
Abstract
Background:
Hook plates are widely used for repair of acromioclavicular joint (ACJ) dislocations. However, it is unclear whether repair of torn coracoclavicular (CC) ligament is necessary. The purpose of this study was to evaluate the outcomes of the hook plate fixation with direct CC ligament repair for acute ACJ dislocation in comparison with the hook plate fixation without direct CC ligament repair.
Methods:
The study included 120 patients with acute ACJ dislocations who underwent surgery. The patients were divided into 73 patient groups with Arbeitsgemeinschaft für Osteosynthesefragen (AO) hook plate fixation and direct CC ligament repair and 47 patient groups without direct CC ligament repair. For clinical assessments, the American Shoulder and Elbow Surgeons score, constant score, and time for implant removal were recorded. The corcoclavicular distance (CCD) and the CCD ratio were used for the evaluation of reduction. Typical reported complications, such as secondary dislocation, implant failure or loosening, peri-implant fracture, acromion osteolysis, and postoperative ACJ arthrosis, were also analyzed.
Results:
There were no differences in the clinical outcomes between the two groups. There was no difference in the timing of implant removal between the two groups. The last follow-up CCD was not statistically significant between group with direct CC ligament repair and without repair (9.1 ± 3.3 vs. 9.0 ± 2.8, respectively, p > 0.05). The last follow-up CCD ratio showed significant differences between the two groups (12.6 ± 25.5% vs. 26.3 ± 39.7, respectively, p < 0.05). There was no statistically significant difference in the complication rate between the two groups.
Conclusion:
The hook plate fixation with direct CC ligament repair group was better for maintenance of reduction than that of the hook plate fixation without direct CC ligament repair group. Although, there were no differences of clinical outcomes and complications between two groups.
Level of Evidence:
Level III, Retrospective Study.
Introduction
Acromioclavicular joint (ACJ) dislocations are common shoulder injuries that occur after a direct blow injury to the shoulder or an indirect outstretch injury in an abducted arm position. 1,2 The overall incidence of ACJ dislocations is 9.2 per 1000 individuals per year. Among ACJ injuries, Rockwood classification type III injuries remain controversial with respect to surgical treatment. For high-grade injuries, most surgeons prefer surgical treatments that enable high activity levels for young patients and athletes. 3,4
Several previous studies have demonstrated that reduction status was not correlated with the clinical outcome; however, most shoulder scores used for clinical evaluation did not include ACJ-specific functional evaluations, such as those provided by the Taft score or ACJ instability score. 1,5,6 ACJ restoration prevents joint deformities and poor outcomes, including persistent discomfort and secondary ACJ arthritis. 7 Therefore, it is necessary to restore normal anatomy during the maintenance of a dislocated ACJ.
Numerous surgical fixations have been described in the treatment of ACJ injuries. 8 –11 Among the various techniques, Hook plates are reliable and widely used for repair of ACJ dislocations. However, it is unclear whether repair of torn coracoclavicular (CC) ligament is necessary. Some surgeons sutured torn CC ligament 6,12 ; however, the others did not suture CC ligament during hook plate fixation for ACJ injuries. 13,14
This study aimed to evaluate and compare the clinical and radiologic outcomes of hook plate fixation with and without direct repair of the CC ligament for acute ACJ dislocation. We hypothesized that the clinical and radiologic outcomes would not differ between the two groups.
Methods
This study was approved by our institutional research ethics committee, and written informed consent was obtained from the patients. In total, 120 consecutive patients who underwent open reduction and internal fixation with the conventional AO hook locking compression plate (LCP; Synthes, Solothurn, Switzerland) for Rockwood types III–VI ACJ dislocations at our institution from January 2011 to December 2017 were enrolled.
Unstable ACJ dislocations were clinically and radiologically diagnosed. The clinical diagnosis was based on the assessment of pain and tenderness after frank injury. Preoperative radiological examinations included anteroposterior and cephalic tilt views taken with the shoulder fixed in the same position to minimize the impact of inconsistent posture on the interpretation of the radiographs. To confirm the Rockwood type, stress AP view of the shoulder was obtained, with the patient standing and holding 4-kg weights with the arm hanging down. The Rockwood classification was performed after a review of the radiographs.
