
Abstract
Background:
There is evidence on the clinical effectiveness of the Lemaire technique for lateral extra-articular tenodesis (LET) in patients undergoing revision anterior cruciate ligament reconstruction (ACLR), but the best fixation technique is unknown.
Purpose:
To compare the clinical outcomes of 2 fixation techniques after revision ACLR: (1) onlay anchor fixation, which would avoid tunnel conflict and physis injury, and (2) transosseous tightening and interference screw fixation. Pain at the area of LET fixation was also assessed.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
This was a retrospective 2-center study of patients with first-time revision ACLR and either LET with anchor fixation (aLET) with a 2.4-mm suture anchor or LET with transosseous fixation (tLET). Outcomes at minimum 12-month follow-up were assessed with the International Knee Documentation Committee score, Knee injury and Osteoarthritis Outcome Score, visual analog scale for pain at the LET fixation area, Tegner score, and anterior tibial translation (ATT). A subgroup analysis within the aLET group investigated passing the graft over or under the lateral collateral ligament (LCL).
Results:
In total, 52 patients were included (26 patients in each group); the mean ± SD follow-up was 13.7 ± 3.4 months. No statistically significant differences were detected between the groups with respect to patient-reported outcome scores, clinical examination, or instrumented testing (side-to-side difference in ATT at 30° of flexion; aLET, 1.5 ± 2.5 mm; tLET, 1.6 ± 1.7 mm). Clinical failure was detected in 1 patient with aLET and none with tLET. Subgroup analysis revealed a small, nonsignificant flexion deficit in knees in which the iliotibial band strand was passed under (n = 42) or over (n = 10) the LCL. No clinically relevant tenderness was detected at the area of LET fixation in any group (aLET, 0.6 ± 1.3; tLET, 0.9 ± 1.7; over the LCL, 0.2 ± 0.6; under the LCL, 0.9 ± 1.6).
Conclusion:
Onlay anchor fixation and transosseous fixation of the LET were equivalent with respect to outcome scores and instrumented ATT testing. Clinically, there were minor differences in passage of the LET graft over or under the LCL.
The clinical importance of anterolateral rotational instability in cases of anterior cruciate ligament (ACL) insufficiency was recently demonstrated in randomized prospective trials. 7,33 In revision ACL reconstruction (ACLR), an additional lateral extra-articular procedure (LEAP) has been shown to reduce rotational laxity, secondary meniscal injuries, and graft failure rates. 7,13,17
In light of the promising effect in first-time ACLR, LEAP has been of rising interest in revision ACLR given that revision ACLR still yields inferior clinical results as compared with first-time ACLR. 37,40 There exists evidence that LEAP also reduces graft failure rates and leads to higher return to preinjury activity when compared with single ACLR revision. 2,9,18
LEAP can be performed as a lateral extra-articular tenodesis (LET), such as a modified Lemaire tenodesis, which has been shown to be biomechanically equivalent to other LEAPs with respect to rotational control. 13,24 However, there is no consensus about certain technical aspects: the type of graft to use for LET, whether to pass the graft over or under the lateral collateral ligament (LCL), the type of LET fixation to perform, and the force and knee flexion angle to tension the graft. The problem of tunnel interference has been pointed out when using a transosseous drilling technique for LET tightening and fixation (tLET). 14,16 This technique allows for precise tensioning of the graft, which has been reported to be important in biomechanical studies. 11 –13 In comparison, anchor fixation of the LET (aLET) has been described in the literature, but comparative studies of the 2 techniques are missing. 23,30,38 In addition, passing the LET graft under the LCL has demonstrated more isometric behavior as compared with passing it over the LCL. 12,13 With respect to the graft passage relative to the LCL, both techniques have been described in clinical application, but data are limited about its significance for ACLR failure and clinical outcome. 28,32
The purpose of this study was to introduce an aLET in a modified Lemaire technique and conduct a comprehensive clinical comparison with a tLET fixation technique in cases of revision ACLR. In addition, the effect of passing the LET over or under the LCL was investigated to examine whether this makes a difference to the local tenderness at the site of LET.
Methods
Between 2018 and 2021, 52 patients with first-time revision ACLR and additional LET were included in a retrospective, 2-center, multisurgeon study. The fixation technique of the LET was not randomized but depended on the study site. One study site performed tLET fixation, while the other performed aLET. The inclusion criterion was persistent or recurrent instability after first-time ACLR revision. Patients with concomitant meniscal injuries, cartilage defects, as well as anteromedial and posterolateral instabilities were included in the study. Exclusion criteria were first-time ACLR and multiple revision ACLRs (>2), open growth plates, concomitant posterior cruciate ligament injury, posterior slope correction, coronal malalignment (>4°), and knee infection. The study protocol was approved by the local ethics committee, and each study patient provided informed consent.
