
Abstract
Background:
The extent to which concomitant cartilage repair provides an improvement in clinical outcomes after osteotomy is unclear.
Purpose:
To compare studies reporting clinical outcomes after isolated osteotomy with or without cartilage repair for osteoarthritis (OA) or focal chondral defects (FCDs) of the knee joint.
Study Design:
Systematic review; Level of evidence, 4.
Methods:
A systematic review was conducted according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines by searching PubMed, Cochrane Library, and Embase databases. The search was done to identify comparative studies that directly compared outcomes between isolated osteotomy—high tibial osteotomy or distal femoral osteotomy—and osteotomy with concomitant cartilage repair for OA or FCDs of the knee joint. Patients were evaluated based on reoperation rate, magnetic resonance observation of cartilage repair tissue score, macroscopic International Cartilage Regeneration & Joint Preservation Society score, and patient-reported outcomes.
Results:
In total, 6 studies—level 2 evidence (n = 2);, level 3 evidence (n = 3);, and level 4 evidence (n = 1)—met the inclusion criteria, including a total of 228 patients undergoing osteotomy alone (group A) and 255 patients undergoing osteotomy with concomitant cartilage repair (group B). The mean patient age was 53.4 and 54.8 years, respectively, and the mean preoperative alignment was 6.6° and 6.7° of varus in groups A and B, respectively. The mean follow-up time was 71.5 months. All studies assessed medial compartment lesions with varus deformity. One study compared osteotomy alone for patients with medial compartment OA versus osteotomy with autologous chondrocyte implantation for patients with FCDs of the medial compartment. Three other studies included a heterogeneous cohort of patients with OA and FCDs in both groups. Only 1 study isolated its comparison to patients with medial compartment OA and 1 study isolated its comparison to patients with FCDs.
Conclusion:
There is limited evidence with substantial heterogeneity between studies on clinical outcomes after osteotomy alone versus osteotomy with cartilage repair for OA or FCDs of the knee joint. At this time, no conclusion can be made regarding the role of additional cartilage procedures in treating medial compartment OA or FCDs. Further studies are needed that isolate specific disease pathology and specific cartilage procedures.
The management of chondral defects of the knee joint continues to raise discussion, as currently no consensus for a standard treatment algorithm exists. 36 Progressive cartilage degeneration of the knee joint leading to osteoarthritis (OA) has been attributed to malalignment because of proximal laxity of the collateral ligaments, deviation of the functional axis of the knee, and tibial and femoral bone deformities due to cartilage loss on the deficient side. 16,27 Although total knee arthroplasty (TKA) provides excellent outcomes in the older population, patients aged <55 years have a risk of revision as high as 35% and a high percentage of dissatisfaction. 3 Because of its activity limitations and complication rates, TKA is less than ideal in younger patients, and investigations into biological joint restoration procedures have been pursued. 36 Realignment osteotomy can serve as an alternative to TKA in active, younger patients with unicompartmental OA by offloading the medial or lateral compartment. 2,18 Furthermore, osteotomies can be used as an adjunct to the treatment of focal chondral defects (FCDs) by reducing contact pressure on the implanted graft, normalizing mechanics, and significantly unloading the affected compartment of the knee leading to improved clinical outcomes and superior graft survivorship. 8
Although realignment osteotomy can improve pain relief and joint function by offloading one of the compartments, osteotomies are not able to restore the integrity or function of the meniscus or articular cartilage. 31 Despite good results at the short- to midterm follow-ups, 1,29 long-term results have shown a clinical deterioration over time. 33,35 This has led to several authors suggesting the use of concomitant cartilage repair procedures—such as autologous chondrocyte implantation (ACI), microfracture (MFx), osteochondral autograft transplantation, and osteochondral allograft transplantation—to improve long-term outcomes. 32,35 Cartilage restoration procedures can help combat this limitation by improving symptoms and preventing degenerative changes by achieving restoration of the articular cartilage. 30
This study aimed to perform a systematic review to compare clinical outcomes of patients undergoing isolated osteotomy with or without cartilage repair for OA or FCDs of the knee joint. Because of the limited literature on this topic, we hoped to gain further insight into the comparative efficacy of osteotomy versus concomitant osteotomy and cartilage repair for chondral lesions of the knee joint. We hypothesized that patients undergoing combined cartilage repair and realignment would have superior clinical outcomes for treating FCDs while no differences in outcomes would be identified in patients with unicompartmental OA.
