
Abstract
Background:
Rotator cuff tears are common in the elderly population and are associated with increased pain, decreased function, and decreased enjoyment of recreational activities.
Purpose:
To evaluate clinical outcomes at a minimum of 5 years after arthroscopic repair of full-thickness rotator cuff tears in recreational athletes aged ≥70 years at the time of surgery.
Study Design:
Case series; Level of evidence, 4.
Methods:
Included were recreational athletes aged ≥70 years who underwent arthroscopic rotator cuff repair (RCR) from December 2005 to January 2016. Patient and surgery characteristics were collected prospectively and retrospectively reviewed. Patient-reported outcome (PRO) scores utilized were the American Shoulder and Elbow Surgeons (ASES), Single Assessment Numeric Evaluation (SANE), the shortened version of Disabilities of the Arm, Shoulder and Hand score (QuickDASH), 12-Item Short Form Health survey (SF-12) questionnaire (Physical Component Summary and Mental Component Summary), and patient satisfaction. Kaplan Meier survivorship analysis was performed, with failure defined as revision RCR or retear on magnetic resonance imaging (MRI).
Results:
Overall, 71 shoulders (n = 67 patients [44 men, 23 women]; mean age, 73.4 years [range, 70.1-81.3 years]) were included in this study. Follow-up data was obtained for 65 of the 69 available shoulders (94%) at a mean of 7.8 years (range, 5-15.3 years). Mean age at follow-up was 81.2 years (range, 75.7-91.0). One RCR was revised after a traumatic accident, and another had a symptomatic, MRI-confirmed retear. One patient had lysis of adhesions for stiffness 3 months postoperatively. All PRO scores improved from pre- to postoperatively—ASES, from 55.3 to 93.6; SANE, from 62 to 89.6; QuickDASH, from 32.9 to 7.3; and SF-12 Physical Component Summary, from 43.3 to 53 (P < .001 for all)—and the median satisfaction score was 10 out of 10. Postoperatively, 63% of the patients returned to their original fitness program and 33% of patients modified their recreational activity. Survivorship analysis showed a 98% survival rate at 5 years and a 92% rate at 10 years.
Conclusion:
Sustained improvement in function, reduced pain, and return to activities was seen after arthroscopic RCR in active patients ≥70 years old. Despite one-third of patients modifying their recreational activity, the cohort reported high levels of satisfaction and general health.
Rotator cuff tears are among the most frequently encountered shoulder pathologies and result in pain, loss of function, and decreased ability to participate in recreational activities. As patients age, rotator cuff pathology is observed at increasing rates,26,34,35 with 1 study 38 reporting full-thickness rotator cuff tears in 45.8% of patients >70 years compared with 12.8% of patients in their 50s. In addition to being more likely to have a rotator cuff tear, patients >60 years old are 2 times more likely to develop large tears and 3 times more likely to develop massive tears compared with those <60 years old. 14 Given the aging demographics in modern society in combination with an increasing number of elderly patients expressing the desire to remain physically active during recent decades, this creates a challenging clinical scenario.
While arthroscopic rotator cuff repair (RCR) has been shown to improve function and decrease pain and have excellent rates of return to activity,3,12,13,17,19,24 older people often have various comorbidities and risk factors that make treatment of shoulder conditions difficult. Patient factors—such as increased age, osteoporosis, decreased tendon vascularity, larger size tears, tendon retraction, and fatty infiltration—as well as medical comorbidities—such as diabetes and hyperlipidemia— influence RCR outcomes and increase retear rates.6-8,18,21,27,32,39 Despite these factors, arthroscopic RCR in this patient population has produced encouraging clinical outcomes, 4 shown superiority over debridement alone, 10 and can be more cost-effective compared with reverse total shoulder arthroplasty. 9 These findings, in the setting of increasing functional demands of elderly patients, have led to more patients being considered for primary arthroscopic RCR.
Despite the aforementioned challenges with arthroscopic RCR in this patient population, many active patients maintain the expectation that surgical repair will allow for their return to their preinjury levels of function. While short-term outcomes have been favorable, 5 questions surrounding the longevity and durability of arthroscopic RCR in active, elderly patients remain. The purpose of this study was to evaluate clinical outcomes after arthroscopic repair of full-thickness rotator cuff tears in self-identifying recreational athletes aged ≥70 years at the time of surgery at a minimum of 5 years after surgery. We hypothesized that patients would experience improvements in clinical outcomes that extended beyond the minimum 5-year time point.
