship among patient age, WOMAC score, and the number of mechanoreceptors in the PCL. P < .05 was regarded as statistically significant.
Results
Histomorphological Observation of Mechanoreceptors in the Posterior Cruciate Ligament
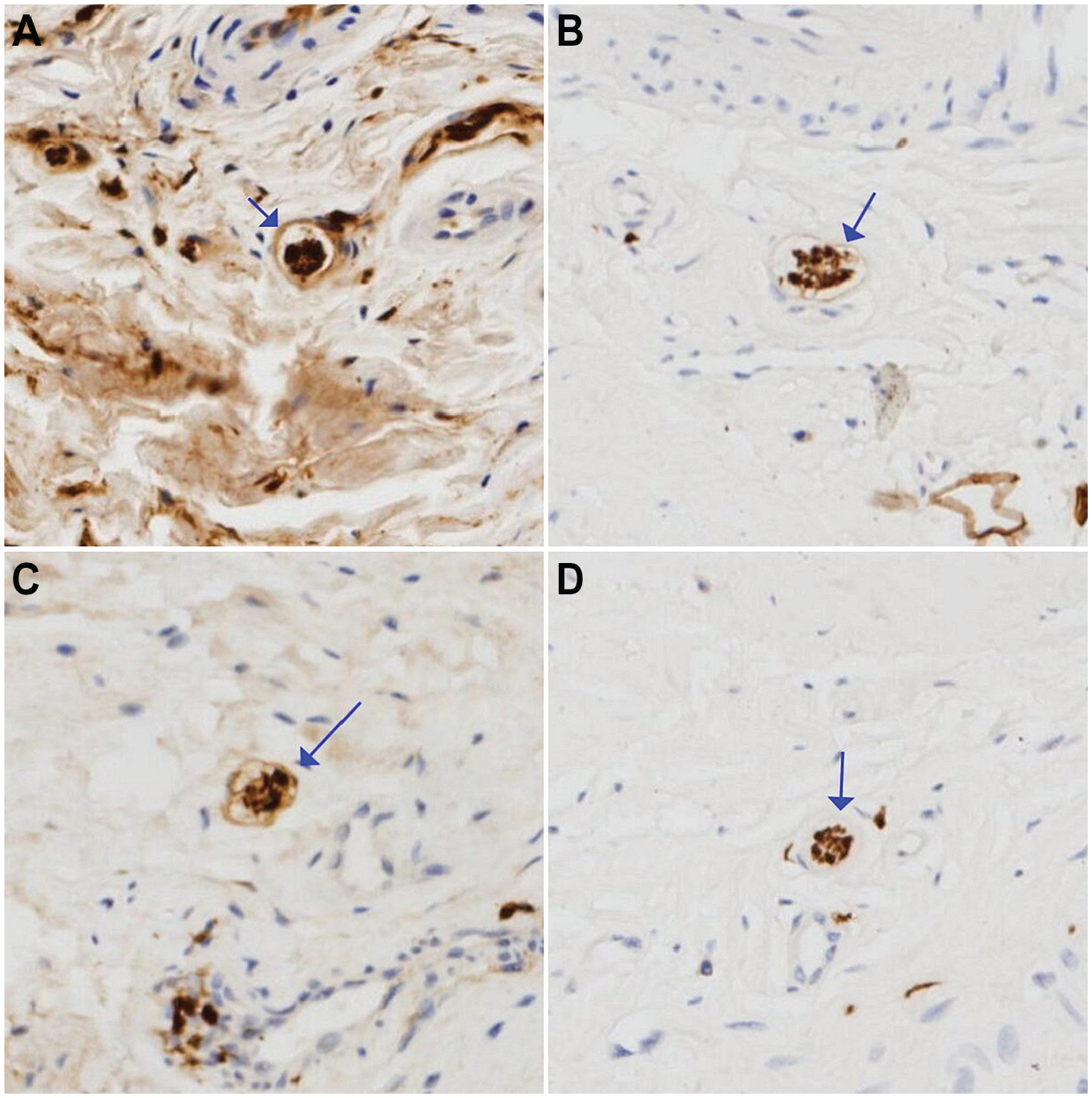
In the section images scanned by K-Viewer software, we observed all 4 types of mechanoreceptors. The PCs were round or oval (Figure 2). We could identify their multiple layers of membranes in only the HE-stained sections (Figure 2, C and D). The REs were oval or round, but they had just a thin membrane that surrounded thick nerve fibers in all sections (Figure 3). FNEs were loosely arranged without cell membranes and could be observed in only S-100 stained sections (Figure 4). GTOEs were fusiform and had just a layer of membrane, and their volume was the largest among the 4 mechanoreceptor types (Figure 5). Figure 6 shows examples of the fibers whose size or shape did not fit the mechanoreceptor classifications per Freeman and Wyke, 10 and these were not included in later analyses.

