
Abstract
Background:
Graft-tunnel mismatch (GTM) is a common problem in anterior cruciate ligament (ACL) reconstruction (ACLR) using bone–patellar tendon–bone (BPTB) grafts.
Hypothesis:
Application of the “N+10 rule” in endoscopic ACLR with BPTB grafts will result in acceptable tibial tunnel length (TTL), minimizing GTM.
Study Design:
Controlled laboratory study.
Methods:
Endoscopic BPTB ACLR was conducted on the paired knees of 10 cadaveric specimens using 2 independent femoral tunnel drilling techniques—accessory anteromedial portal and flexible reamer. The graft bone blocks were trimmed to 10 × 20 mm, and the intertendinous distance (represented by “N”) between the bone blocks was measured. The N+10 rule was used to set the angle of the ACL tibial tunnel guide to the appropriate number of degrees for drilling. The amount of excursion or recession of the tibial bone plug in relation to the anterior tibial cortical aperture was measured in both flexion and extension. A GTM threshold of ±7.5 mm was set based on prior studies.
Results:
The mean BPTB ACL intertendinous distance was 47.5 ± 5.5 mm. The mean measured intra-articular distance was 27.2 ± 3 mm. Using the N+10 rule, the mean total (flexion plus extension) GTM was 4.3 ± 3.2 mm (GTM in flexion, 4.9 ± 3.6 mm; GTM in extension, 3.8 ± 3.5 mm). In 18 of 20 (90%) cadaveric knees, the mean total GTM fell within the ±7.5-mm threshold. When comparing the actual measured TTL to the calculated TTL, there was a mean difference of 5.4 ± 3.9 mm. When comparing femoral tunnel drilling techniques, the total GTM for the accessory anteromedial portal technique was 2.1 ± 3.7 mm, while the total GTM for the flexible reamer technique was 3.6 ± 5.4 mm (P = .5).
Conclusion:
The N+10 rule resulted in an acceptable mean GTM in both flexion and extension. The mean difference between the measured versus calculated TTL using the N+10 rule was also acceptable.
Clinical Relevance:
The N+10 rule is a simple and effective intraoperative strategy for achieving desired TTL regardless of patient-specific factors to avoid excessive GTM in endoscopic BPTB ACLR using independent femoral tunnel drilling.
Bone–patellar tendon–bone (BPTB) is a widely used graft choice in anterior cruciate ligament (ACL) reconstruction (ACLR).1,24 The BPTB graft provides advantages in overall graft strength, single-incision technique, bone-to-bone healing, and aperture fixation. 24 Despite the many advantages of BPTB grafts, graft-tunnel mismatch (GTM) is one of the potential complications encountered.5,23 In its simplest form, GTM refers to a discrepancy between the relative length of the BPTB graft and the tibial tunnel length (TTL). Clinically, this manifests with either the tibial bone plug's recessing within the tibial tunnel or protruding out of the anteromedial tibial aperture after femoral fixation. The end result is less bone plug present (or easily accessible) within the tibial tunnel, which can compromise, or in some instances prevent interference screw fixation. Further, as interference fixation with screws has been shown to be the optimal fixation strategy in BPTB ACLR,3,13,14 GTM that compromises this fixation could lead to failure of the reconstruction.