Methods
A retrospective review of prospectively collected data was performed in this institutional review board–approved study. All surgeries were performed by a single surgeon (P.J.M.) between December 2005 and January 2016. Patients aged ≥70 years who had their full-thickness supraspinatus (SSP) tears—with or without infraspinatus (ISP) or subscapularis (SSC) involvement—repaired arthroscopically and who self-identified as recreational athletes were included in the study. Recreational athletics was defined as physical activity in an individual or group setting intended as exercise and independent of normal daily activities. Patients who previously refused to participate or died before the final follow-up were excluded from the final analysis. Additional exclusion criteria were partial RCR, concomitant clavicular or scapular fractures, acromioclavicular joint injuries, concomitant ulnar nerve release procedures, or previous total shoulder arthroplasty. Patient characteristics, recreational activity, imaging, and surgical information were collected.
Surgical Technique
The arthroscopic RCR technique utilized was based on tear patterns using contemporaneous techniques. A knotted suture bridge double row (DR) technique was used earlier in the study period. Later, after biomechanical studies supported their use, a knotless tape bridge DR technique was used. 33 While the preferred technique of the senior surgeon (P.J.M.) is a bridging DR construct, select cases were performed with a standard single row (SR) repair technique if tears were small and easily reduced to their native location. Linked DR constructs with anchors and tapes were utilized to repair crescent-shaped tears directly to the bone. L- and U-shaped tears were repaired with a combination of margin convergence and footprint restoration with anchors. 23
Surgical repair techniques for rotator cuff tears have previously been published11,25 and are briefly reviewed here. Operations were performed in the beach-chair position with the patient under general anesthesia in addition to an interscalene nerve block. The operative extremity was placed in a pneumatic arm holder (Tenet T-Max Beach Chair and Spider arm positioner; Smith & Nephew) and was prepared and draped in standard fashion. First, a standard diagnostic arthroscopy was performed to confirm the suspected rotator cuff tear and identify any concomitant pathology. A subpectoral biceps tenodesis or tenotomy was performed if the biceps tendon demonstrated any degeneration, synovitis, instability, or pully lesions, or if there was disruption of the biceps anchor. The biceps tendon was tenotomized during the intra-articular portion of the procedure and the tenodesis was completed after RCR. Biceps tenodesis was performed according to Pogorzelski et al, 30 who previously described a technique using an interference screw (7 or 8 mm; Arthrex). Patients also underwent subacromial decompression and acromioplasty to create a Bigliani type 1 acromion before RCR.
In all cases, a bleeding bony bed was created with an arthroscopic shaver to enhance tendon healing to the rotator cuff footprint on the greater tuberosity. The integrity of the underlying cortex was preserved to ensure secure fixation. For the knotted suture bridge repairs, the medial anchors (4.5-mm Corkscrew anchor; Arthrex) were placed slightly lateral to the articular margin. The 2 sutures (No. 2 FiberWire; Arthrex) were then passed through the tendon adjacent to each other and just lateral to the musculotendinous junction using a suture shuttling device (SutureLasso, 90° straight; Arthrex). 37 The sutures were placed in a manner that facilitated the repair of the tendon to the anatomic footprint. A sliding Weston knot and 4 subsequent, alternating half-hitches were used to secure the medial row anchors. One suture strand of each medial row anchor was then grasped, tensioned, and inserted into the eyelet of the first lateral row anchor (4.75-mm biocomposite SwiveLock or 4.5-mm Pushlock; Arthrex). The lateral row anchor was then inserted into the anterolateral rim of the greater tuberosity. The same process was then repeated with the second lateral row anchor, creating the crossing, DR repair when the anchor was placed at the posterolateral rim of greater tuberosity. 22
The knotless, tape bridge repairs (Figure 1) were performed using similar principles. An RCR kit (SpeedBridge Kit with 4.75-mm biocomposite SwiveLock anchors), which contained 2 medial row anchors loaded with a No. 2 suture tape and 2 tapeless lateral row anchors, was used. Alterations to the above-described knotted procedure were that the medial row anchors did not require knot tying and that suture tapes were passed with 1 pass through the tendon. Again, 1 strand of, in this case, suture tape from each medial row anchor was inserted into the eyelet of the lateral row anchors, which were placed at the anterolateral and posterolateral rims of the greater tuberosity.
