
Abstract
Objectives
The mechanism underlying neuropathic pain (NP) in osteoarthritis (OA) of the knee is not completely understood. This study aimed to investigate whether possible NP in patients with knee OA undergoing knee surgery is associated with specific radiological findings.
Methods
This study included 197 patients who underwent knee surgery for symptomatic knee OA. Clinical evaluation was performed using the Central Sensitization Inventory (CSI), Western Ontario and McMaster Universities Arthritis Index (WOMAC), and PainDETECT questionnaire. Radiological evaluation was performed using the hip-knee-ankle (HKA) angle, posterior tibial slope (PTS), varus and valgus laxities, and magnetic resonance imaging OA Knee Score (MOAKS). Radiological findings were compared between patients with possible and unlikely NP. Logistic regression analysis was performed to identify the predictive factors for NP.
Results
There were 163 and 34 patients with unlikely NP and with possible NP, respectively. The percentage of patients with CSI score ≥ 40 was significantly higher in the possible NP group than in the unlikely NP group (17.6% vs. 6.1%). Patients with possible NP had worse WOMAC scores than patients with unlikely NP. There were no significant positive associations between the possible NP and radiological findings in knee OA. Regression analysis showed no predictive factors for possible NP.
Conclusions
Possible NP is not associated with specific radiological findings in knee OA. Patients with possible NP may mediate CS and experience more severe symptoms, including decreased knee function and lower quality of life, than patients with unlikely NP.
Keywords
Introduction
Osteoarthritis (OA) of the knee is a joint disease characterized by articular cartilage degeneration, meniscus tear/degeneration, synovitis, osteophyte formation, and subchondral bone change.1,2 Patients with knee OA experience interference with daily activities due to knee pain, joint instability, and restricted range of knee motion. The primary therapeutic target is pain as a cardinal symptom, and some studies have revealed an association between knee pain and subchondral bone marrow legion.3–5 However, the underlying pain mechanism in knee OA is not fully understood. 6
Knee OA pain has both nociceptive and neuropathic components.7–11 In addition, chronic noxious knee pain triggers central sensitization (CS) in 20%–40% of patients with advanced knee OA, which induces persistent pain even after noxious stimuli have been eliminated.12–14 In the knee joint, innervation has been confirmed in the synovium, periosteum, menisci, cruciate ligament, collateral ligament, joint capsule, and subchondral bone,15–19 and these regions can cause neuropathic pain (NP) and nociceptive pain. Treatment differs based on the diagnosis of nociceptive and NP. Because nociceptive pain mainly comes from tissue injury, anti-inflammatory drugs and surgical treatments are performed while NP is treated with antineuralgics such as duloxetine. 20 Diagnosis of NP is based on subjective evaluation such as the PainDETECT and Standardized Evaluation of Pain,21,22 but it is unclear how tissue injury is related to the onset of NP. If NP can be diagnosed based on objective evaluations such as magnetic resonance imaging (MRI) finding, it will be possible to make a more appropriate and earlier diagnosis and to select an appropriate treatment method.
For the measurement of NP in knee OA, the PainDETECT, including the modified one, questionnaire has been validated and suggested that 20%–67% of patients with knee OA have possible NP.7–11,21 To comprehensively assess knee tissue (articular cartilage, ligaments, bone, menisci, and fat tissue) in knee OA, the magnetic resonance imaging osteoarthritis knee score (MOAKS) has been validated and useful.23–27 This study aimed to investigate whether possible NP in patients with knee OA undergoing knee surgeries is specific radiological findings of the knee joint using MOAKS. Identification of specific radiological findings resulting in NP has the potential to improve pain management, including pharmaceutical, physical, and surgical treatment, to provide pain relief and improve quality of life in patients with knee OA. In the current study, we hypothesized that specific radiological findings are positively associated with possible NP in patients with knee OA undergoing knee surgery.