Methods
This systematic review was conducted according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) guidelines using a PRISMA checklist. Two independent reviewers (J.D., S.M.F.) searched PubMed, Embase, and Cochrane Library databases up to August 17, 2022. The electronic search strategy used was as follows: osteotomy AND knee AND (“autologous chondrocyte” OR “osteochondral autograft” OR “osteochondral allograft” OR microfracture). Included were clinical studies that compared isolated osteotomy— high tibial osteotomy (HTO) or distal femoral osteotomy (group A)—versus osteotomy with concomitant cartilage repair for the treatment of OA or FCDs of the knee joint (group B). Studies were excluded if they were nonhuman, did not involve a knee joint, had additional procedures, or had a patellofemoral chondral pathology focus or if there was no English full-text publication available. A total of 603 studies were reviewed by title and/or abstract to determine study eligibility based on the inclusion criteria. In cases of disagreement, a third reviewer (M.J.K.) made the final decision. Six studies 4,9,17,20,23,27 met the inclusion criteria and were included in the systematic review (Figure 1).

A PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analyses) flow diagram of study inclusion.
Data extraction from each included study was performed independently and then reviewed by the second author (M.J.K.). There was no need for funding or a third party to obtain any of the collected data.
Reporting Outcomes
Outcomes assessed included patient-reported outcomes (PROs), including the subjective International Knee Documentation Committee (IKDC) score, 14 the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), 28 Knee Society Knee Score (KSKS) and Function Score (KSFS), 7 Japanese Orthopaedic Association knee score, 25 Hospital for Special Surgery knee assessment, 13 Lysholm score, 21 visual analog scale for pain, and satisfaction. Patient satisfaction was measured by 1 study 27 according to a satisfaction scale (range, 1-10).
Other outcomes assessed included reoperation rate, complication rate, and macroscopic International Cartilage Regeneration & Joint Preservation Society (ICRS) score. One study 20 assessed postoperative arthritic changes using the MOCART (magnetic resonance observation of cartilage repair tissue) score. 22 The MOCART score, ranging from 0 (worst possible) to 100 (normal), allows for the analysis of 3 clinical variables as follows: (1) the radiological outcome of cartilage repair technique several months to years after surgery; (2) the statistical description of the interobserver variability; and (3) the statistical correlation of the subjective clinical outcome with the radiological variables of the magnetic resonance imaging scoring system.
Study Methodology Assessment
The modified Coleman Methodology Score (MCMS) 6 was used to evaluate the study methodology quality. The MCMS has a scaled potential score ranging from 0 to 100 (excellent, 85-100; good, 70-84; fair, 55-69; poor, <55). The primary outcomes assessed by the MCMS are study size and type, follow-up time, attrition rates, number of interventions per group, and proper description of study methodology.
The risk of bias was assessed according to the Cochrane risk-of-bias tool 11 for 1 randomized study, 27 which incorporates an assessment of randomization, blinding, completeness of outcome data, selection of outcomes reported, and other sources of bias. For the remaining 5 nonrandomized studies, 4,9,17,20,23 bias was assessed according to the Risk Of Bias In Non-randomised Studies–of Interventions (ROBINS-I) risk-of-bias tool, 34 which incorporates an assessment of bias due to confounding, selection of participants, deviations from intended interventions, completeness of outcomes data, selection of outcomes reported, and other sources of bias. The Cohen kappa (κ) was calculated to determine the level of agreement between reviewers. A κ value of <0.20 indicates poor agreement; 0.21 to 0.40, fair agreement; 0.41 to 0.60, moderate agreement; 0.61 to 0.80, good agreement; and 0.81 to 1, very good agreement. 24
Statistical Analysis
The weighted mean was calculated for numerical demographic characteristics (age, follow-up, sex proportion, body mass index, and lesion size).