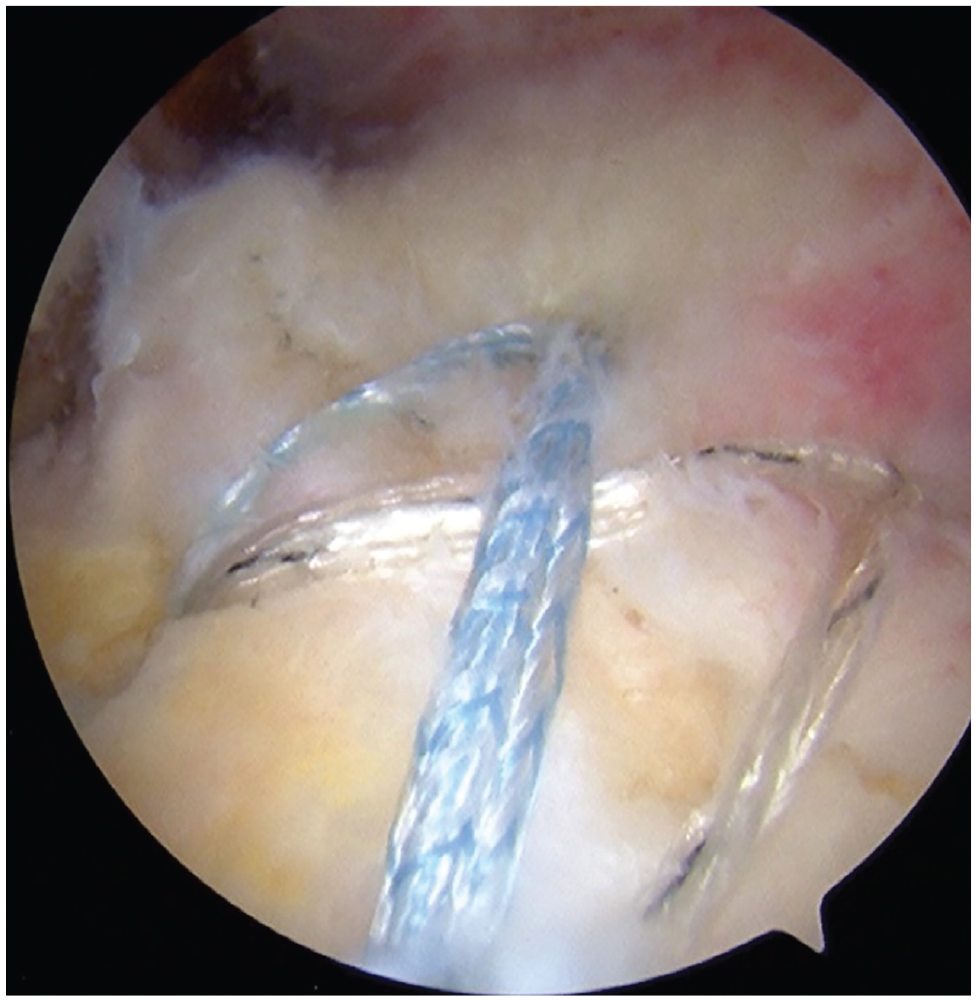
An arthroscopic view through a lateral portal illustrating a knotless 4-anchor, double-row rotator cuff repair of a 74-year-old avid skier.