The rate of GTM in ACLR using BPTB autografts is reported to range between 13% and 26% in the current literature.19,23,26 This rate is suggested to be even larger in situations in which a BPTB allograft is utilized.15,23 The etiology of GTM is likely a combination of both differences in surgical technique and anatomic variation between patients, specifically intertendinous distance (N) and intra-articular distance (IAD). Although anatomic variability likely plays a role, multiple studies evaluating differences in patellar tendon lengths, IAD, patient height, and sex show variable results with moderate to no association with GTM.4,6,7
Several approaches have been developed in an attempt to mitigate GTM.4,11,15,17,23,26 Unfortunately, most of these direct measurement or indirect estimation techniques are based on transtibial ACLR and often involve cumbersome and subjective intraoperative measurements. Other authors have suggested modifying the graft itself or adjusting the femoral tunnel to make up for the mismatch. Graft rotation, bone block trimming, femoral tunnel recession, or the use of free bone blocks have all been proposed; however, these methods pose the obvious risk of damage to the graft or compromises in fixation.9,23,25,26 In lieu of making potentially difficult or detrimental changes to the surgical technique, the graft itself, or the fixation method, Miller and Hinkin 17 proposed the N+7 rule as a simple intraoperative strategy to approximate the ideal length of the tibial tunnel. This method simply adds 7° to the measured intertendinous distance of the BPTB graft (represented by “N”) to provide a value to set the endoscopic ACL tibial drill guide. This method was created based on the routine use of 25-mm bone plugs and transtibial ACLR techniques. In 2005, Verma et al 26 suggested the “N+10” modification to more aptly mitigate GTM with more modern anatomic techniques, but they never formally validated this strategy. This method is employed in a similar fashion but differs by adding 10° to the intertendinous distance to set the tibial guide angle.
In this cadaveric study, we sought to critically evaluate the N+10 rule and its ability to consistently provide tibial tunnels of acceptable lengths in BPTB ACLR with independent femoral tunnel drilling and interference screw fixation. To assess this strategy, the threshold for “acceptable” mismatch was set at ±7.5 mm of extrusion or recession of the tibial bone block in relation to the tibial tunnel aperture. This threshold was selected based on biomechanical BPTB ACLR screw data showing that the failure load strength of a standard 20 mm–long interference screw remained equal to a 12.5-mm screw. 2 We hypothesized that the N+10 rule would provide a reliable estimation of TTLs in this series.
Methods
A total of 20 paired knees from 10 fresh-frozen cadaveric specimens (5 female and 5 male specimens; mean age, 56.4 years [range, 37–68 years]) were obtained via a personal research fund purchase. The characteristics of the specimens are shown in Table 1. There were no documented prior surgical procedures involving any of the knees. Each pair of knees (right and left) underwent endoscopic BPTB ACLR with an independent femoral tunnel drilling technique. The procedures were performed by 3 members of the sports medicine faculty (M.D.M, D.R.D. and F.W.G.).
Demographic Characteristics and Cause of Death of Cadaveric Specimens Used in This Study a

Mean age, 56.4 years (range, 37–68 years); 5 male and 5 female specimens.
BPTB Graft Harvest
Each cadaveric knee was potted securely in a leg holder and the knee was allowed to flex to 90° with gravity. A standard medial parapatellar anterior incision was made, and the central one-third of the patellar tendon was identified. A 10-mm catamaran graft knife (Depuy Mitek Inc) was used to harvest a uniform 10 mm–wide graft for all specimens. A reciprocating saw was used to harvest the tibial and patellar bone blocks in a standard fashion. The bone blocks were uniformly trimmed and carefully contoured to 10 mm in width and 20 mm in length for all specimens by attending orthopaedic surgeons (M.D.M., D.R.D.). The intertendinous distance between the bone blocks was measured in millimeters and recorded.
Femoral Tunnel Preparation
The native ACL was arthroscopically debrided, exposing both the tibial and the femoral footprints. For each cadaveric specimen, the right and left knees were equally divided into 2 groups for femoral tunnel drilling—an accessory anteromedial portal technique (n = 10), or a flexible reamer technique through a standard medial portal (n = 10). Two femoral tunnel drilling techniques were employed to mimic real-life scenarios where either method is commonly used.
For the accessory anteromedial portal technique, an accessory medial portal was created under direct visualization. A 6-mm over-the-top guide was placed through this portal and anchored on the back wall of the lateral femoral condyle with the knee held in 120o of hyperflexion. A guide pin was drilled in the anatomic ACL footprint and reassessed before reaming. A rigid 10-mm acorn reamer was then used to create the tunnel with the knee still held in hyperflexion. The tunnel was drilled to a depth of 25 mm using the calibration on the reamer. We reamed to 25 mm for the 20-mm bone block to ensure we were not hindered when pulling the bone plug flush to the femoral aperture.