Materials and methods
Participants
Consecutive 229 patients undergoing knee surgeries for symptomatic knee OA between April 2020 and September 2021 at our institution were included in this cross-sectional study. Performed surgeries included osteotomies around the knee or total or unicompartmental knee arthroplasty. The inclusion criteria were the diagnosis of knee OA by an anteroposterior radiographic examination, an age of 40 years or more, and persistent knee pain after at least 3 months of conservative treatment. The exclusion criteria were a history of knee surgeries, infection, rheumatoid arthritis, valgus alignment of the knee, and lumbar spinal disorders with neurological symptoms. After selection based on the inclusion and exclusion criteria, one patient with a diagnosis of knee joint infection, 27 with valgus knees, and four experiencing lumbar spinal disorder were excluded. Finally, 197 patients were included in this study. Patients completed questionnaires regarding pain and symptoms and underwent computed radiography (CR) and MRI examinations.
Clinical evaluation
Patient demographic data, including age, sex, body mass index, and maximum extension and flexion angles, were recorded. Symptoms were evaluated using questionnaires that were completed by the patients. The incidence of CS was screened using the Central Sensitization Inventory (CSI), with a score of ≥ 40 indicating CS.28,29 Osteoarthritis severity was evaluated using the Western Ontario and McMaster Universities Arthritis Index (WOMAC), a valid and reliable measure of knee pain, stiffness, and functional limitations, 30 with higher scores indicating more severe OA. Neuropathic pain was determined using the PainDETECT questionnaire, 21 with a slight modification according to the modified PainDETECT. 8 In brief, patients were instructed to report on their symptoms “in or around each knee” as opposed to “their main area” of pain in the original version. It is composed of seven items evaluating pain quality, one item evaluating pain pattern, and one item evaluating pain radiation. The total score is an aggregated score ranging from −1 to 38. The 12-point cutoff point was used to discriminate patients with unlikely NP (PainDETECT ≤ 12 points) from patients with possible NP (PainDETECT > 12 points).
Radiographic assessment
The Kellgren–Lawrence (K–L) grade, 31 hip-knee-ankle (HKA) angle, and posterior tibial slope (PTS) were measured using the Rosenberg view, double-leg standing anteroposterior view of the lower limb, and lateral view of the lower limb, respectively. Varus and valgus laxities were evaluated using the anterolateral stress view of the knee. Varus and valgus laxities were defined as differentials between joint line convergence angles under no stress and varus or valgus stress (15 lb) at 30° flexion, respectively.
Magnetic resonance imaging osteoarthritis knee score
Magnetic resonance imaging osteoarthritis knee score with a slight modification was used for semiquantitative evaluation of knee joint tissues, including cartilage degeneration, bone marrow lesions, bone cysts, osteophytes, Hoffa-synovitis, synovitis-effusion, menisci, anterior and posterior cruciate ligament, pes anserine bursitis, iliotibial band signal, infrapatellar bursa signal, and ganglion cysts. In scoring cartilage degeneration, bone marrow lesions, and bone cysts, the medial femoral condyle and medial tibial condyle were combined as the medial compartment, the lateral femoral condyle and lateral tibial condyle as the lateral compartment, and the medial and lateral facet of the patellofemoral (PF) joint as the PF joint. The reliability of the MOAKS system has been reported before, and agreement by the same readers has been shown to be good to excellent. 23
Reproducibility of measurements
The interclass correlation coefficient (ICC) of the radiographic measurement (HKA angle, PTS, varus and valgus laxities) and MRI scoring (MOAKS) were calculated using the Statistical Package for the Social Sciences. Two observers calculated the interclass reliability based on the results of the initial radiographic assessment in randomly selected 20 patients. A single observer calculated the intraclass reliability from the results from the initial assessment and from the assessment 4 weeks after the radiographic and MRI evaluations in randomly selected 20 patients. In all evaluations, the observers were blinded to the clinical status of the patients. An ICC score ≥ 0.75 was considered excellent, ≥ 0.60 to < 0.75 good, ≥ 0.40 to < 0.60 fair, and < 0.40 poor. 32
Statistical analyses
Descriptive statistics were calculated for all quantitative and qualitative variables. Patients with possible NP and unlikely NP were compared for differences in demographic, radiographic, MOAKS, and clinical factors using t-tests or Wilcoxon rank sum tests for continuous variables and chi-squared or Fischer’s exact test for categorical variables, as appropriate. Logistic regression analysis with stepwise selection was used to identify the predictive factors for possible NP (PainDETECT > 12 points). Independent factors included radiographic parameters (HKA angle, PTS, varus and valgus laxities) and MOAKS items (cartilage degeneration, bone marrow lesions, bone cysts, osteophyte, medial meniscus and lateral meniscus, ligament, Hoffa-synovitis, synovitis-effusion, pes anserine bursitis, iliotibial band signal, and infrapatellar bursa signal).