Postoperative Rehabilitation
Postoperatively, patients were placed in a sling with an abduction pillow and were encouraged to start movement of the fingers, wrist, and elbow immediately. Passive range of motion (ROM) exercises were also started on the first day and continued for 6 weeks. Between 4 to 6 weeks after surgery, patients began active-assisted ROM. Once all active-assisted shoulder movements could be performed without pain, patients transitioned to unassisted active ROM exercises. This typically occurred 4 to 6 weeks postoperatively. At approximately 8 to 10 weeks after surgery, patients began strengthening exercises that targeted the rotator cuff muscles. Patients who underwent an additional biceps tenodesis were asked to avoid any resisted elbow flexion for 6 weeks. Patients were typically released to all activities of daily living at 14 to 16 weeks while undergoing continued strengthening. Full return to sports activities was permitted after the physical therapist’s clearance and typically achieved by 20 to 25 weeks postoperatively. 36
Patient-Reported Outcomes
Minimum 5-year follow-up data were obtained via electronic questionnaires and compared with preoperatively collected patient-reported outcome (PRO) scores. PROs collected were the American Shoulder and Elbow Surgeons (ASES) score, Single Assessment Numerical Evaluation (SANE) score, the shortened version of Disabilities of the Arm, Shoulder and Hand (QuickDASH) score, the 12-Item Short Form Health Survey (SF-12) questionnaire Physical Component Summary (PCS) and Mental Component Summary (MCS), and patient satisfaction (range, 1-10, where 10 = highly satisfied). Complications and further surgical interventions were assessed. If patients had not returned their annual questionnaires after 5 years, they were contacted regarding elective participation in the study. No questions regarding the PROs were asked via telephone. PROs available in the institutional database at time points of 1 and 2 years postoperatively were used to illustrate progression over time. Additional questions were asked regarding the level of pain associated with recreational activities, activities of daily living, and work. Patients were also asked questions regarding reasons for activity modification and the need for additional surgeries. Failure was defined as revision RCR or symptomatic rotator cuff retear with magnetic resonance imaging (MRI) confirmation. Patients with an ASES score of <75 with a corresponding satisfaction score of <7 were identified as having “poor” outcomes. The minimal clinically important difference (MCID) for the ASES score was an improvement of ≥15.2 points in this patient group. 20
Statistical Analysis
Statistical analysis was performed with SPSS Version 11.0 (IBM). A priori power analysis was not performed because of a fixed sample size. However, considering the study design, a minimum sample size of 57, 2-tailed testing, an alpha level of .05, and an effect size of d = 0.38 were detectable with a statistical power of 80%. Furthermore, assuming an SD of 10 points, 29 this effect size corresponds to a between–time point mean difference of 3.8 points on the ASES scale.
Categorical data were presented as numbers with percentages and continuous data as the mean ± SD, or mean with range for not normally distributed data. For normally distributed variables, an independent or paired t test was used. For nonparametric data, the Mann-Whitney or Kruskal-Wallis tests were performed. The Fisher exact test was used for discrete covariates. Survivorship analysis was performed using Kaplan-Meier survival curves with failure defined as progression to revision RCR, rotator cuff tear demonstrated on MRI, or progression to an arthroplasty procedure. The significance level was set at P < .05.
Results
Between December 2005 and January 2016, arthroscopic RCR was performed on 115 shoulders of patients ≥70 years old by the senior surgeon (P.J.M.). After applying the exclusion criteria, 71 shoulders (N = 67 patients) were included in the study group (Figure 2). The mean age of the study cohort at the time of RCR was 73.4 years (range, 70.1-81.3 years), and there were 44 men and 23 women. Also, 6 RCRs (8.5%) were performed as revision procedures. Additional patient characteristics are reported in Table 1. Rotator cuff tears involved only the SSP in 30 shoulders (42.3%), the SSP and ISP in 36 shoulders (50%), the SSP and SSC in 4 shoulders (5.6%), and the SSP, ISP, and SSC in 2 shoulders (2.8%). A total of 67 shoulders (94.4%) were repaired with a DR bridging technique, while 4 shoulders (5.6%) were repaired with an SR technique. Further surgical data are illustrated in Table 2. Two shoulders were removed from the final analysis. One shoulder surgery was defined as a failure because of a symptomatic, MRI-confirmed retear 1 year after surgery. Another patient experienced a glenoid fracture and labral tear after a high-speed traumatic cycling accident at 11.4 months postoperatively. Although he underwent a subsequent surgery, his operation was not considered a surgical failure, as his RCR was shown to be intact upon surgical intervention for his glenoid fracture. Minimum follow-up was obtained on 65 of 69 shoulders (94%) at a mean follow-up of 7.8 years (range, 5-15.3 years). Mean age at follow-up was 81.2 years (range, 75.7-91.0). Primary recreational activities are reported in Table 1.

Study flow diagram. AC, Acromioclavicular joint; MRI, magnetic resonance imaging; RCR, rotator cuff repair; TSA, total shoulder arthroplasty.
Preoperative Characteristics of the Study Cohort a

RCR, rotator cuff repair.
Other activities included hockey, masters pole vaulting, yoga, hiking, and horseback riding.