A retrospective comparative cohort study design was adopted, with the following inclusion criteria: (1) acute and Rockwood type III or V ACJ dislocations, (2) operative treatment using conventional AO hook LCP, (3) a minimum follow-up period of 12 months after surgery, and (4) a history of painless and unrestricted shoulder function prior to trauma. The exclusion criteria were as follows: (1) previous surgical history of the affected shoulder, (2) concomitant fracture around the affected shoulder, (3) open dislocations and fracture dislocation of the ACJ, and (4) neglected and chronic ACJ dislocations (>4 weeks). The first 73 patients underwent hook plate fixation with direct repair of the CC ligament (group A), and the next 47 patients underwent hook plate fixation without direct repair of the CC ligament (group B); the procedures were performed by two shoulder surgeons (JBS and JSY). Data regarding patient characteristics, injury mechanism, time to surgery, and follow-up period were collected.
Surgical procedure of hook plate fixation with direct repair of CC ligament
All surgeries were performed under general anesthesia, with the patient in a supine position and 30° chest elevation. A 5–6-cm saber cut incision was made above the ACJ. The deltoid–trapezoidal fascia was incised in line with the lateral clavicle. After exposure and reduction of the ACJ, a hook plate was placed under the acromion posterior to the ACJ. The reduction status, depth of the hook, and contour of the plate on the distal clavicle were observed under fluoroscopic guidance. The medial part of the plate was pressed downward using reposition forceps, and then the plate was fixed with a 3.5-mm medial cortical screw. After the reduction status, plate contour, and hook depth were rechecked under fluoroscopy, locking screw fixation of both the medial and lateral fragments was performed (Figure 1). For additional CC ligament repair, the attachment of the deltoid muscle was partially detached from the clavicle. After confirmation of the hematoma around the injured and ruptured CC ligament, the hematoma was removed and both ends of the ruptured CC ligament were repaired using Vicryl No. 1 sutures (Figure 1). Subsequently, the deltoid and trapezial fascias were repaired for secure reinforcement over the plate, and the wound was closed in layers (Figure 2).

Intraoperative photographs of a 56-year-old man left shoulder: (a) Total rupture of CC ligament was observed after deltoid partial detachment. (b) Ruptured CC ligament was directly repaired with four Vicryl No. 1 sutures after hook plate fixation. CC: coracoclavicular.

Preoperative and postoperative anteroposterior radiographs of a 44-year-old man who underwent hook plate fixation in the acute ACJ dislocation. ACJ: acromioclavicular joint.
Surgical procedure of hook plate fixation without direct repair of CC ligament
The same position, approach, and reduction were used for patients who underwent hook plate fixation without direct repair of the CC ligament. In this group, the attachment of the deltoid muscle was not detached from the clavicle. The deltoid and trapezial fascias were repaired for secure reinforcement over the plate, and the wound was closed in layers.
Postoperative rehabilitation and implant removal
The affected arm was kept in a sling for 6 weeks after surgery. Pendulum, self-assisted circumduction, and gradual passive range-of-motion (ROM) exercises were started 3 days after surgery, as tolerable. Active ROM exercises were started 6 weeks after surgery. The implant was removed after 3–5 months. If the patient experienced shoulder stiffness at the time of implant removal, brisement or arthroscopic capsulectomy under general anesthesia was concomitantly performed before implant removal. During implant removal, the authors prefer to only expose the superior tissue of the plate without further soft tissue dissection to avoid iatrogenic injury of the healed ligament. Strength exercises were initiated after implant removal.
Clinical and radiologic evaluations
All patients were evaluated for a minimum period of 1 year. For clinical assessments, the American Shoulder and Elbow Surgeons (ASES) score and Korean shoulder score (KSS) were recorded by the physician’s assistant at the final follow-up. An independent examiner who was blinded to patient data evaluated all values at each postoperative follow-up appointment.