For the flexible reamer technique, with the knee remaining at 90° of flexion, a 6-mm over-the-top guide was placed through a standard medial portal and again anchored on the posterior wall of the lateral femoral condyle. A flexible guide pin was drilled and the location of the femoral tunnel was confirmed. The pin was overdrilled with a 10-mm flexible reamer (Versi-Tomic system; Stryker) also to a depth of 25 mm based on the reamer calibrations.
Tibial Tunnel Preparation
For tibial preparation, the proposed N+10 rule was used to set the angle of the ACL tibial tunnel guide (Arthrex) to the appropriate degree setting for drilling. To employ the N+10 rule, the intertendinous distance between the bone plugs of the BPTB ACL graft (“N”; in millimeters) was measured (Figure 1).

An intraoperative photo of a bone–patellar tendon–bone anterior cruciate ligament autograft showing the intertendinous distance (“N”; 55 mm) between the bone plugs.
Once measured, 10° was added to this number and that sum value was used to set the tibial guide drill angle (N +10°). For example, if the intertendinous distance on a BPTB graft measured 55 mm, the tibial guide would be set to 65° and drilled in a standard fashion at the anatomic tibial ACL footprint (Figure 2). When drilling the tunnel, care was taken to ensure that the guide arm was parallel to the tibial plateau to avoid artificially changing the degree of drilling and thus the TTL (Figure 3).

An intraoperative photo of the tibial ACL guide (Arthrex) being set using the N+10 rule. Given the intertendinous distance of 55 mm (as measured in Figure 1), the guide angle for drilling was set to 65°. The inset shows that the approximate drilled tunnel length was 50 mm.

An intraoperative photo of the ACL tibial tunnel guide (Arthrex) positioned on the anatomic tibial footprint. The guide is set to 65° (“N” = 55 mm, as shown in Figure 1). Using this angle for the guide, the TTL is estimated to be 50 mm (inset). Notice how the guide is positioned parallel to the tibial articular surface for accurate distances. ACL, anterior cruciate ligament; TTL, tibial tunnel length.
Externally, the guide was placed on the anterior tibia midway between the tibial crest and the posterior tibia externally for a uniform tunnel starting point. With the knee at 90° of flexion, a guide pin was advanced through the tibial ACL guide, and the appropriate location on the ACL footprint was confirmed. The tibial tunnel was then drilled using a rigid 10-mm fully threaded reamer. Soft tissue and bony debris were arthroscopically cleared from each tunnel to allow for easy graft passage and accurate measurements.
Measurements
Direct measurements of the TTL and IAD were then obtained using an arthroscopic calibrated measurement device with the knee at 90° of flexion. For the IAD, the ruler was delivered through the tibial tunnel and held at the central position of the femoral tunnel aperture under direct arthroscopic visualization. The length from the aperture of the femoral tunnel to the intra-articular aperture of the tibial tunnel was visualized and recorded. We then measured the actual length of the prepared tibial tunnel using the arthroscopic ruler. The tibial tunnel was measured from the central intra-articular tibial tunnel aperture to the center of the aperture on the anteromedial tibial cortex after soft tissues were removed to reveal the cortical margins.
Once measurements were obtained, the prepared BPTB graft was secured into the femoral tunnel with the bone plug flush with the aperture using a 7 × 20–mm metal interference screw (Versi-Tomic; Stryker). Care was taken to not countersink the graft within the 25-mm tunnel. After the femoral side of the BPTB graft was appropriately secured, maximal tension was placed on the sutures emanating from the tibial bone plug. The amount of excursion or recession of the tibial bone plug in relation to the anterior tibial cortical aperture at the 12 o'clock position was measured at both 90° of flexion and full extension (Table 2).