Surgery Characteristics a
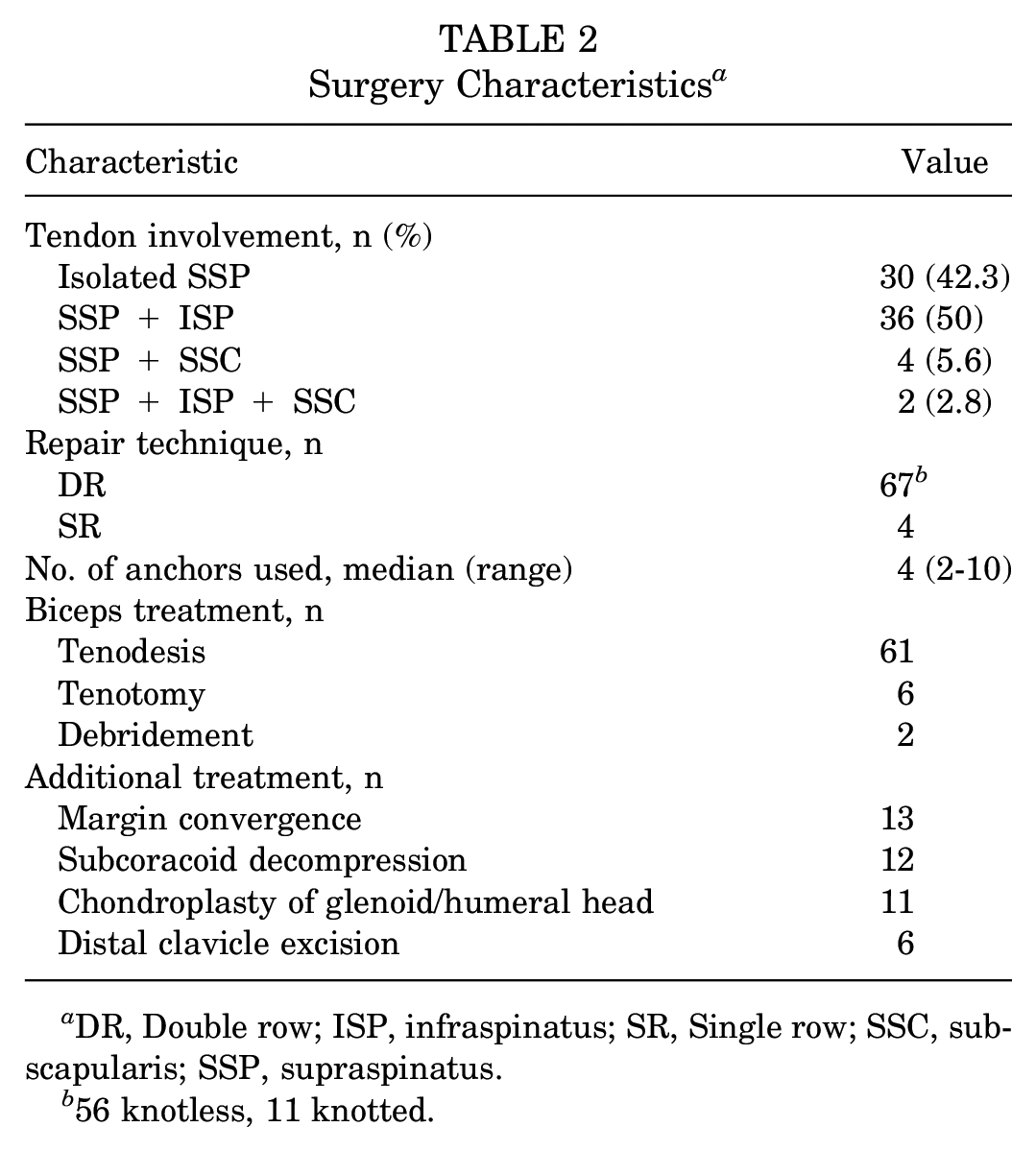
DR, Double row; ISP, infraspinatus; SR, Single row; SSC, subscapularis; SSP, supraspinatus.
56 knotless, 11 knotted.
Patient-Reported Outcomes
At a minimum 5-year follow-up, the ASES (from 55.3 to 93.6; P < .001), SANE (from 62 to 89.6; P < .001), QuickDASH (from 32.9 to 7.3; P < .001), and SF-12 PCS (from 43.3 to 53: P < .001) scores significantly improved pre- to postoperatively. Also, 93% of patients achieved the MCID for the ASES score, which was improved ≥15.2 points. 20 There was no significant change in the SF-12 MCS scores (P = .582). The median patient satisfaction with surgical outcomes was 10 (range, 2-10); however, 10 patients (16.1%) reported a satisfaction level of <7. PROs at the final follow-up were not associated with age at the time of surgery, prior RCR, critical shoulder angle, Goutallier grade, tendon involvement, or the number of anchors used. When evaluated at postoperative time points of 1 year, 2 years, and 5 years, shoulder-specific PROs illustrated significant improvements at 1-year follow-up, which was maintained at a minimum of 5 years (Figure 3A). There was no significant change in PROs between any of the follow-up time points. Mental health scores (SF-12 MCS) were unchanged between time points (Figure 3B). Physical health (SF-12 PCS) was shown to be significantly improved at 1-year follow-up and maintained through a minimum 5-year follow-up (Figure 3B).