For radiological evaluation, anteroposterior views of both clavicles were taken regularly after surgery (at 3, 6, and 12 weeks; 6 months; and 1 year). ACJ dislocation grade was determined via a bilateral weight-bearing panoramic view for comparison with the uninjured side. Standing anteroposterior radiographs with patients holding a 4-kg weight in each hand (stress view of both shoulders) were taken. The degree of ACJ displacement (CC distance (CCD) ratio) was measured using the CCD and compared with that of the contralateral shoulder on standard radiographs. The CCD was measured between the uppermost border of the coracoid process and the lateral aspect of the conoid tubercle (Figure 3).

CCD was measured between the uppermost border of the coracoid process and the lateral aspect of the conoid tubercle. CCD ratio was measured using the CCD and compared with that of the contralateral shoulder on standard radiographs. CCD: coracoclavicular distance.
All radiologic measurements were analyzed by two independent examiners (SJK and HJH). The individual value was measured, and then the individual mean value was calculated. All radiographs were evaluated for the time periods required for fracture consolidation and adverse events including typical reported complications of both procedures such as secondary dislocation, implant failure and loosening, peri-implant fracture, acromion osteolysis, and postoperative ACJ arthrosis (Figure 4).

Complications following hook plate fixation. (a) ACJ arthrosis. (b) Acromion osteolysis (arrow). ACJ: acromioclavicular joint.
Statistical analyses
To determine the normal distribution of the continuous data, the Kolmogorov–Smirnov test was performed. Continuous variables were analyzed using an independent t-test, and noncontinuous variables were analyzed using Pearson’s χ 2 test. All statistical analyses were performed using the Statistical Package for Social Sciences version 25.0 (SPSS, Inc., IBM Co., Chicago, Illinois, USA). Statistical significance was considered at p < 0.05 for all analyses.
Results
Demographic data
The study included 17 women and 103 men (age range, 19–72 years). The initial injuries were caused by traffic accidents in 11 patients, falls in 68 patients, and sport-related injuries in 41 patients. No significant differences were found in the demographic data, time to surgery, and mean follow-up period between the two surgical groups (Table 1).
Demographic data.
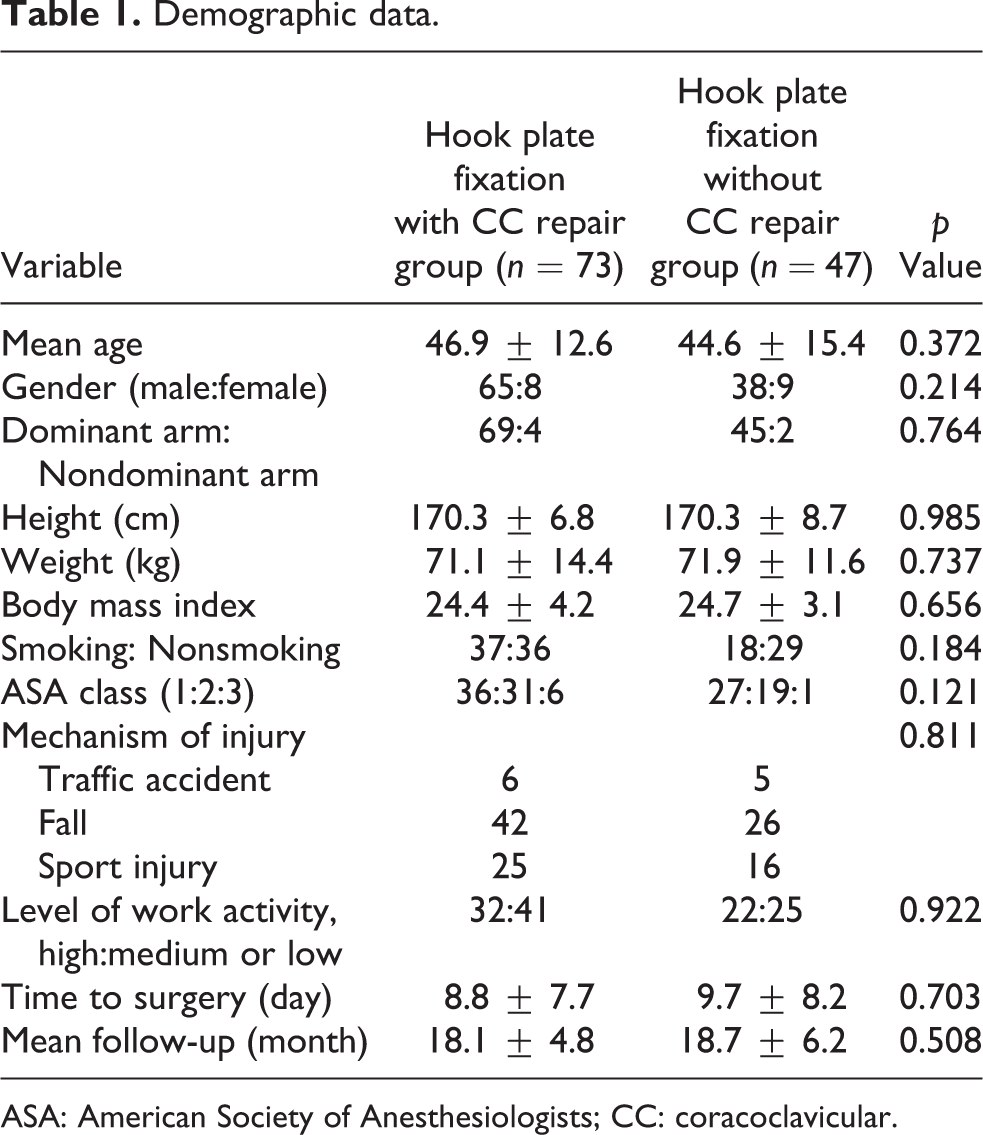
ASA: American Society of Anesthesiologists; CC: coracoclavicular.
Clinical outcomes
