
Abstract
Background:
Graft-tunnel mismatch (GTM) is a condition in which the anterior cruciate ligament (ACL) graft is either too long or too short. GTM is particularly problematic when bone–patellar tendon–bone grafts are used because of a potential compromise in fixation of the bone plug on the tibia.
Hypothesis:
The Blumensaat line (BL), a radiographic landmark representing the roof of the intercondylar fossa, will accurately approximate the native ACL (nACL) length and may aid in the prevention of GTM.
Study Design:
Cohort study (diagnosis); Level of evidence, 3.
Methods:
A total of 130 patients (66 males, 64 females) underwent direct measurement of the nACL during knee arthroscopy. The lengths of the nACL and patellar ligament (PL) were measured intraoperatively, and BL length was measured on lateral knee radiographs. The nACL length was compared with PL and BL lengths to calculate the absolute difference (AD). Mean AD was calculated and used to determine mean percentage difference (MPD). Pearson correlation coefficients (CC) between BL, PL, and nACL length were calculated, along with inter- and intraobserver reliability coefficients for the measurement of BL.
Results:
For male patients, the mean length of the nACL was 32.5 mm, BL was 30.4 mm, and PL was 49.2 mm. The AD between the BL and nACL was 2.4 ± 1.3 mm, MPD was 2.6% ± 1.9%, and CC was 0.88. The CC between the PL and nACL was 0.08. For female patients, the mean length of the nACL was 30.2 mm, BL was 27.5 mm, and PL was 44.4 mm. The AD between the BL and nACL was 2.7 ± 1.7 mm, MPD was 4.5% ± 2.4%, and CC was 0.93. The CC between the PL and nACL was 0.1. The inter- and intraobserver reliability coefficients for the measurement of BL were 0.86 and 0.83, respectively.
Conclusion:
A strong correlation was found between BL and nACL with a high inter- and intraobserver reliability. This correlation provides a simple and reliable method to closely approximate nACL length before reconstruction and may aid in the prevention of graft-tunnel mismatch.
Keywords
Anterior cruciate ligament reconstruction (ACLR) is a common procedure in orthopaedics, with more than 200,000 cases annually. 17 In general, high success rates are common, but complications can occur both intra- and postoperatively. Intraoperative technical errors, one of which is graft-tunnel mismatch (GTM), have been cited as a major cause of ACL graft failure.
GTM is a situation in which a harvested autograft is either too long or too short. GTM is particularly problematic when bone–patellar tendon–bone (BPTB) grafts are used, due to a potential compromise in fixation of the bone plug on the tibia. 6,7,19 Additionally, patients with patella alta and patella baja have an increased likelihood of GTM when BPTB autografts are used. 1 To ensure optimal graft fixation, careful preoperative planning must be used to prevent the incidence of GTM, which has proven challenging.
The Blumensaat line (BL) is a radiographic landmark seen on lateral radiographs of the knee, representing the roof of the intercondylar fossa. 3,9 This radiographic finding is a common landmark for orientation and guidance of femoral tunnel placement during ACLR and other procedures. 2,8,14 Although a number of reported radiographic measurements and observations of the knee can be made during preoperative planning, no published reports are available that correlate the length of the native ACL (nACL) with the length of BL on preoperative lateral knee radiographs.
The initial phase of this project involved a preliminary study using 18 cadaveric specimens to assess BL as a predictor of nACL length. 11 Before reconstruction, BL was measured on lateral knee radiographs and used to predict appropriate graft length and tibial tunnel length (TTL) for each specimen. 11 ACLR was performed through use of allografts and an anteromedial portal technique. 11 The difference between the predicted and actual TTL was not significant (P = .3), and the mean GTM was –0.9 ± 3.15 mm. 11 The mean percentage difference (MPD) between the BL and the intra-articular graft length was 5.2%. 11 Thus, BL was determined to be an accurate predictor for the length of the tendinous portion of a BPTB graft as well as the TTL. 11
The purpose of this study was to propose a method to closely approximate the length of nACL as well as the intra-articular graft length during ACLR. We hypothesized that the BL would have a significant correlation with the length of the intact nACL.