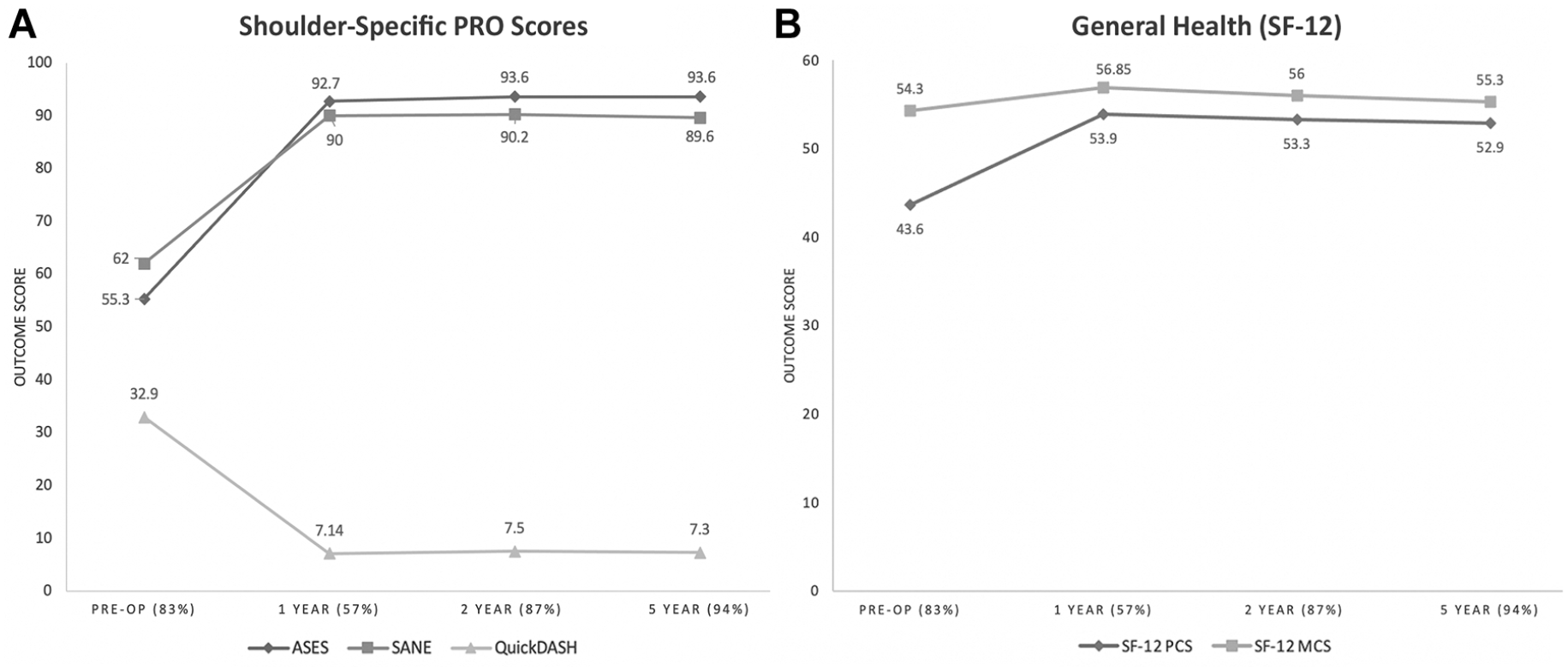
(A) Shoulder-specific PROs and (B) general health (SF-12) scores over time: preoperatively (Pre-op) and 1, 2, and ≥5 years postoperatively. ASES, American Shoulder and Elbow Surgeons; MCS, Mental Component Summary; PCS, Physical Component Summary; PRO, patient-reported outcome; QuickDASH, shortened version of Disabilities of the Arm, Shoulder and Hand; SANE, Single Assessment Numeric Evaluation; SF-12, 12-Item Short Form Health Survey.