There were no differences in the ASES score, KSS, and constant score between the groups. The mean ASES scores were 89.2 ± 12.6 and 87.9 ± 11.2 in group A and group B, respectively. The mean constant scores were 83.9 ± 9.8 and 84.0 ± 10.6 in groups A and B, respectively (Table 2).
Clinical and radiologic outcomes between the two groups.

ASES: American Shoulder and Elbow Surgeons; CCD: coracoclavicular distance; CC: coracoclavicular.
Radiologic outcomes
There were no differences in the Rockwood classification between the two groups, and there were also no differences in the CCD of the uninjured side between the two groups; the mean CCDs of the uninjured side were 8.0 ± 2.1 mm and 7.3 ± 1.8 mm in groups A and B, respectively. There were no differences in the preoperative CCD of the injured side between the two groups; the mean preoperative CCDs of the injured side were 15.5 ± 4.6 mm and 14.4 ± 5.7 mm in groups A and B, respectively. There were no differences in the CCD of the injured side at the last follow-up between the two groups; the mean CCDs of the injured side at the last follow-up were 9.1 ± 3.3 mm and 9.0 ± 2.8 mm in groups A and B, respectively. There were no significant differences in the preoperative CCD ratios between the groups; the mean preoperative CCD ratios were 198.5 ± 54.3 and 201.3 ± 78.3 in groups A and B, respectively. However, there were significant differences in the CCD ratios at the last follow-up between the two treatment groups; the means of the CCD ratios at the last follow-up were 112.6 ± 25.5 and 126.3 ± 39.7 in groups A and B, respectively (p = 0.039, Table 2).
Complications
There was no difference in the complication rates between the two treatment groups; overall, 48 (65.7%) and 33 (63.8%) complications were observed in groups A and B, respectively. Postoperative stiffness was reported in 25 (34.2%) and 16 (34.0%) patients in groups A and B, respectively, although pendulum and self-assisted circumduction exercises were started 3 days after surgery. Brisement or arthroscopic capsulectomy was performed in patients with postoperative stiffness during implant removal. After implant removal, all patients recovered full ROM at the final follow-up.
There were no significant differences that could influence the clinical outcomes in the prevalence of subacromial erosion and post-traumatic ACJ arthrosis between the groups. Subacromial erosion was observed in 32 (43.8%) and 19 (40.4%) patients in groups A and B, respectively. Post-traumatic ACJ arthrosis was observed in 16 (21.9%) and 12 (25.5%) patients in groups A and B, respectively. No cases of infection, secondary dislocation, implant failure, loosening, or peri-hardware fractures were observed in either of the groups (Table 3).