Examples of Pacinian corpuscles (PCs; arrows). S-100 protein staining: (A) a degenerated PC and sparse stained nerve tissue; (B) a PC with better morphology. Hematoxylin and eosin staining: (C) the same PC in panel A, with multiple layers of atrophied membranes; (D) the same PC in panel B, with multiple layers of membranes and a clearer and denser structure. All slides are shown at 1000 × magnification.

Examples of Ruffini endings (REs; arrows). (A, B) S-100 protein staining shows oval REs with a monolayer membrane. (C) Hematoxylin and eosin staining of the same RE in panel B at the adjacent section. All slides are shown at 500 × magnification.

Examples of free nerve endings (arrows) with S-100 protein staining. They are loosely arranged without any membranes. Slides are shown at 500 × magnification.

Examples of Golgi tendon organ–like endings (GTOEs) with a monolayer membrane (arrows). S-100 protein staining: (A and B) curled and deformed GTOEs and (C) a more regular GTOE. Hematoxylin and eosin staining: (D) the same GTOE in panel C, which is fusiform. All slides are shown at 250 × magnification except for panel B at 500 × magnification.
S-100 protein staining: examples of unclassified nerve fiber tissue (arrows). (A-C) Tissues have a layer of membrane. (C) The tissue has a slightly irregular membrane and (D) the tissue has no membrane. All slides are shown at 500 × magnification.
Quantitative Analysis of Mechanoreceptors in the PCL of Patients With Knee OA
A total of 56 slices were made, and 28 underwent HE and S-100 staining. The total number of mechanoreceptors in the 28 PCLs that underwent staining were classified by type and counted (Table 1). In addition, there were 481 unclassified nerve fibers whose size or shape was not consistent with the recognized characteristics of the 4 types of mechanoreceptors; they were not included in the subsequent analyses.
Number of Mechanoreceptors at the Tibial Attachment of the Posterior Cruciate Ligament by Type a
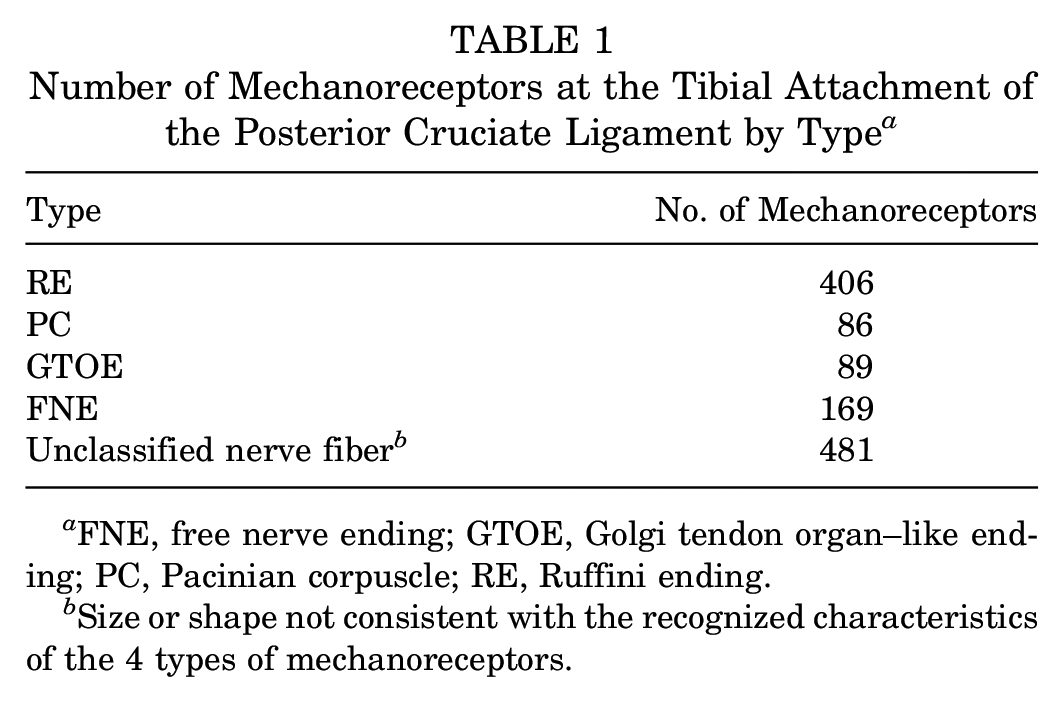
FNE, free nerve ending; GTOE, Golgi tendon organ–like ending; PC, Pacinian corpuscle; RE, Ruffini ending.