Recreational Activities
Patients reported significant improvements in all questions related to sports participation and pain related to activity when compared pre- to postoperatively (Table 3). Also, 63% of patients reported returning to their preoperative fitness program and 33% said they “somewhat” returned to their preoperative program. Notably, the median response for shoulder function during recreational activity was “normal” at the final follow-up compared with “very difficult” preoperatively (P < .001). However, at the final follow-up, 37.3% of patients had modified their recreational sporting activity. The most common reasons for activity modification were lifestyle changes, fear of reinjury, and/or weakness. As expected, patients who did not report modifying their activities had superior ASES (96.8 vs 84.6; P < .001), SANE (94.8 vs 76.1; P < .001), and QuickDASH (6.6 vs 18.1; P < .001) scores in addition to having a higher median satisfaction with surgical outcomes (10 vs 7; P < .001).
Sports Health and Pain-Specific Questions a

Bold P values indicate statistically significant differences from preoperative to postoperative outcomes (P < .05). Postop, postoperatively; Preop, preoperatively.
Survivorship, Satisfaction, and Complications
Kaplan-Meier survivorship analysis demonstrated survivorship rates of 98% at 5 years and 92% at 10 years. While the satisfaction with surgical outcomes was excellent (median, 10) in the collective patient cohort, 10 patients (16.1%) had a satisfaction of <7. Of whom, 4 (6.4% of entire cohort) had corresponding ASES scores of <75, which were deemed “poor outcomes.” This subgroup of did not differ in any measured preoperative or surgical characteristics when compared with the entire study cohort but did report moderate (3) or severe (1) pain with recreation and mild (2) or moderate (2) pain with sleep. One shoulder underwent lysis of adhesions for stiffness 3 months postoperatively. This patient experienced no further complications and reported satisfaction of 10, an ASES score of 100, and a SANE score of 99 at a 5.2-year follow-up. Of note, 1 patient with a minimum 5-year follow-up was included in the final analysis despite reinjuring their index shoulder 10 years postoperatively. The MRI scan demonstrated an intact rotator cuff, but the patient did have signs of osteoarthritis progression. The patient opted to undergo physical therapy rather than further surgical intervention. No patients progressed to an arthroplasty procedure during the study period.
Discussion
The principal findings of the present study are that in physically active patients who are ≥70 years old, arthroscopic RCR produced excellent clinical outcomes and low revision rates at a minimum follow-up of 5 years. Patients experienced significant improvements in PROs, were able to effectively return to their recreational activities, reported decreased pain, and were highly satisfied with their surgical outcomes. These improvements were illustrated at their 1- and 2-year follow-up time points and were maintained through a mean follow-up of approximately 8 years. Additionally, arthroscopic RCR in this patient cohort exhibited an exceptional survivorship rate of 98% and 92% at 5- and 10-year follow-ups, respectively. However, approximately one-third of patients modified their recreational activities at the final follow-up.
As a result of the aging demographics in modern society in conjunction with elderly patients increasingly expressing the desire to remain active, the optimal management of rotator cuff tears in older patients has become a topic of growing interest. Despite the physiologic disadvantages to healing and high retear rates previously discussed, a systematic review evaluating the effectiveness of rotator cuff tears in 680 elderly patients by Altintas et al 4 reported mean postoperative ASES scores of 87.9 at a minimum follow-up of 2 years. The study group also reported improvements in pain and high rates of patient satisfaction, concluding that RCR is an effective treatment option in properly indicated elderly patients. These findings align with the presented study, where exceptional final follow-up ASES (93.6), SANE (89.6), and QuickDASH (7.3) scores were illustrated.
The present study demonstrates that the clinical outcomes and high return to sports rate published by Bhatia et al 5 after a minimum 2-year follow-up do not deteriorate when follow-up is extended to a minimum 5-year follow-up. The findings in this study also indicate that older patients who are active preoperatively achieve significant improvements in function after arthroscopic RCR, which allows for a high rate of return to their recreational activities. Furthermore, these improvements are maintained over time without signs of outcome deterioration as patients age, which is evidenced by the high level of activity shown at a mean follow-up age of >80 years. While the sustained benefit of RCR at mid- and long-term follow-ups has been previously shown,16,25 a relative paucity of literature remains to illustrate these findings in the elderly population, with the majority of studies reporting a mean 2- to 4-year follow-up. 4 One retrospective case series by Plachel et al 28 reported a mean 7-year follow-up on 31 shoulders undergoing RCR at age >75 years, showing a Subjective Shoulder Value of 90% and an ASES score of 89, both of which are comparable with the presented findings. However, their study was limited by a relatively small cohort, with a 74% follow-up rate (n = 23 shoulders). The sustained PRO improvement in the present study reinforces the short-term findings of Altintas et al 4 and midterm findings of Plachel et al, 28 strengthening the conclusion that the arthroscopic RCR in elderly patients is an effective and durable intervention.