Surgical Technique of ACLR and LET
Before ACLR, tunnels were filled with allograft bone chips if the preoperative tunnel diameter was >11 mm or if the former tunnel was placed semianatomically. ACLR was carried out 4 to 6 months after tunnel filling. In all cases, coronal and sagittal malalignment was assessed.
All ACLRs were performed with a single-bundle hamstring or quadriceps autograft and anteromedial portal inside-out drilling technique. If the transplant diameter was <7 mm with the semitendinosus tendon, an additional gracilis graft was harvested. Both constructs were femoral fixed using an extracortical adjustable loop system and tibial fixed using an interference screw and additional extracortical button. For ACLR within its anatomic femoral attachment, the anteromedial portion of the ACL footprint was aimed at the femoral side, 26 and 43% of the anteroposterior tibial diameter was aimed at the tibia. 34 Meniscal tears including root tears and ramp lesions were fixed by sutures or transosseous fixation. Medial collateral ligament (MCL) injuries in this study were reconstructed using contralateral hamstring tendons or a peroneal split graft as described previously. 1,3 Cartilage lesions were treated individually following the recommendations of the German Society for Orthopaedics and Trauma Surgery. 25
An adjunctive LET via the modified Lemaire technique was carried out in all cases according to a technique described by Wagner et al. 36 LET preparation was conducted after preparation of the ACL tunnels but before pulling in the ACL graft to avoid any potential tunnel interference. A 4-cm skin incision was made in projection of the lateral epicondyle, and a strip of the distal iliotibial band (ITB) was dissected and cut proximally. In the tLET technique, the proximal end of the strip was whipstitched with a No. 2 FiberWire suture (Arthrex) and passed underneath the LCL. A K-wire was placed proximally and posterior to the LCL footprint with the knee in 110° to 130° of flexion. 16 After isometry testing, the K-wire was reamed with a 4.5-mm drill under direct arthroscopic visualization of the femoral ACL tunnel to avoid tunnel conflict before ACL graft implantation. After ACL graft implantation and fixation, the ITB graft was transosseously tightened manually and fixed with an interference screw at 50° of flexion and neutral rotation.
For the aLET technique, a 2.4 mm metal anchor (FASTak; Arthrex Inc) was placed proximal and posterior to the LCL footprint, and isometry was tested (Figure 1). The decision to pass the ITB strand over or under the LCL during aLET was based on the preference of the 2 surgeons (K.H.F. and M.K.). Afterward the ITB graft was baseball-stitched using one end of the suture-loaded anchor. Fixation was conducted at 45° of flexion and neutral rotation with a sliding knot after implantation and fixation of the ACL graft (Figure 2).
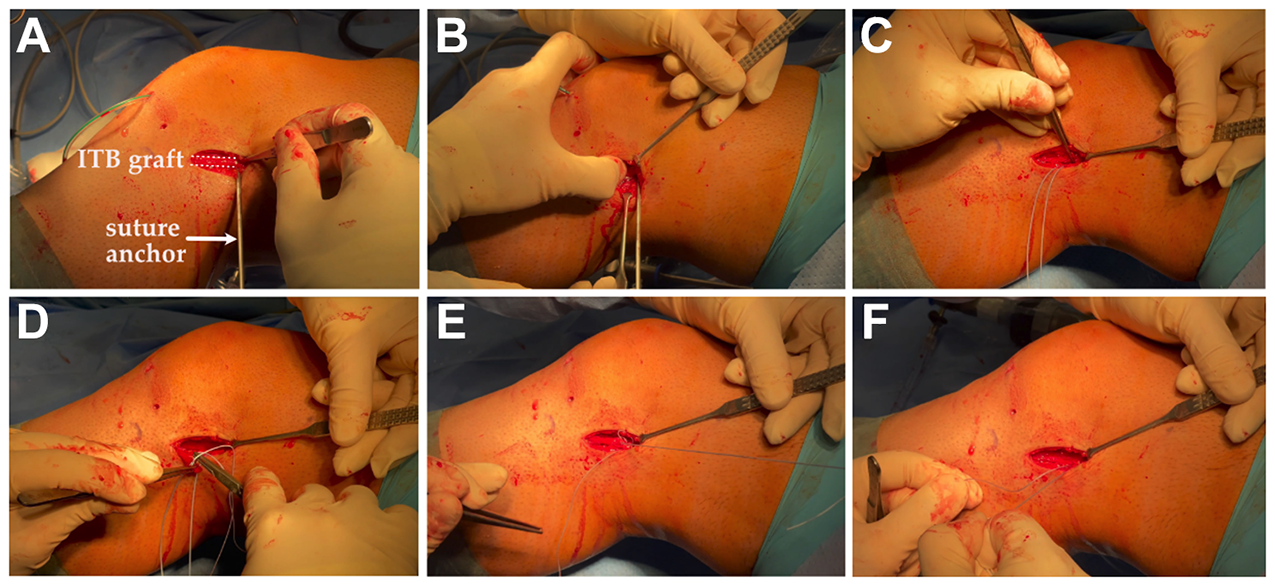