Size or shape not consistent with the recognized characteristics of the 4 types of mechanoreceptors.
The mean ± SD number of mechanoreceptors in the tibial attachment of the PCL was 14.50 ± 7.24 for REs, 3.07 ± 2.52 for PCs, 3.18 ± 2.07 for GTOEs, and 6.04 ± 2.98 for FNEs (Table 2, Figure 7). Table 3 shows the results of the comparison regarding the 4 types of mechanoreceptors. There were significant differences between REs and the other 3 types of mechanoreceptors (P < .001 for all), and there were significant differences between PCs and FNEs (P < .001) or between GTOEs and FNEs (P < .001). There was no significant difference between PCs and GTOEs (P = .86). Thus, REs were the most prevalent, FNEs were the second most, and PCs and GTOEs were the least prevalent types of mechanoreceptors in the tibial attachment of PCLs in patients with knee OA.
Number of Mechanoreceptors at the Tibial Attachment of the Posterior Cruciate Ligament a

FNE, free nerve ending; GTOE, Golgi tendon organ–like ending; PC, Pacinian corpuscle; RE, Ruffini ending.
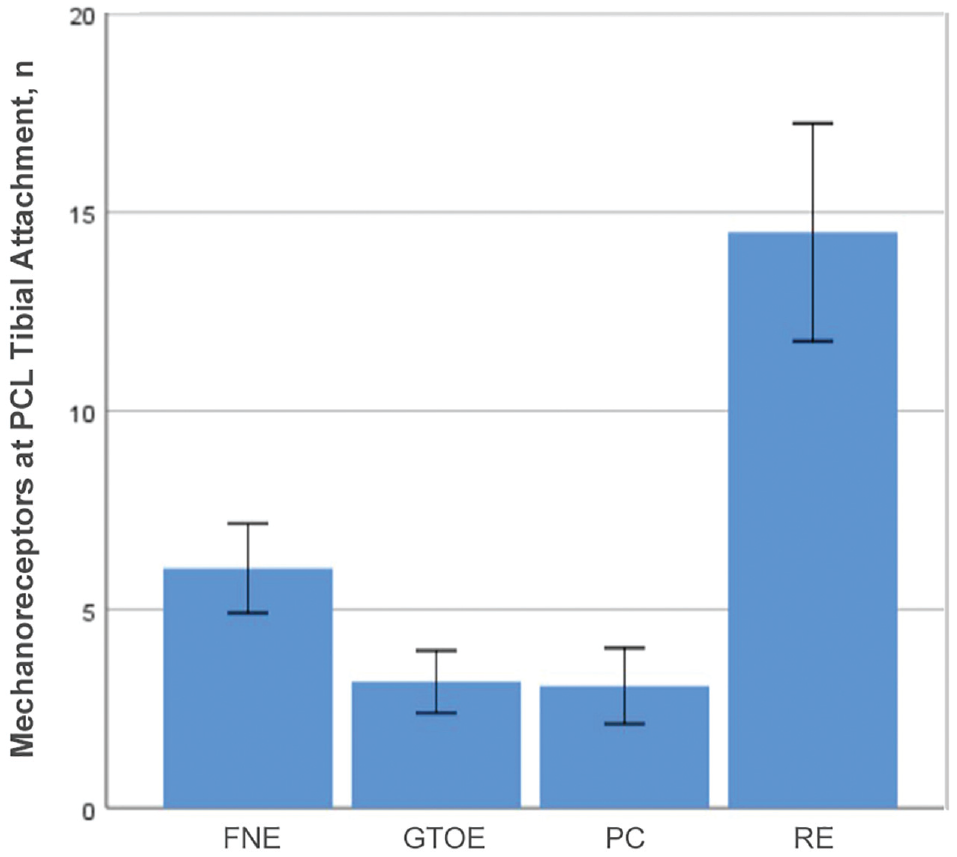
Mean number of mechanoreceptors at the tibial attachment of the posterior cruciate ligament (PCL). Error bars indicate 95% CI. FNE, free nerve ending; GTOE, Golgi tendon organ–like ending; PC, Pacinian corpuscle; RE, Ruffini ending.