Methods
Approval was granted by an institutional review board, and informed consent was obtained from each patient.
In total, 130 patients were included in this study. Prior to finalization of participants, we excluded 8 patients because they did not have appropriate corresponding lateral radiographs for comparison. Of the patients included, 66 were male and 64 were female. Participant ages ranged from 15 to 79 years, with the mean male and female ages being 48.6 and 50.1 years, respectively.
Patients were identified and considered for inclusion if they were scheduled for a surgical knee procedure that would permit intraoperative measurement of the nACL. Furthermore, participants were selected for inclusion if they were scheduled for a surgical knee procedure that did not involve treatment of the ACL, were skeletally mature, had an intact ACL at the time of the scheduled procedure, and had appropriate lateral knee radiographs as part of a preoperative series within 12 months of the procedure. Patients were excluded if they had a history of prior ACL injury or reconstruction, had a history of prior injury to or surgical procedure on the patellar ligament (PL), or did not have appropriate lateral knee radiographs within 12 months of the study procedure.
An appropriate lateral knee radiograph was defined as having less than 5 mm of posterior condylar offset, which was based on literature that supports a 5-mm cutoff value for acceptable lateral radiographs. 15 To ensure maximum accuracy, radiographs were taken by a single radiology technician as part of a routine preoperative series, using the same machine for all radiographs in the study. The technician was given specific instructions that included taking all radiographs with the patient’s knee flexed to 30°, centering the knee to the focal spot on the x-ray tube, minimizing source image receptor distance, and minimizing object image receptor distance to reduce image magnification and distortion. A 25-mm radiopaque ball was placed at the level of the femoral notch in 25 of the radiographs to determine the machine’s average degree of magnification and account for distortion.
Intraoperative nACL and PL measurements were conducted before measurement of the BL to avoid potential measurement bias. The PL was measured on each patient, after administration of anesthesia and before the procedure started, with the knee flexed to 90°. Measurements were taken to the nearest millimeter through use of a tape measure and palpated landmarks from the distal pole of the patella to the proximal-most aspect of the tibial tubercle.
The nACL was measured after the administration of anesthesia and early during the procedure. Measurement was obtained at the single point where the origin of the ACL, off the medial aspect of the lateral femoral condyle, and its insertion on the anterior tibia could be seen. This technique involved flexing the knee to 90°, inserting a spinal needle through soft tissues immediately anterior to the ACL, and advancing the needle until reaching the origin on the medial aspect of the lateral femoral condyle (Figure 1). The spinal needle was carefully scored with a grasper at the insertion of the ACL on the tibia, and the distance between the tip of the needle to the score was measured to the nearest 0.1 mm (Figure 2). If necessary, the ligamentum mucosum and fat pad were debrided to allow for optimal visualization and reliability of measurement and landmarks.

Arthroscopic view of percutaneous spinal needle at the origin of the anterior cruciate ligament on the medial aspect of the lateral femoral condyle.
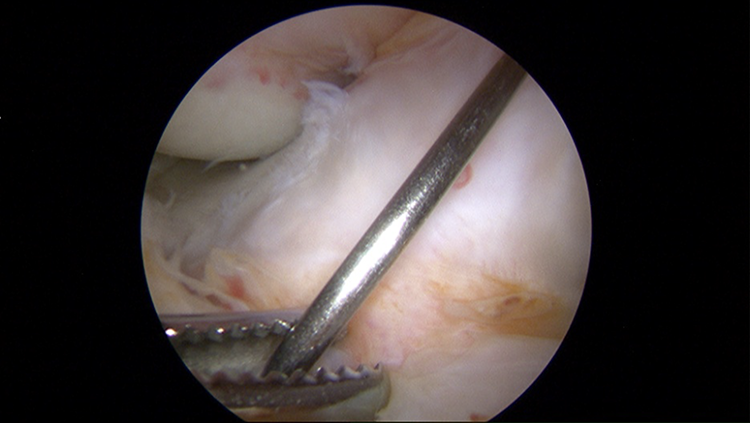
Arthroscopic view of a percutaneous spinal needle at the insertion of the anterior cruciate ligament on the tibia.