Modified Lemaire technique as lateral extra-articular tenodesis. (A) Based on the previously described technique by Lemaire, an iliotibial band (ITB) strip is prepared and proximally cut. For femoral fixation, a point proximal and posterior to the lateral femoral epicondyle is located, which can be marked with a K-wire for isometry testing. (B) A suture-loaded and self-tapping metal anchor (FASTak; Arthrex) is inserted. (C, D) Depending on the graft strength, the proximal end of the graft can be baseball-stitched beginning at the level of the anchor or distal from it. (E, F) A sliding knot can be used to tighten the graft.

Representative case of a 17-year-old patient who received concomitant anterior cruciate ligament reconstruction and anchor fixation of the lateral extra-articular tenodesis (aLET). (A) Three-dimensional reconstruction and (B) axial computed tomography scan demonstrate the close proximity of the lateral femoral anterior cruciate ligament tunnel exit and its fixation button (ACL fb) as well as the aLET. Drilling for transosseous lateral extra-articular tenodesis can create critical tunnel interference as compared with the aLET.
Postoperative treatment was administered according to a standard protocol after ACLR and revision ACLR. All patients wore a dynamic knee brace (eg, Hypex-Lite; Albrecht) immediately after surgery for 6 weeks and were allowed to fully bear weight from the second week on. Partial weightbearing and limited flexion to 60° were carried out in patients with concomitant meniscal reconstruction, cartilage procedures, and peripheral MCL reconstructions.
Clinical Testing
Follow-up examination was conducted 12 months after the index surgery and included functional outcome scoring systems by Lysholm, Tegner, subjective International Knee Documentation Committee, and Knee injury and Osteoarthritis Outcome Score. Subjective pain during exercise was quantified by visual analog scale (VAS). In addition, tenderness at the LET fixation site during exercise was quantified according to the VAS. The side-to-side difference (SSD) in anterior translation of the tibia (ATT) was measured by Rolimeter (Aircast). In addition, knee stability was measured with the dial test, Lachman classification (grade 0, normal; grade 1, 3-5 mm; grade 2, 6-10 mm; grade 3, >10 mm), and pivot-shift test (grade 0, absent; grade 1, glide; grade 2, clunk; grade 3, gross). Varus and valgus stability was tested at 0° and 30° to evaluate the collateral ligaments. Postoperative clinical failure was defined as SSD in ATT >5 mm or pivot-shift grade 2 or 3.
Statistical Analysis
Data are presented as mean and standard deviation or as absolute value and percentage. Outcomes were compared between patients with aLET and tLET fixation. The primary outcome measure was Instrumented testing results, and the secondary outcome measure was patient-reported outcome scores. Differences between the groups were calculated with the Student t test or the Kruskal-Wallis test for nonparametric parameters. Categorical parameters were compared with the chi-square test, with the Fisher exact test used in case of small subgroups (n < 5). In addition, subgroup analysis was performed by the anatomic course of the ITB graft (over vs under the LCL), and differences were calculated via the Student t test or Mann-Whitney U test. Statistical analysis was performed with Prism Version 8 (GraphPad). P < .05 was considered significant.