Cross-tabulation of P Values for the Comparison of Mechanoreceptor Types a

Bold P values indicate statistically significant difference in mechanoreceptor count between types (P < .05). FNE, free nerve ending; GTOE, Golgi tendon organ–like ending; PC, Pacinian corpuscle; RE, Ruffini ending.
Number of Mechanoreceptors by Patient Age and WOMAC Score
In our experiment, we performed statistical analysis on only the total number of mechanoreceptors. Through multifactorial analysis of variance on the number of mechanoreceptors, we found that the main effect of age was not significant (P = .77), that the main effect of WOMAC score was significant (P < .001), and that there was no significant interaction between WOMAC score and age (P = .30).
Then we evaluated the number of mechanoreceptors according to the different age and WOMAC score groups (Table 4, Figure 8): the mean number of mechanoreceptors in groups A, B, and C was 24.00 ± 15.19, 30.92 ± 11.41, and 23.38 ± 11.39 respectively, with no significant difference between groups after pairwise comparison (Table 5). The number of mechanoreceptors in groups I, II, and III was 43.50 ± 4.99, 25.00 ± 5.27, and 15.20 ± 5.61 with significant between-group differences after pairwise comparison (I vs II, P < .001; I vs III, P < .001; II vs III, P < .001) (Table 6).
Number of Mechanoreceptors According to Patient Age and WOMAC Score Groups a

WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.

Mean number of mechanoreceptors in the tibial attachment of the posterior cruciate ligament (PCL) by (A) age group and (B) WOMAC score group. Error bars indicate 95% CI. WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Cross-tabulation of P Values for the Comparison of Mechanoreceptors by Age Group a

No P values indicate a statistically significant difference in mechanoreceptor count between groups (all P > .05).
Cross-tabulation of P Values for the Comparison of Mechanoreceptors by WOMAC Score Group a

All P values indicate statistically significant differences in mechanoreceptor count between groups (P < .05). WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
Discussion
In the current study, we found that the age of patients with knee OA had no significant effect on the number of PCL mechanoreceptors. There were significant differences in the number of mechanoreceptors according to WOMAC score (group I, 43.50 ± 4.99; group II, 25.00 ± 5.27; group III, 15.20 ± 5.61; P < .001 for all pairwise comparisons), indicating that the number of PCL mechanoreceptors decreased with increased (worsening) WOMAC score. This was the case even after we stratified the scores by age group. Through multifactorial analysis of variance on the number of mechanoreceptors, we found that the main effect of age was not significant (P = .77), that the main effect of WOMAC score was significant (P < .001), and that there was no significant interaction between WOMAC score and age (P = .30).