Results
The 6 included studies had evidence levels of 2 to 4 (2 level 2 studies, 3 level 3 studies, and 1 level 4 study). A total of 483 patients were included across all studies, including 228 patients undergoing osteotomy alone (group A) and 255 patients undergoing osteotomy with concomitant cartilage repair (group B). The mean patient age was 53.4 and 54.8 years in groups A and B, respectively, and the mean lesion size was 4.8 and 5.2 cm2 in groups A and B, respectively. The mean follow-up time was 71.5 months. The mean body mass index was 26.8 and the overall percentage of men was 45.5% (Table 1).
Studies Included in the Review a

a Age, follow-up, and BMI data (if available) are reported as mean or mean ± SD. BMI, body mass index; LOE, level of evidence; NR, not reported. Dash indicates not applicable.
b n refers to the number of knees that underwent operation with either osteotomy alone (group A; n = 228) or osteotomy with concomitant cartilage repair (group B; n = 255).
c Reported as weighted mean.
The only osteotomy used was HTO. Five studies 4,9,17,20,27 used an opening-wedge HTO and 1 study 23 used a closing-wedge HTO. The cartilage procedures used were marrow-stimulating procedures (MFx, abrasion arthroplasty, and subchondral drilling) (n = 202; 79%) and regenerative procedures (ACI) (n = 53; 21%) (Table 2). The mean preoperative 6.6° and 6.7° of varus in groups A and B, respectively. Only 1 study 4 reported postoperative alignment (group A, 2.8° ± 1.8° of valgus; group B, 2.6° ± 1.7° of valgus). All studies assessed medial compartment lesions with varus deformity. A total of 204 patients with OA and 96 patients with FCDs underwent treatment.
Cartilage Lesion Characteristics a

a Defect size and preoperative alignment are reported as mean ± SD. Treated Lesion Loc and Type of Cart Repair refer to number of knees treated.. A, group A (osteotomy alone); AA, abrasion arthroplasty; ACI, autologous chondrocyte implantation; B, group B (osteotomy with cartilage repair); FCDs, focal chondral defect; MFC, medial femoral condyle; MFx, microfracture; Mixed, study included patients with OA or FCDs; NR, not reported; OA, osteoarthritis; SD, subchondral drilling.
b All angles are varus.
c Reported as weighted mean.
Patient-Reported Outcomes
In 1 study, 4 patients undergoing isolated HTO for OA or HTO with ACI for medial compartment FCDs had a significant decrease in the visual analog scale for pain level and a significant increase in Lysholm scores from pre- to postoperatively (P < .001). However, PROs were not compared between the 2 groups, as they represented different medial compartment pathologies (medial compartment OA versus FCDs).
In the study by Ferruzzi et al, 9 isolated HTO and HTO with ACI showed significantly better outcomes in terms of Hospital for Special Surgery and WOMAC scores compared with HTO with MFx at the final follow-up (P < .05). This study included a heterogeneous collection of patients with OA or FCDs in groups A and B.