Results
Patient Demographics
This study included 52 patients with first-time revision ACLR and additional LET, with a mean ± SD follow-up of 13.7 ± 3.4 months (range, 12.0-20.4 months) (Table 1). An equal number of patients was present in each group (26 aLET and 26 tLET). Reasons for first-time revision ACLR were traumatic accident (58.0%) and nontraumatic graft failure (42.0%), defined as patient-reported instability in addition to objective signs of insufficient ACLR (SSD >5 mm or pivot-shift grade 2 or 3). The latter cases were mainly due to tunnel malpositioning, concomitant MCL and LCL injuries, and idiopathic graft failure. There were no differences between aLET or tLET and ACLR regarding demographic data (P > .05). The radiologic findings (coronal alignment and posterior tibial slope) did not differ in the compared groups. Recurrent surgical intervention after first-time revision ACLR attributed to arthrofibrosis (aLET, n = 2 [7.7%]; tLET, n = 0 [0.0%]; P = .4898) and soft tissue granuloma (aLET, n = 1 [3.8%]; tLET, n = 0 [0.0%]; P = .9999) was nonsignificantly different between the groups.
Preoperative Patient and Injury Characteristics a
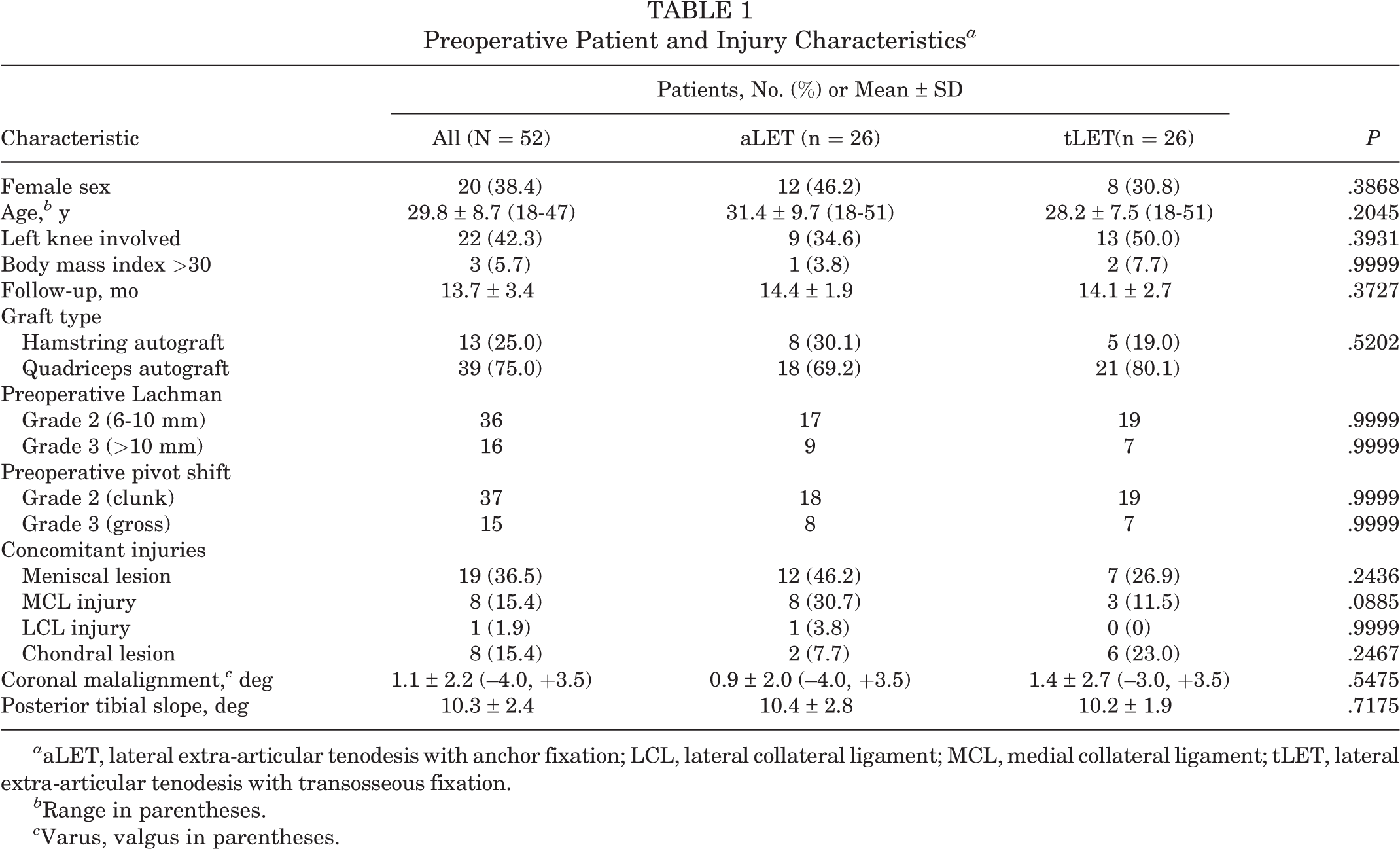
a aLET, lateral extra-articular tenodesis with anchor fixation; LCL, lateral collateral ligament; MCL, medial collateral ligament; tLET, lateral extra-articular tenodesis with transosseous fixation.
b Range in parentheses.
c Varus, valgus in parentheses.