BPTB Graft, Tibial Tunnel, and Mismatch Measurements a
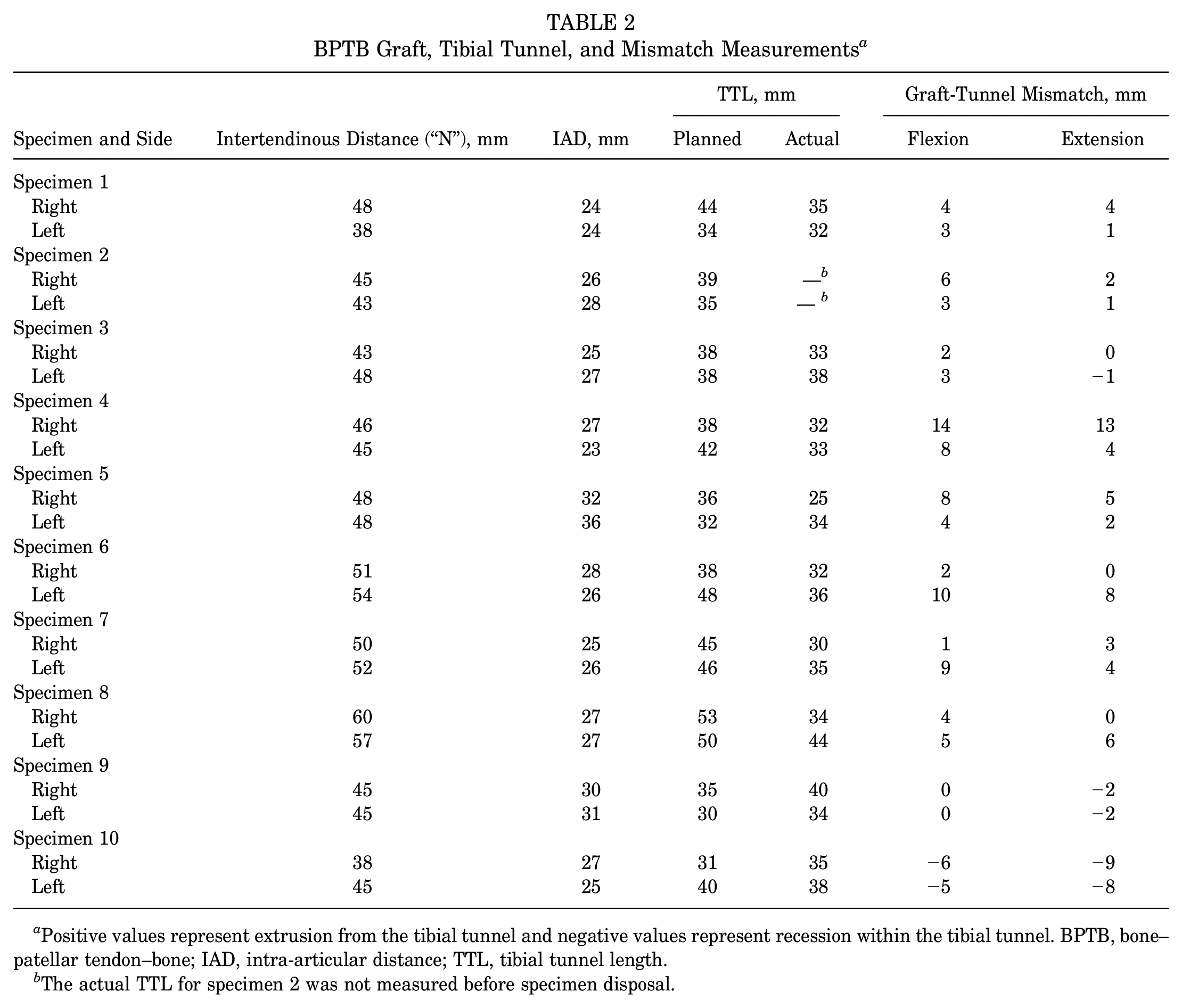
Positive values represent extrusion from the tibial tunnel and negative values represent recession within the tibial tunnel. BPTB, bone–patellar tendon–bone; IAD, intra-articular distance; TTL, tibial tunnel length.