In addition to the improved shoulder-specific outcomes discussed above, high levels of general physical and mental health were exhibited as indicated by the SF-12 scores of the cohort. SF-12 PCS scores (physical health) improved significantly to 53, and MCS (mental health) scores remained high (55.3) at the final follow-up, each of which was superior to previously published values 15 of 41.6 (PCS) and 52.1 (MCS) in patients aged 75-79 years. With the present-day aging demographics and increasing demands of older patients to remain active, preserving shoulder function may be a key factor to upholding overall patient health and quality of life. While this relationship is undoubtedly multifactorial, increasing physical activity and decreasing sedentary lifestyle habits have been shown to be associated with improved mental and physical health as people age.1,2,31
Despite the overall high patient satisfaction with surgical outcomes and return to prior activities in the present study, there were 10 patients (16%) who reported satisfaction scores <7; of 4 (6.4% of entire cohort) of whom were deemed to have “poor” outcomes because of corresponding ASES scores of <75. Interestingly, each patient reported moderate (3) or severe (1) pain with recreation and mild (2) or moderate (2) pain with sleep, indicating that pain resolution is likely a central focus of this patient cohort. Additionally, approximately one-third of patients (37.3%) modified their recreational activities postoperatively. While there were no preoperative or surgical characteristics associated with decreased satisfaction or modification of activities, there may be additional contributing postoperative factors, such as health issues related to aging (degenerative arthritis, cardiopulmonary disease, or other systemic illness) that were not evaluated. Given that these patients commonly reported pain as a symptom, it is plausible that they could have developed osteoarthritis, a retear of their rotator cuff, or another pain-generating pathology. Attention to and addressing postoperative patient pain may result in even better patient outcomes than are reported in this cohort study.
Limitations
While this study had many clinically useful findings, it is not without limitations. First, the presented study was retrospective in nature, which carries intrinsic limitations such as recall bias. This limitation was minimized by the use of prospectively collected patient data. Next, this study took place at a high-volume sports medicine referral center, where procedures were performed by a single surgeon. The patients treated at this sports medicine center include a high percentage of motivated and active patients; therefore, their outcomes may not be generalizable to all patients. However, this also serves as a strength of the study, as it provides findings specific to active older patients treated by an experienced surgeon. Additionally, there were no structural imaging findings or clinical examinations at the final follow-up included in this study that prevented the identification of asymptomatic retears or progression of glenohumeral osteoarthritis, although radiographs and MRIs were always obtained in symptomatic patients. A further limitation of the study is that multiple repair techniques were used (DR and SR) and the study was not designed or powered to compare the outcomes of the 2 techniques.
Conclusion
Arthroscopic RCR in active patients ≥70 years old results in sustained improvements in function, less pain, and return to activities. Despite one-third of patients modifying their recreational activity, the cohort reported high levels of satisfaction and general health, supporting the use of RCR as a means of preserving older patients’ quality of life and activity level.
Footnotes
Final revision submitted January 30, 2023; accepted February 13, 2023
One or more of the authors has declared the following potential conflict of interest or source of funding: Grant support for this study was received from Arthrex (grant IIRR-01051). This study was supported by the Steadman Philippon Research Institute (SPRI), which is a 501(k) nonprofit institution. During the past calendar year, the SPRI has received grant funding or in-kind donations from Arthrex, DJO, Ossur, Siemens, Smith & Nephew, and XTRE. R.B.P. has received research support from Arthrex; education payments from Medical Device Business Services, Pinnacle, and Smith & Nephew; and hospitality payments from Exactech. L.B.V. has received education payments from Arthrex and consulting and nonconsulting fees from Smith & Nephew. P.J.M. has received research support from Arthrex, Ossur, Siemens, and Smith & Nephew; consulting fees and nonconsulting fees from Arthrex; and royalties from Arthrex, Medbridge, and Springer; and has stock/stock options in VuMedi. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Vail Health Hospital (ref No. 2021-067).