Patient-Reported Functional Outcome
Functional outcome scores at the time of follow-up are given in Table 2. There was no difference between the groups according to VAS, local tenderness in the area of LET fixation, and functional scores. In total, 98.1% of patients (n = 51) would have the same operation again.
Functional Outcome Scores at the Follow-up a

a ADL, Activities of Daily Living; aLET, lateral extra-articular tenodesis with anchor fixation; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; LET, lateral extra-articular tenodesis; tLET, lateral extra-articular tenodesis with transosseous fixation.
Clinical and Instrumented Anterior Laxity Testing
Data of clinical examination and instrumented ATT testing at the time of follow-up are given in Table 3. There was no significant difference in postoperative range of motion and instrumented ATT testing. Lachman grade 1 was minimally less in the tLET group versus the aLET group (P = .0415). Clinical failure was recorded in 1.9% (n = 1) of all cases.
Clinical Examination and Instrumented Stability Assessment at the Follow-up a

a Data are reported as mean ± SD or % unless otherwise indicated. aLET, lateral extra-articular tenodesis with anchor fixation; SSD, side-to-side difference; tLET, lateral extra-articular tenodesis with transosseous fixation.
b Defined as SSD in anterior tibial translation >5 mm or pivot-shift grade 2 or 3.
Results of Subgroup Analysis
There were no differences in VAS, postoperative knee ATT stability (Rolimeter, Lachman), or patient-reported outcome scores between aLET with the graft over the LCL and that under the LCL (Table 4).
Subgroup Analysis Based on the Anatomic Course of the Iliotibial Band Graft for LET a

a IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; LCL, lateral collateral ligament; LET, lateral extra-articular tenodesis; SSD, side-to-side difference.
b Preoperative-postoperative.
Discussion
As the main finding in this study, onlay anchor versus transosseous fixation of the LET procedure with concomitant first-time revision ACLR was not found to cause significant clinical differences at 12-month follow-up. Onlay aLET was clinically established as a reliable and simple alternative to the tLET technique. With respect to local tenderness at the area of LET fixation, there was no clinically significant pain in both groups. In cases with aLET fixation, no significant clinical differences were detected depending on whether the LET graft was passed over or under the LCL.
Clinical effectiveness of LET and anterolateral ligament reconstruction in ACLR was recently demonstrated in large randomized prospective studies. 2,7 However, some technical difficulties have been pointed out regarding the modified Lemaire technique, such as tunnel interference, risk of overconstraint, and physis injury in skeletally immature patients. 11,14,30 Therefore, an anchor-based technique seemed to offer an eligible alternative. Secure evaluation of the anatomic insertion site as well as isometry testing can be performed equally to the transosseous technique with a K-wire. A potential advantage of the transosseous technique may be the precise tensioning of the graft. Yet, recent biomechanical studies revealed that a considerably low tension of 20 N is sufficient to restore intact knee kinematics and avoid overconstraint. 11,12 To our knowledge, no biomechanical study has compared the tensioning properties of various anchor devices. In view of the relatively low graft tensioning needed, however, it is likely that by using a sliding-knot technique and conducting a length-change test of the graft before fixation, adequate tensioning can be realized by the described technique.
Importantly, both techniques resulted in good to excellent clinical outcome as compared with related studies. 2,5,6,9 A recent systematic review reported a mean Lysholm score of 88.9, a subjective International Knee Documentation Committee score of 83.3, and a Knee injury and Osteoarthritis Outcome Score of 68.3 for Sport/Recreation at final midterm follow-up. 9 However, it is known that by first-time revision ACLR the outcome critically depends on concomitant injuries, patient age, sporting demands, and follow-up, which compromises this comparison. 1,7,29 The overall failure rate was 3.6% in ACLR with additional LET, which again depends on the previously mentioned criteria and graft selection. 9,29 No significant clinical differences were detected in this study with respect to the utilized LET technique. In addition to the studied patient-reported outcomes, there was no reoperation for recurrent meniscal injuries in both groups, which would be indicative for persistent instability.