The BL was measured on lateral knee radiographs by a single investigator (P.W.J.) (Figure 3), beginning where the anterior condyle cortical density intersected with the anterior femoral notch density and ending at the posterior intersection of the femoral notch density and posterior cortical density at the level of the superior aspect of the posterior condyles. Radiographic measurements were taken through use of the embedded tools within the Picture Archiving and Communication System (PACS) workstation (Version 2.1, Centricity PACS; GE Healthcare Systems), with high-resolution monitors to measure to the nearest 0.1 mm. Using the same workstation, the investigator measured the diameter of the 25-mm ball to determine the degree of magnification for each image. The degree of magnification was averaged over the 25 radiographs to determine the average degree of magnification, which was incorporated into study results, thus minimizing distortion and ensuring the accuracy of the BL measurements.

Measurement of the femoral notch roof (Blumensaat line) on a lateral radiograph.
To establish a degree of intra- and interobserver reliability for this study, we retrospectively reviewed a selection of lateral knee radiographs to repeat the same radiographic measurements. In total, 57 lateral knee radiographs, from 50 individuals (25 males and 25 females), were reviewed by 3 board-certified and sports medicine fellowship–trained orthopaedic surgeons (P.W.J., J.B., R.H.). The lateral knee plain radiograph for each individual was viewed on the same PACS workstation, and measurements of BL were made through use of the embedded tools within this system. Blinded to previous results, the reviewer repeated the above process 6 weeks later, and a new set of measurements was obtained. This procedure was performed for each reviewer.
Statistical analysis was performed separately for male and female patients. The mean length and standard deviation were calculated for nACL, BL, and PL. The absolute difference (AD), MPD, and Pearson correlation coefficient (CC) were calculated between the nACL and BL length, whereas only CC was calculated between nACL and PL length. AD represented the difference between the nACL and BL, regardless of whether the length was longer or shorter. If both the nACL length and BL length were identical, the AD would be 0 mm. The MPD represented any number greater or smaller than 100%, which was the percentage difference between the nACL length and BL length. An MPD less than 5% was considered excellent. A type (3,1) intraclass correlation coefficient (ICC) was calculated for measurements obtained at different sessions (intraobserver reliability) and measurements obtained by different surgeons (interobserver reliability). For CC and ICC, greater than 0.8 was considered excellent and less than 0.2 was considered poor.
Results
For male patients, the mean ± SD length of the ACL was 32.5 ± 3.5 mm with a range of 24 to 42 mm. The mean length of the BL was 30.4 ± 3.0 mm with a range of 24.4 to 38.7 mm, and the mean PL length was 49.2 ± 7.4 mm with a range of 34 to 70 mm. The mean AD between BL and nACL length was 2.4 ± 1.3 mm, MPD was 2.6% ± 1.9%, and CC was 0.88. The CC between the PL and nACL was 0.08.
For female patients, the mean length of the nACL was 30.2 ± 4.8 mm with a range of 22 to 38 mm; BL was 27.5 ± 4.0 mm with a range of 21 to 35.8 mm, and PL was 44.4 ± 5.9 mm with a range of 31 to 58 mm. The mean AD between the length of BL and nACL was 2.7 ± 1.7 mm, MPD was 4.5% ± 2.4%, and CC was 0.93. The CC between the PL and nACL length was 0.1.
The mean ICC of measurements obtained between different surgeons was 0.86, and the mean ICC of measurements obtained by the same surgeon at different sessions was 0.83.