The actual TTL for specimen 2 was not measured before specimen disposal.
Statistical Analysis
To assess mismatch, descriptive statistics were calculated and presented as means and standard deviations. The mean mismatch was individually calculated for both flexion and extension in all 20 specimens. The mean total mismatch (the mean of the sum of flexion and extension mismatch) was also calculated. A threshold of ±7.5 mm was used to define the acceptable amount of mismatch. This value was chosen based on prior biomechanical aperture fixation studies that showed only 12.5 mm of screw and bone plug interface is needed to achieve equal stiffness, displacement, and failure load strength compared with the standard 20 mm–long interference screw. 2 Additionally, a bone plug recessed ≤7.5 mm is a reasonable distance to still visualize and accurately place an interference screw. The Shapiro-Wilk test was used to assess the normality of data distribution. The Student t test was used to compare mean values.
A subgroup analysis was performed to compare the mismatch that resulted from the accessory anteromedial portal and flexible reamer femoral preparation techniques. Although 2 independent femoral tunnel drilling techniques were used, the femoral bone plug was fixed flush at the femoral aperture in both methods. Fixation at the femoral aperture allows for visualization of the bone-screw interface and also prevents graft abrasion at the anterior lip of the femoral tunnel. 10 As most prior studies reporting on mismatch are based on transtibial drilling techniques, both our accessory anteromedial portal and our flexible reamer techniques were individually evaluated.
As a secondary outcome, the measured TTL after the application of the N+10 rule was compared with the predicted TTL for each knee. The predicted TTL was calculated based on the equation IAD+TTL = N+ 20 (size of femoral bone plug in millimeters). This equation requires flush fixation of the femoral bone plug at the femoral aperture (Figure 4).
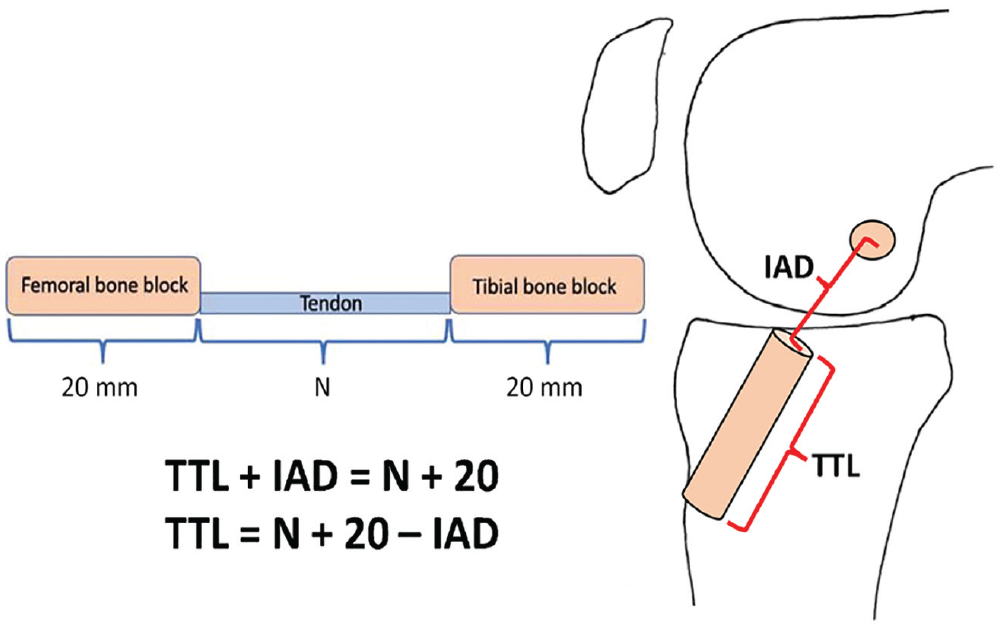
A derived formula for calculating the predicted TTL using the IAD and the known measured value of the intertendinous distance (N) and the set lengths of the bone blocks (20 mm). IAD, intra-articular distance; TTL, tibial tunnel length.