Ethical approval
This study was approved by the institutional review board of our institution (approval no. TGE01668-066).
Results
Patient characteristics
Patient characteristics (n = 197).

K–L grade, Kellgren–Lawrence grade.
Association between possible NP and health-related quality of life
Comparison of WOMAC score between the patients with unlikely and possible NPs (n = 197).

WOMAC, Western Ontario and McMaster Universities osteoarthritis index; NP, neuropathic pain.
Radiographic assessment
Comparison of radiographic parameters between the patients with unlikely and possible NPs (n = 197).
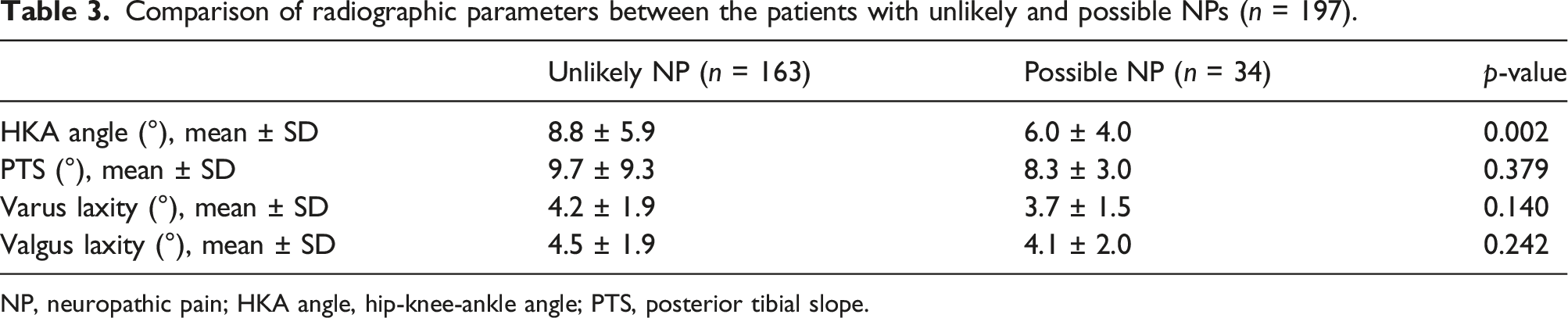
NP, neuropathic pain; HKA angle, hip-knee-ankle angle; PTS, posterior tibial slope.