At present, there are few studies on the relationship between age and the number of mechanoreceptors. Dang et al 8 believed that the number of PCL mechanoreceptors decreased with age. Considering the histological degeneration, Kleinbart et al 14 found that the proportion of significant degeneration of the PCL in patients >70 years old was higher than that in patients <70 years old, but Levy et al 16 thought that the histological degeneration of the PCL began early (<50 years old) and proceeded slowly with age. These conclusions are not consistent with our research conclusions, which may be due to the large error caused by the low sample size of this experiment. Either the age grouping is not detailed enough to accurately reflect the relationship between age and the number of mechanoreceptors, or the subjective judgment in the classification of mechanoreceptors leads to the inaccurate number; furthermore, it may be that age is not an important factor affecting the number of mechanoreceptors, which would need more data to support.
With the aggravation of OA, the PCL gradually degenerates owing to the invasion of inflammatory factors and physical wear over a long time. Çabuk et al 5 found that the nerve tissue of the PCL in patients with OA was less than that in healthy patients, but the authors did not analyze the effect of different degrees of OA on the number of mechanoreceptors. Kleinbart et al 14 confirmed that OA can aggravate histological degeneration of the PCL. Levy et al 16 reported that histological degeneration of the PCL aggravated steadily per Outerbridge cartilage injury classification (grades 0-4), increasing from grade 0 to 3. Cartilage injury can be considered one of the manifestations of OA; as such, it is understandable that the histological degeneration of the PCL is aggravated with the progression of OA. Martins et al 19 stated that with the aggravation of histological degeneration, the neurovascular structure of the PCL was damaged more. These views support our research results.
In addition to the severity of OA, other factors may affect PCL degeneration. For example, Mullaji et al 18 believed that varus deformity of the knee (>15°) would increase the possibility of moderate degeneration of the PCL. Levy et al 16 believed that injury of the anterior cruciate ligament would lead to degeneration of the PCL. These factors are related to the degenerative changes of the PCL, but whether they lead to changes in the number of mechanoreceptors is unknown and needs further study.
Our study is a basic science experiment about PCLs and mechanoreceptors. The PCL is one of the most important ligaments of the knee joint; it mainly plays a role in preventing the tibia from moving backward relative to the femur and providing knee joint dynamic stability through proprioception and muscle activity. 2 Proprioception includes perception of the static position, displacement, velocity, acceleration, and muscle force of body parts. 3 Proprioception depends on mechanoreceptors, which are distributed in many tissues of the knee joint. Çabuk et al 5 found that there are mechanoreceptors at the PCL, the anterior articular capsule, and the medial meniscus, which attaches to the articular capsule. Çabuk et al 4 also reported that most mechanoreceptors were in tissue near the attachment point of the bone rather than in the center of the tendons and ligaments. Taking this into account, we needed to ensure that the cross sections of all slices were standardized to facilitate horizontal comparison. Our slicing methods were as follows: all slices 4 μm thick that were 3 mm away from the farthest end near the tibia were continuously cut perpendicularly to the long axis of each PCL.
The classification of mechanoreceptors into 4 types was derived from Freeman and Wyke. 10 Gao et al 11 summarized the morphology and function of these 4 types of mechanoreceptors. REs are round or oval bodies with a thin capsule, about 50 to 500 μm in size. Their main function is to feel the pressure in the joint cavity, the joint position, and the speed and angle of joint movement. PCs are round or oval bodies coated with polymembranes (15-30 layers), with a size about 150 to 600 μm, and their main function is to sense the initiation and acceleration of motion. GTOEs are fusiform with a thin capsule; their size is about 100 to 600 μm; and they usually give feedback on the limit position of the joint. FNEs have no myelin sheath and are about 0.5 to 1.5 μm in size. They can sense inflammation, pain, and intense mechanical stimulation. In our study, the classification of mechanoreceptors also referred to the morphological description by Gao et al.
Previous studies on mechanoreceptors mainly rely on gold chloride staining. Franchi et al 9 used gold chloride staining to observe all types of mechanoreceptors and found that patients with osteoarthrosis had fewer mechanoreceptors in PCL than healthy people. Now more immunological staining is used to label targets with the method of specific antigen-antibody responses. Rajgopal et al 21 used S-100 protein and mouse anti-neurofilament protein to label mechanoreceptors and successfully found neurons in the PCL from most patients with OA. Çabuk et al 5 used S-100 protein immunohistochemical staining to observe all types of mechanoreceptors. In addition, histological staining is one of the methods to observe mechanoreceptors. Dang et al 8 used a combination of histological and immunological methods to observe all types of mechanical receptors. Chun et al 7 also used immunohistochemical staining to determine the existence of mechanoreceptors.