Discussion
The most important finding of this study was a strong correlation between BL and nACL. This correlation may aid in the prevention of GTM, which can occur when an ACL graft is either too long or too short during ACLR. GTM most commonly involves a BPTB graft that is too long, resulting in protrusion of the distal end of the graft out of the tibial bone tunnel. 7 One study demonstrated a 13% rate of GTM overall and a 20% rate of mismatch when BPTB allografts were used. 19 Other studies reported mismatch in as many as 26% of BPTB autografts. 16
A reliable method to closely estimate the length of the nACL preoperatively could help to minimize such complications. Several studies investigated methods of determining ACL length with a goal of minimizing the incidence of GTM. 4,5 One study examined 414 magnetic resonance imaging (MRI) scans of knees with intact ACLs and developed a linear regression formula to calculate the length of the ACL based on the individual’s height. 4 A strong correlation was found between ACL length and patient height. However, no significant association was noted between PL and patient height. That study calculated ACL length (y, in millimeters) as a function of height (x, in inches), expressed as y = 1.17x – 41.29. Although that study showed a strong correlation between height and nACL length, the applicability of this equation is limited, as it is difficult to recall and use practically.
Another study examined 50 knees endoscopically as well as 9 cadaveric knees and reported no statistically significant correlation between nACL and PL. 5 In our study, a similar poor correlation was found between nACL and PL (0.08 in male patients and 0.10 in female patients), but a strong correlation between nACL length and BL length was demonstrated (0.88 in male patients and 0.93 in female patients).
Variability in intra-articular graft length has been noted throughout the literature, with a range of 21 to 33 mm reported in one study and 15 to 26 mm reported in another. 5,16 Our study demonstrated a similar range in ACL length: 24 to 42 mm in male patients and 22 to 38 mm in female patients. This variability stresses the value of knowing the nACL length preoperatively and the ability to make simple calculations and minor changes in technique to avoid or minimize GTM and its inherent compromises.
GTM is more common when the tendinous portion of the graft exceeds 50 mm. 16,20 In our study, the mean length seen was similar to that reported by several others and was demonstrated to be 49.2 ± 7.4 mm in male patients and 44.4 ± 5.9 mm in female patients. 5,16 The range for male PL length was 34 to 70 mm, with 50% (33/66) being 50 mm or longer. The range for female PL length was 31 to 58 mm, with 28% (18/64) being 50 mm or longer.
Several studies have attempted to determine formulas to calculate TTL to accommodate the BPTB graft length. 10,12,13,20 One calculated the TTL by subtracting 50 mm from the overall BPTB graft length. 10 Another used the “N + 7” rule, where the length of tendinous graft (in millimeters) plus 7° is the optimal angle of the tibial guide. 12 A third study recommended a combination of the “N + 7” rule and the “N + 2 mm” rule, where the TTL is PL length + 2 mm. 13 A fourth study used the “N + 10” rule to determine the angle of the tibial guide, with “N” again being the length of the tendinous portion of the BPTB graft. 20 None of these studies addressed the determination of nACL length in their calculations, which can possibly provide a more accurate TTL.
In the current study, a high degree of inter- and intraobserver reliability was found with the measurement of BL length on lateral knee radiographs (0.86 and 0.83). This demonstrates the ease and reproducibility of obtaining an accurate estimate of the nACL length.
One strength of this study was the use of direct in vivo measurements of the nACL and PL, which allowed for direct measurement. MRI is a popular method for obtaining nACL and PL measurements, but quality is often affected by the patient’s ability to remain motionless during a study, body habitus, and the strength of the magnet. Thus, a poor-quality MRI can limit the accuracy of measurements. 18,20,21 In contrast, radiographs offer a more consistent quality and are easily obtained. Additionally, the need for a repeat radiograph (ie, to obtain a “true” lateral knee radiograph) adds little cost and inconvenience. Another strength of this study was separation by sex. Examining the data by sex allowed for stratification of any differences between nACL, BL, and PL lengths in women and men.