Patient-Reported Outcome Scores a
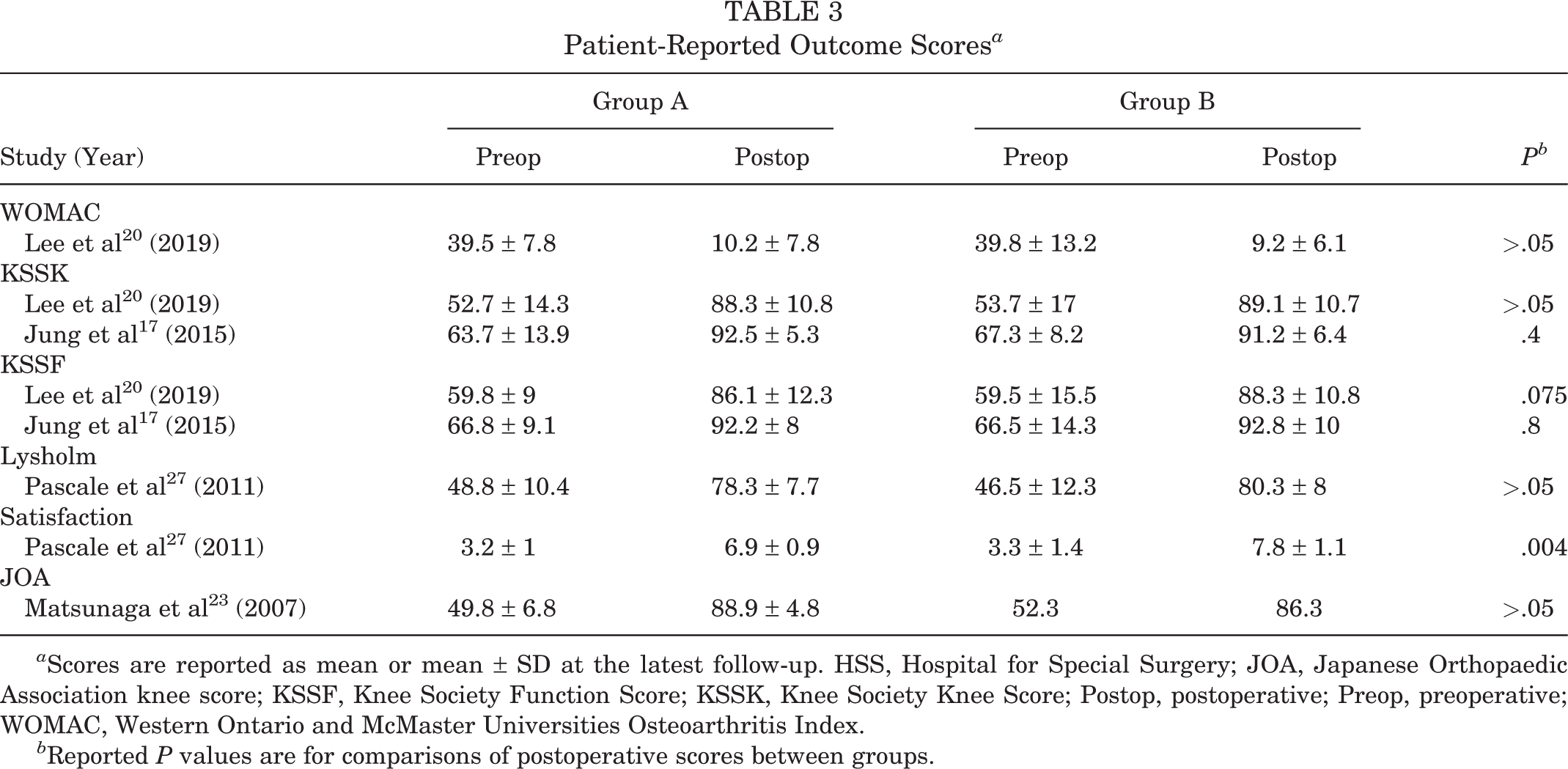
a Scores are reported as mean or mean ± SD at the latest follow-up. HSS, Hospital for Special Surgery; JOA, Japanese Orthopaedic Association knee score; KSSF, Knee Society Function Score; KSSK, Knee Society Knee Score; Postop, postoperative; Preop, preoperative; WOMAC, Western Ontario and McMaster Universities Osteoarthritis Index.
b Reported P values are for comparisons of postoperative scores between groups.