Solving the equation for TTL (TTL = N+ 20 –IAD) allowed the planned TTL to be calculated for each cadaveric knee and compared with the measured values (Table 2).
Results
The mean BPTB ACL intertendinous distance was 47.5 ± 5.5 mm (range, 38-60 mm) and the mean IAD was 27.2 ± 3 mm (range, 23-36 mm), which were both similar to previously published values.7,18,23 Using the N+10 rule, the mean mismatch of the tibial bone block relative to the tibial tunnel was 4.9 ± 3.6 mm and 3.8 ± 3.5 mm in flexion and extension, respectively. As a representative value for the total GTM, the mean mismatch of both flexion and extension for all specimens was 4.3 ± 3.2 mm.
The mean total mismatch as well as the mean individual flexion and extension mismatch values all fell within the ±7.5-mm threshold. Individually, 18 of the 20 cadaveric specimens (90%) tested had combined mean GTM values within that threshold. Mismatch in flexion and extension for each of the specimens was within ±7.5 mm 75% and 80% of the time, respectively. When comparing the actual measured TTL to the calculated TTL, there was a mean difference of 5.4 ± 3.9 mm.
When subcategorizing based on the independent femoral tunnel drilling technique, the mean total mismatch (flexion and extension) for the accessory anteromedial portal technique was 2.1 ± 3.7 mm, while the flexible reamer technique was 3.6 ± 5.4 mm. There was no significant difference in the mean total mismatch when comparing the 2 techniques (P = .5).
Discussion
The primary finding of this investigation is that the N+10 rule is a reliable method of achieving desired TTL to avoid GTM in BPTB ACLR with independent femoral tunnel drilling. Using this tunnel estimation technique, the cadaveric ACLRs demonstrated a mean total (combined flexion and extension) as well as individual flexion and extension mismatch values that fell within a clinically relevant ±7.5-mm threshold in 90% of specimens. Additionally, there was only a 5.4-mm mean difference in actual versus calculated TTLs (also within ±7.5 mm), further supporting the ability of the N+10 rule to provide an appropriate TTL.
There have been a number of strategies developed to estimate, calculate, or directly measure the TTL to avoid GTM, albeit with variable and unvalidated results.4,6,12,15 Shaffer et al 23 prospectively applied a direct measurement technique where the patellar tendon length as well as the IAD was measured during surgery using an arthroscopic measurement device. Despite these patient-specific measurements, the authors still found mismatch in 26% of their 34 consecutive patients. In a slight variation of this method, Hartman and Sisto 11 described a method to directly measure the drilled TTL and IAD as to allow for femoral tunnel recession with modest results in their small series. Although debated, a number of authors have raised concerns with femoral tunnel recession, as it puts the graft at risk for abrasion failure at the anterior femoral tunnel aperture and reduces bone block visibility during interference screw fixation. 10 In a study evaluating the true reliability of direct arthroscopic measurements, Dwyer et al 8 found that the correlation between arthroscopic and open measurements of femoral and tibial tunnels was good at >0.9; however, IAD had a poor correlation between arthroscopic and open measurements (kappa coefficient = 0.4) and only moderate interrater reliability. Direct measurement strategies do have a role and provide value in avoiding GTM, but the measurements have inherent variability and can often be cumbersome and time-consuming during surgery.