SSD measurement of ATT in ACLR and concomitant LET has been reported 22 to be 2.4 mm, which was lower in our study. This may be due to a selection of first-time revision ACLR and an early outcome measurement. Although no significant differences in ATT were measured, we acknowledge that the complex biomechanical behavior of residual anterolateral rotatory instability cannot be sufficiently assessed by an instrumented ATT test. Pivot-shift grading highly depends on the examiner and cannot differentiate between ATT and the amount of rotatory laxity, which is why its validity as an outcome parameter in ACL surgery is limited. 20
Many biological and biomechanical features (eg, maximum load to failure and mode of failure) can be discussed for different soft tissue–bone fixation techniques. 4 Recent studies have investigated the concept of onlay fixation using different metal or soft tissue anchors. 8,19,21 Clinical studies comparing onlay and intraosseus screw fixation are missing, but a recent animal study examined the biological properties of an onlay MCL fixation, which demonstrated nonsignificant differences when compared with the native MCL. 35 These results are in line with clinical data showing good to excellent results of ligament fixation using the anchor technique. 19,21 Another technical benefit of the aLET is the minimized risk of tunnel interference when performing a concomitant ACLR. Such tunnel conflicts have been reported in a substantial number of cadaveric studies. 14 These tunnel conflicts can be avoided by drilling the LET tunnel under direct visualization of the femoral ACL tunnel or in strict accordance with certain knee flexion when placing the femoral ACL and LET tunnel. 16 However, the introduced anchor technique avoids this issue, as described recently, 10 especially when using a self-tapping anchor. A similar technique was reported before using a tenodesis screw. 27 As illustrated in Figure 2, the close proximity of the femoral ACL tunnel exit and ideal LET fixation point favors a small anchor without the need of predrilling, which was recently confirmed in a biomechanical study. 41 Nevertheless, we recommend placing the anchor before pulling in the ACL graft to minimize any interference with the femoral ACL fixation implant. Whether metal or soft tissue anchors are favorable in this regard remains a debate. Soft tissue anchors ease any revision operation, but their insertion points may be difficult to access on conventional radiographs.
Additionally, physis injury can be minimized in skeletally immature patients since the LET fixation point is located distal to the distal femoral physis and transosseous drilling would require a transphyseal tunnel. 30,31 There is limited evidence about the supplemental LET procedure in skeletally immature patients, but ACL revision rates are highest in adolescents, who may need additional ACL protection procedures. 39 Also, with a transphyseal drilling technique, physis injury can be minimized by using a considerably vertical tunnel orientation, although this demands additional rotatory stability by a peripheral reconstruction technique. 15
In addition, in a recent study of the transosseous fixation technique, up to 17% of persistent tenderness was reported at the area of LET fixation. 6 In our study, there was no critical VAS score in either the aLET group or tLET group, which may be due to the fact that we used low fixation forces in both groups. In this regard, we hypothesized that the anatomic course of the ITB graft might be a factor influencing the local tenderness at the LET fixation area. Biomechanical studies advocate passage under the LCL, since this changes the force vector of the graft, making it more potent in controlling internal rotation. 13 Inderhaug et al 12 demonstrated that with this technique, the flexion angle of LET fixation can vary between 0° and 60°. In this study, we detected a very low pain level at the area of LET fixation regardless of the fixation type as well as the course of the ITB strand. In 2021, Neri et al 24 examined potential overtightening of rotational laxity by LET with the ITB over versus under the LCL, which they did not detect with anterolateral ligament reconstruction and a modified Ellison procedure.
Limitations
This study has some relevant limitations. There was no randomization conducted, which was due to the retrospective design. Neither the passage of the ITB over or under the LCL nor the choice of LET fixation was randomized. In addition, the anchor group was inconsistent with respect to the passage of the graft over or under the LCL, but no significant differences were detected in the subgroup analyses. Still, subgroup analysis was based on a relatively small number of patients. In addition, 12-month results must be considered as early results and longer follow-up studies are necessary. With respect to biomechanics, we cannot make a statement about the superiority of either technique used for LET fixation in our study since no objective rotational measurements were conducted.
Conclusion
This study provides clinical evidence that anchor fixation of the ITB graft prepared in a modified Lemaire technique offers a considerable alternative to tLET fixation in revision ACLR.
Footnotes
Final revision submitted January 15, 2023; accepted January 30, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: This research project was funded by the German Knee Society. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Hamburg (2020-10227-BO-ff).