In the current study, we used the combination of immunology and histology (ie, S-100 staining and HE staining). We observed all types of mechanoreceptors in S-100 immunohistochemical staining slices. HE staining was used only to determine whether the PCs had multilayer membranes, because such a structure is not nerve tissue and would not be labeled by S-100 protein. So we stained the adjacent slices with HE, identified the same body in the same position of adjacent slices, and observed whether the body had a multilayer membrane structure. Finally, we determined that all types of mechanoreceptors existed in our slices. In addition, we identified a new nerve ending whose size or shape was not described in the mechanoreceptor classification by Freeman and Wyke. 10 We therefore did not include it in our statistical data. We could not find any literature that has described this unclassified nerve ending in the PCL. We speculate that these nerve endings may be the cross section of afferent nerves that connect with the mechanoreceptors.
The conditional basis for supporting TKA with CR prosthesis is that there are abundant mechanoreceptors in the PCL, which can enhance the proprioception of the knee joint. Martins et al 19 and Rajgopal et al 21 found that mechanoreceptors or nerve tissue could be detected on most PCLs from patients undergoing TKA. Zhang and Mihalko 25 compared the number of mechanoreceptors of the PCL obtained during TKA with that in patients who had undergone CR prosthesis replacement 5 to 12 years before. They did not find a significant difference between them. This finding suggests that the PCL retained during TKA may still provide proprioception during postoperative activity. All of this shows that it is valuable to retain PCL. However, Çabuk et al 5 considered that the histological degeneration of the PCL in patients with OA was more serious and that the number of mechanoreceptors was less than that in healthy people, so the value of preserving PCL may not be as great as expected. Yet, they did not analyze in detail the number of mechanoreceptors of the PCL in patients with different degrees of OA, and they did not know whether the value of retaining PCLs in patients with OA at all levels was the same. The clinical results of Vandekerckhove et al, 22 Götz et al, 12 and Bravi et al 3 show that preservation of PCLs cannot significantly improve the proprioception or postural stability of the joint after TKA. Nevertheless, their study did not indicate the degree of OA in the experimental group and the control group, which does not reflect the true preservation value of the PCL. According to the results of our study, if the severity of OA is very high, the value of retaining the PCL during TKA is low.
Limitations
A limitation of this study is the small sample size, which may lead to large errors. To reduce selection bias and researcher bias, patient information was blinded during mechanoreceptor evaluation and counting, and we used the same person to complete the same process during each step (ie, sampling, making slices, staining, counting, observing, and statistics analysis). The WOMAC is a comprehensive index to reflect knee OA, but there may be some factors that it ignores, resulting in more bias. In addition, the subjectivity of WOMAC scoring and mechanoreceptor classification may have introduced more errors. Thus, more data are needed to support our conclusion.
In our experiment, we discussed only the changes in number of mechanoreceptors; we did not analyze what influence these changes would have on the actual proprioception. Yet, the lack of knee proprioception suggests a low value of retaining PCLs. It means that we do not know the exact low number of mechanoreceptors indicating that the PCLs have no value to retain. We plan to study the quantitative relationship between proprioception and mechanoreceptors in PCLs in the future and hope to find the key that can solve these problems.
Conclusion
The age of patients with knee OA has no significant effect on the mechanoreceptors, but the number of mechanoreceptors in PCLs decreased significantly with OA severity as indicated by the WOMAC score. These findings suggest that in patients of any age with high WOMAC scores, there may be little value as it relates to knee proprioception in performing a PCL-retaining TKA.
Footnotes
Acknowledgements
Len Zhi, PhD, and Zhu Yunjia, MS, are gratefully acknowledged for their support in specimen acquisition and histological method validation.
Final revision submitted December 11, 2022; accepted January 24, 2023.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto. Ethical approval for this study was obtained from The Second Affiliated Hospital of Chongqing Medical University (No. 2022-079).