Magnetic resonance imaging osteoarthritis knee score
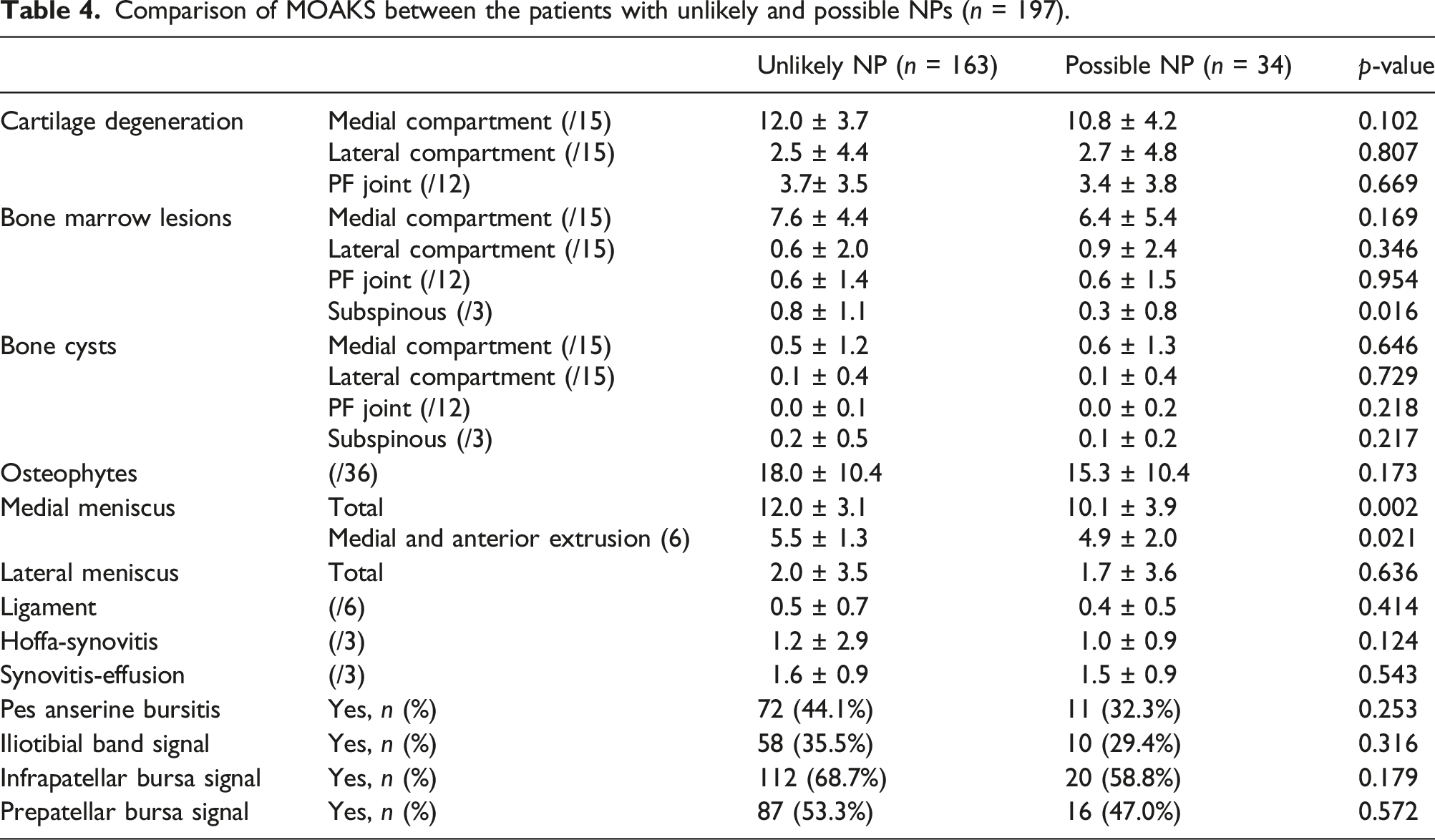
Comparison of MOAKS between the patients with unlikely and possible NPs (n = 197).
Logistic regression analysis for the risk factors for possible NP
Logistic regression analysis with stepwise selection was performed for the predictive factors for possible NP with independent factors, including radiographic parameters and MOAKS items. Regression analysis showed no predictive factors for possible NP.
Discussion
The most important finding in this study was that there were no significant positive associations between possible NP and radiological findings as shown by CR and MRI images in knee OA. Rather, patients with possible NP were significantly negatively associated with higher score of the medial meniscus and subspinous bone marrow lesions in MOAKS and also showed significantly higher CSI scores than patients with unlikely NP. These results suggest that possible NP in knee OA is not associated with the radiological findings in the knee or the progression of knee OA. Patients with possible NP may mediate CS and experience more severe OA symptoms, including decreased knee function and lower quality of life, than patients with unlikely NP.