Complications between the two groups.

ACJ: acromioclavicular joint; CC: coracoclavicular.
Discussion
This study aimed to compare the clinical and radiologic outcomes of hook plate fixation with and without direct repair of the CC ligament for acute ACJ dislocation. According to our hypothesis, there were no differences in clinical outcomes and complications between the groups. However, contrary to our initial hypothesis, compared with group B, group A showed a better CCD ratio at the last follow-up.
Although various surgical procedures have been reported for the treatment of ACJ dislocation, no optimal surgical solution has been agreed upon. 15 –18 Among the various fixation methods, hook plate fixation is a popular procedure for ACJ injuries. However, loss of reduction of CCD is a concern associated with implant removal after hook plate fixation for ACJ dislocation. Jensen et al. 13 described that 68% of patients who underwent hook plate fixation showed more than 2-mm loss of reduction of CCD. Stein et al. 6 also reported that the mean CCD ratio of 27 patients at 24 months after hook plate fixation for ACJ dislocation was 141.8%. Several studies have reported satisfactory clinical outcomes despite the loss of reduction of CCD. 6,12 –14 However, they used shoulder scores for clinical evaluation without analyzing the ACJ-specific functional evaluations (Taft score or ACJ instability score).
Whether direct repair of the CC ligament is better for maintenance of reduction is unclear. However, this method may help restore the length of the CC ligament. However, loss of reduction is inevitable, although the torn CC ligament can be repaired with hook plate fixation. 6 Direct repair of torn CC ligament could lead to biological damage with additional soft tissue violation. Further, iatrogenic injury of the anterior deltoid fiber could occur while approaching the CC ligament, because the anterior part of the deltoid muscle is widely spread over the clavicle and over the anterior surface and the anterior third of the lateral acromion. 19 The main purpose of hook plate fixation for acute displaced ACJ dislocation is to maintain the indirect reduction of ACJ until the CC ligaments heal and to prevent scarring of the CC interspace while permitting some rotatory motion between the clavicle and acromion. 16,20,21 However, loss of reduction is also inevitable after hook plate fixation without direct repair of the CC ligament for ACJ injuries. 14 To the best of our knowledge, no study has compared hook plate fixation with and without direct repair of the CC ligament. Contrary to our initial hypothesis, the CCD ratios at the last follow-up were better in group A than in group B in the present study. It is considered that direct repair of the torn CC ligament is better for the restoration of the length of CC ligament than indirect healing of CC ligament with ACJ reduction.
A high rate of hook-related complications has been reported in previous studies. 22 –25 In 2018, Yin et al. reported that 16 of 26 patients (61.5%) treated with hook plate osteosynthesis experienced complications. In a systematic review, 66 of 162 patients (40.7%) treated with hook plate fixation experienced complications. 26 The present study showed a higher complication rate in both groups (65.7% vs. 63.8%) compared with that reported in previous studies; however, there was no statistically significant difference. We believe that the higher complication rate in this study was due to the different methods used to define complications.
This study has several limitations. First, this was a nonrandomized retrospective study. Second, the sample size differed between the two groups. The authors changed the technique from hook plate fixation with direct repair of the CC ligament to hook plate fixation without direct repair of the CC ligament to avoid iatrogenic anterior deltoid detachment from the clavicle. This decision was made iatrogenic anterior deltoid detachment that can induce postoperative anterior deltoid atrophy. Third, the groups were divided according to whether they underwent direct repair of the CC ligament, and two different surgeons operated on the groups. Fourth, only the ASES and constant scores were analyzed without ACJ-specific functional evaluations (Taft score or ACJ instability score) in this study. Finally, postoperative anterior deltoid muscle volume was not evaluated and compared between the groups.
Conclusion
Although no differences in clinical outcomes and complications were observed between the two groups in this study, hook plate fixation with direct repair of the CC ligament was better than hook plate fixation without direct repair of the CC ligament for maintenance of reduction.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This article does not contain any studies with human participants or animals performed by any of the authors.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.