Lee et al 20 reported results for the WOMAC, Knee Society Knee Score, and the Knee Society Function Score and found no significant differences between groups at the final follow-up (P > .05). Pascale et al 27 reported results for the Lysholm score and found no significant differences between groups at the final follow-up (P = .42). The same study 27 reported satisfaction and found a significantly higher satisfaction in group B compared with group A at the final follow-up (P = .004). Matsunaga et al 23 reported results for the Japanese Orthopaedic Association score and found no significant differences between groups at the final follow-up (P > .05). Jung et al 17 reported results for the Knee Society Knee Score and function score and found no significant differences between groups at the final follow-up (P = .4 and P = .8, respectively).
Other Reported Outcomes
Macroscopic ICRS Score
Two studies 17,20 reported results for the macroscopic ICRS score and found no significant differences between groups (P > .05 17 and P > .43 20 ).
MOCART Score
One study, 20 which included a heterogeneous collection of patients with OA/FCDs in both groups and used MFx to treat chondral lesions, reported results of the MOCART score and found a significant difference in the defect filling and integration to the border zone of the medial femoral condyle, favoring group B (P < .001).
Reoperation Rate
Three studies 4,9,27 assessed the reoperation rate at the final follow-up (Table 4). Two studies 4,27 indicated reoperation as the need to convert to TKA, while the third study 9 did not define reoperation.
Reoperation Rate a
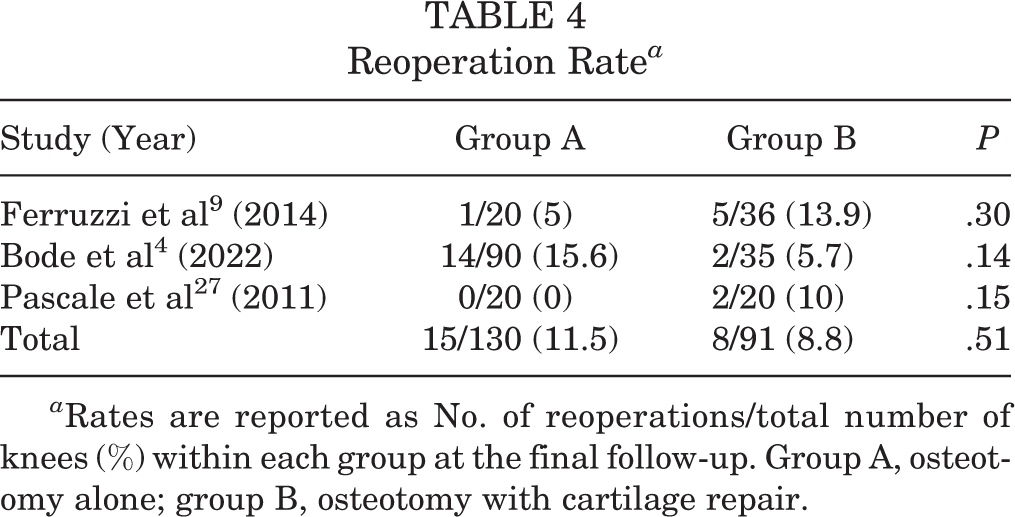
a Rates are reported as No. of reoperations/total number of knees (%) within each group at the final follow-up. Group A, osteotomy alone; group B, osteotomy with cartilage repair.