Previous studies have shown that 20%–46% of patients with knee OA present possible NP,7–9,11 which is consistent with the results of the current study where possible NP was identified in 20.3% of all patients (34/163 patients). In the studied population of patients undergoing knee surgeries for knee OA, patients with possible NP have more severe osteoarthritic symptoms than patients with unlikely NP. The WOMAC total score of patients with possible NP was significantly higher than that of patients with unlikely NP (67.6 ± 19.5 vs 50.0 ± 19.7, p < 0.001), which was nearly the same as in previous reports.9,34 In addition, patients with possible NP have significantly higher average CSI scores and higher percentages of CSI ≥ 40 than patients with unlikely NP, suggesting that a subset of patients with knee OA with possible NP have centrally mediated pain sensitization, as previously reported.8,35
The mechanism underlying possible NP in knee OA is not completely understood, and cumulative data have shown that chronic pain in knee OA is caused by NP and CS. 36 Repetitive local stimuli, including mechanical stress and inflammation in knee OA, result in structural damage and innervation of the knee structures. This nociceptor stimulation may lead to modification of peripheral and/or central pain-transmitting neurons arising from damage to a nerve innervating knee joint structures, 13 which mediate NP and central pain sensitization. 37 For early diagnosis and early therapy for NP and central pain sensitization, identification of structural damage, which is the epicenter of NP, might be necessary. A cross-sectional observational pilot study using the PainDETECT questionnaire and MRI in 50 patients with knee OA showed that meniscal lesions is a risk factor for NP in patients with knee OA. 34 However, in the current study, there were no positive associations between NP and radiological findings; rather, meniscal scores in MOAKS were significantly higher in the unlikely NP group than in the possible NP group. This discrepancy may be attributed to differences in the study design, including patient selection and their background: patients with moderate to severe pain or undergoing surgery and K–L grades 2 to 3 or grades 3 to 4. Another possible explanation is that meniscal injury may occur and cause NP in the early stage of OA, but in the late stage of OA, other tissue injuries may cause NP and the meniscus may not be the main cause of NP anymore. Based on the results showing no relationship between specific knee tissues and NP, it is suggested that various tissues in the knee joint cause NP, and that the causative tissues of NP also change depending on the stage of OA. One of the problems related to NP in knee OA is that patients with knee OA with NP may undergo knee surgery due to pain, despite relatively lower joint structural damage that does not necessarily require surgery. This concern is supported by the inverse association between preoperative radiographic severity and postoperative pain in patients who underwent joint replacement surgery for knee OA 38 and the association between preoperative possible NP and development of persistent postoperative pain following total knee arthroplasty. 39 In the treatment of knee OA, to reduce patients taking the ineffective prolonged use of anti-inflammatory drugs or those with continuous NP after surgery, a screening of NP using the PainDETECT questionnaire or other NP scales should be performed, and personalized pain management considering radiological findings and pain severity needs to be established.
The current study has some limitations. First, this study included only patients with advanced knee OA who underwent surgery, and the prevalence of NP may differ in other patients with slight to mild knee OA. Second, the diagnosis of NP was based solely on the PainDETECT questionnaire. However, it provides a high level of confidence in previous studies, and no gold standard test for the diagnosis of NP in knee OA has been established.7,40,41
Conclusion
This study failed to prove the hypothesis that specific radiological findings of the knee are positively associated with possible NP in patients with knee OA undergoing knee surgery. Possible NP was not associated with knee joint alignment, laxity, or MRI finding of the knee joint.
Footnotes
Authors’ contribution
H. Ogawa: Study design, data collection and analysis, statistical analysis, and initial draft preparation.
Y. Nakamura, K. Sohmiya, M. Sengoku, T. Shimokawa, and K. Ohnishi: Initial draft preparation and data collection.
K. Matsumoto and H. Akiyama: Initial draft preparation.
All authors read and approved the final version of the paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee and with the 1964 Declaration of Helsinki and its later amendments or comparable ethical standards. This cross-sectional study was approved by the Institutional Review Board of Ogaki Tokushukai Group (approval number: TGE01668-066).