We obtained nACL lengths before measuring BL, and observers were blinded to intraoperative results in an attempt to minimize measurement bias, but a potential limitation of this study remains the retrospective collection of radiographic data. All radiographic measurements were dependent on consistent and appropriate lateral radiographs of the knee. Patients with poor lateral knee radiographs were excluded, but variations in the remaining radiographs may have caused inaccurate measurements. Great efforts were taken to minimize such inaccuracies, which included having all radiographs taken by a single technician and providing the technician with specific instructions that included flexing the patient’s knee to 30°, centering the knee on the focal spot on the x-ray tube, minimizing source image receptor distance, and minimizing object image receptor distance. Furthermore, the same machine was used for all radiographs in the study, and a 25-mm ball was used in 25 radiographs to determine the average degree of magnification and adjust study results accordingly. However, source image receptor distance and object image receptor distance were not recorded, and there was no standardized distance for either. Additionally, a standard radiopaque marker could have been used on every radiograph to better correct for magnification and distortion. All of these steps would have further increased measurement accuracy and precision.
Another potential limitation was the method for acquisition of nACL and PL length. The spinal needle was placed just anterior, resting on the ACL, and was therefore more a measurement of the anteromedial bundle. This method was performed to prevent any damage to the nACL during the measurement process. Measurements were also taken with the knee flexed to 90°, at which point the ACL has been shown to be shortest. 22 However, it is unlikely this potential difference has a significant impact on the clinical application of this concept. Nevertheless, given the limitations in measurement and need to preserve ACL integrity during this study, further research using MRI and cadavers (currently under way) is certainly warranted and may provide more insight into this anatomic relationship.
The results of this study were consistent with the data established by our preliminary cadaveric study and demonstrate a high correlation between the length of BL measured on true lateral knee radiograph and the length of the nACL. 11 The MPD between the nACL length and the BL length was 2.6% in male patients and 4.5% in female patients. Additionally, the mean AD in nACL length, compared with BL in male and female patients, was found to be 2.4 and 2.7 mm, respectively. This is the first time that BL length has been shown to correlate highly with the length of the nACL. 9,14 This correlation may help prevent GTM during ACLR with a BPTB graft, because knowing the total length of graft harvested and the intra-articular length of graft needed allows for the adjustment of femoral and tibial tunnels to better accommodate the graft.
Conclusion
A strong correlation was found between BL and the nACL, with a high inter- and intraobserver reliability. This correlation provides a simple and reliable method to closely approximate nACL length before reconstruction and may aid in the prevention of GTM.
Footnotes
Final revision submitted March 3, 2020; accepted March 17, 2020.
One or more of the authors has declared the following potential conflict of interest or source of funding: P.W.J. has received educational support from Supreme Orthopedic Systems and consulting fees from Amend Medical, DePuy Mitek, and RTI and is an employee of PerfectACL App. S.B. has received grant support from DJO, educational support from MVP Orthopedics and Smith & Nephew, and hospitality payments from Zimmer Biomet. J.B. has received educational support from Arthrex and Alpha Orthopedic Systems, speaking fees from Abbott Laboratories, and hospitality payments from Smith & Nephew. T.R. has received hospitality payments from Trimed. R.H. has received educational support from Arthrex and Gemini Medical and hospitality payments from Smith & Nephew. C.L.W. has received educational support from Arthrex and Medwest and hospitality payments from DJO. J.R.A. has received consulting fees from Biomet, Bauerfiend, Theralase, and MiMedx; speaking fees from Halyard and Arthrex; and royalties from Biomet; has stock or stock options in Patient Connection and Connective Orthopaedics; is a board member for FastHealth and Physiotherapy Associates; and is an employee of Biomet, Bauerfiend, Theralase, MiMedx, and Physiotherapy Associates. C.A.R. has received educational support from Arthrex and hospitality payments from Smith & Nephew. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the Baptist Hospital Institutional Review Board (ref No. 457180-1).