Study Methodology Assessment
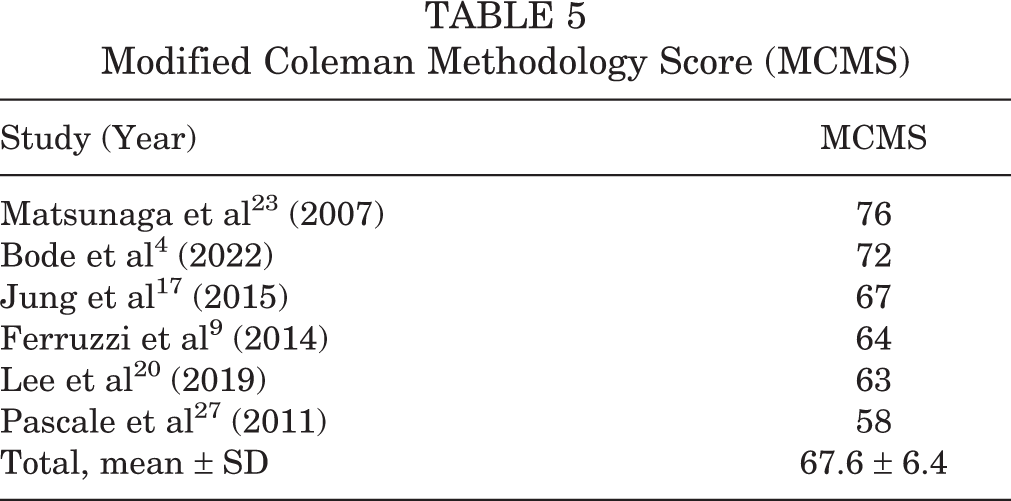
Modified Coleman Methodology Score
Table 5 shows the MCMS scores from the 6 included studies. Two studies 4,23 received a good score. The remaining 4 studies 9,17,20,27 received a fair score.
Modified Coleman Methodology Score (MCMS)
Risk of Bias
The results of the methodologic quality assessment of the 5 nonrandomized studies using the ROBINS-I risk of bias tool are presented in Figure 2. All 5 nonrandomized studies 4,9,17,20,23 showed a moderate risk of bias due to confounding, as no prognostic variables predicted baseline intervention and no patients switched between interventions during the study period. No studies excluded eligible patients or used variable follow-up times based on intervention (low risk of bias), no studies deviated from the intended intervention (low risk of bias), and all studies classified treatment type (low risk of bias). One study 20 using blinded outcome assessors showed no systematic differences in the care provided between treatment groups (low risk of bias), while 4 studies 4,9,17,23 used nonblinded but identical postoperative protocols (moderate risk of bias). No studies showed bias due to missing data (low risk of bias). One study 20 demonstrated a low risk of bias in the measurement of outcomes through the use of blinded outcome assessors, while 5 studies 4,9,17,20,23 used physicians not blinded to the treatment group because of the nature of the treatment (serious risk of bias). Finally, no studies showed bias due to selective reporting (low risk of bias). A Cohen κ value of 0.86 reflected a very good agreement between reviewers.