Another option for estimating and preventing GTM is directly measuring the length of the harvested BPTB graft and adjusting the tibial tunnel accordingly. In 1996, Miller and Hinkin 17 proposed the N+7 rule as an indirect estimation strategy to estimate the required TTL. The N+7 rule simply requires measuring the intertendinous distance between the bone plugs of the BPTB graft in millimeters and adding 7° to this value to determine the angle of the tibial tunnel drill guide. In their cadaveric series, to evaluate this strategy, the authors reported that nearly 90% of the cadaveric ACLs achieved acceptable length. Others have found less reliable results with this technique, noting only a 50% success rate. 21 Verma et al 26 in 2005 and Miller 16 in 2018 suggested the modification of the N+7 rule to the N+10 rule; however, they did not formally evaluate its applicability. Anecdotally, in more modern, anatomic ACLRs utilizing independent femoral tunnel drilling, the N+7 rule seemed to underestimate the TTL required to match the grafts.
Based on the findings of the present study, the N+10 rule provided a reliable estimate of the required TTL. The mean mismatch between flexion and extension fell within an acceptable threshold to maintain maximal fixation strength in the interference screw. Additionally, the calculated versus actual tibial tunnel length was within 5.4 mm, on average. These were favorable results despite the fact that mismatch measurements were assessed on the superior cortical (12 o'clock position) aspect of the tibial tunnel, with more bone present posteriorly. Of note, there was less GTM seen in extension compared with flexion in the present series, which we feel is important, as grafts are typically secured in extension. 22
It is important to critically appraise the results of this study with the understanding that subtle differences in tibial tunnel guide placement can significantly alter the TTL. Slight alterations in knee flexion angle or slight superoinferior tilt of the tibial tunnel guide with relation to the tibial plateau can artificially lengthen or shorten the tibial tunnel. Although there is certainly a degree of mismatch still present with our findings, one must also keep in mind that this is an estimation strategy. Despite the expected inherent user inconsistency in tibial guide use, the level of mismatch found did not routinely compromise fixation. The N+10 rule is also an indirect estimation strategy that provides the additional benefit of avoiding multiple intra-articular measurements that are subject to aforementioned interobserver variability and error. 8 Finally, there is no need to alter or compromise the harvested BPTB graft or femoral tunnel.
Limitations
This cadaveric study has several limitations. No a priori power analysis was performed; thus, only the 20 paired knees available were used. The smaller number of specimens can potentially explain some of the variability represented by the elevated standard deviations, but the number included in our analysis was similar to prior cadaveric GTM studies.15,20 As per the methods, the application of a handheld tibial guide has inherent user variability, potentially affecting our consistency and internal validity. Although care was taken in our study to keep the tibial guide parallel with the tibial plateau with the knees flexed to 90°, there was no external control of these variables during our ACLRs. This, however, is representative of ACL tibial tunnel drilling in practice. Additionally, prior to direct measurement of the actual TTL, cadaveric specimen 2 was unfortunately disposed of; thus, we were not able to include the full 20 specimens in this part of the analysis. The results of the present study are not applicable to those utilizing suspensory fixation in BPTB ACLR, as the ±7.5-mm threshold used for analysis was based on interference screw fixation. Finally, the endoscopic measurement of the IAD and the tibial tunnel in the center of the apertures has inherent subjectivity and room for error in measurement as shown in previous reliability studies. 8
Conclusion
For ACL tibial tunnel drilling using independent femoral tunnel drilling and a BPTB graft, the N+10 rule resulted in an acceptable average GTM in both flexion and extension. The mean difference between the measured versus calculated TTL using the N+10 rule was also acceptable.
Footnotes
Final revision submitted January 8, 2023; accepted January 30, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.E.D. has received education payments from Arthrex and hospitality payments from Stryker. I.S.M. has received education payments from Medwest. T.E.M. has received education payments from Fortis Surgical. B.C.W. has received education payments, consulting fees, and nonconsulting fees from Arthrex and hospitality payments from Integra LifeSciences. F.W.G. has received education payments from Fortis Surgical; consulting fees from DePuy/Medical Device Business Services and OsteoCentric Technologies; nonconsulting fees from Arthrex; royalties from OsteoCentric Technologies and Smith & Nephew; and hospitality payments from Stryker. M.D.M. has received consulting fees from Arthrex and Ipsen Bioscience; nonconsulting fees and royalties from Arthrex; and honoraria from Encore Medical. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.