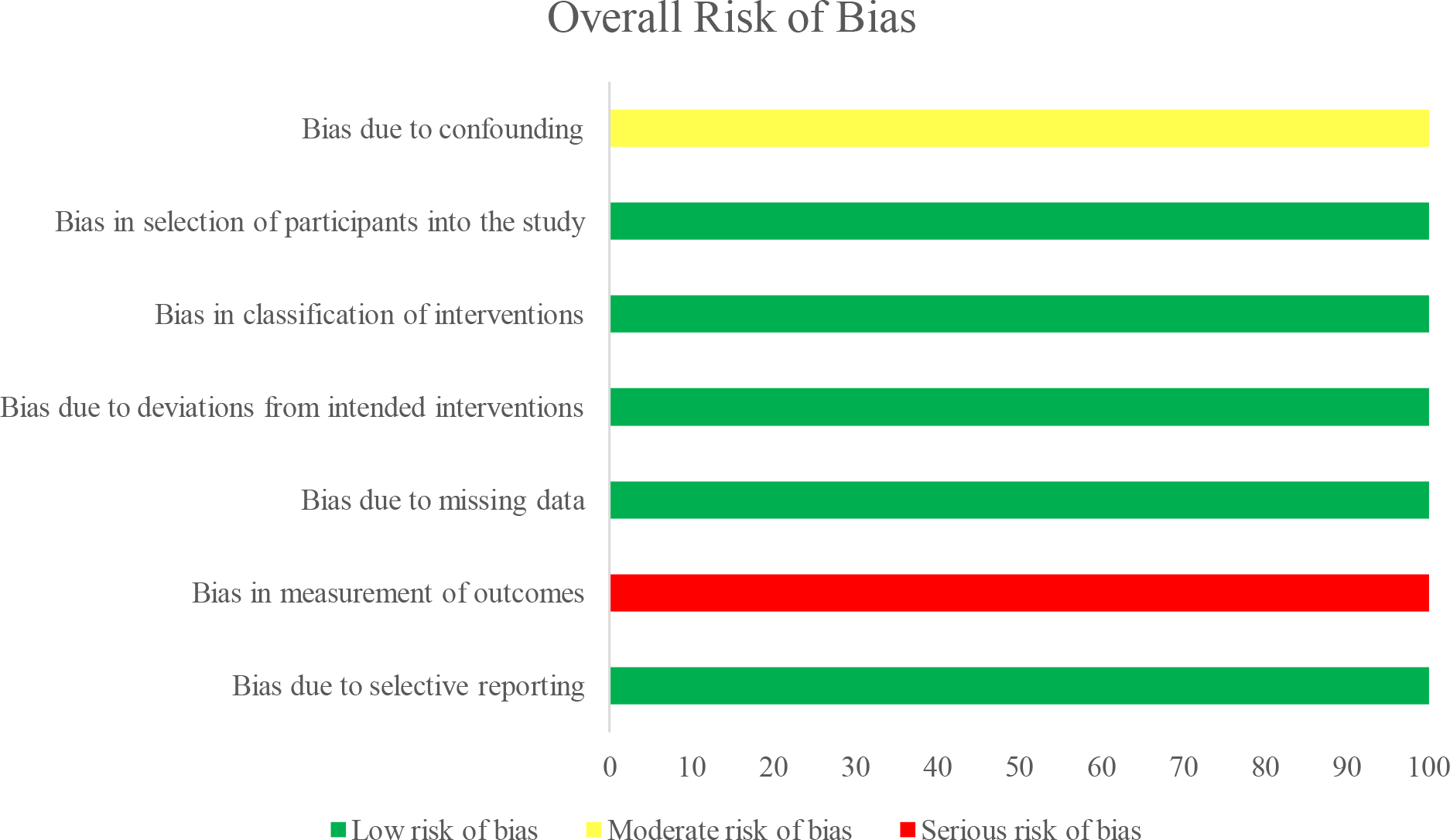
Risk of bias of the nonrandomized studies (n = 5).
The remaining, randomized, study 27 was assessed for methodologic quality using the Cochrane risk-of-bias tool. While sequence generation and allocation were not adequately reported (high risk of bias), there was a low risk for detection bias because of the blinding of the outcome assessor. Patients were blinded to their intervention group (low risk of bias). There was no significant loss to follow-up (low risk of bias) and no selective reporting or incomplete outcome data (low risk of bias).
Discussion
Based on the results of our systematic review, we found substantial heterogeneity between studies on clinical outcomes after osteotomy alone versus osteotomy with cartilage repair for OA or FCDs of the knee joint. One study 4 compared osteotomy alone for patients with medial compartment OA versus osteotomy with ACI for patients with FCDs of the medial compartment, thereby comparing outcomes between 2 heterogeneous cohorts. Three other studies 9,20,27 included a heterogeneous cohort of patients with OA and FCDs in both groups. Only 1 study 23 isolated their comparison to patients with medial compartment OA, and 1 study 17 isolated comparison to patients with FCDs. Due to heterogeneity between and within studies, it is not possible to make any strong conclusions at this time regarding isolated osteotomy versus osteotomy with cartilage repair.
Knee OA most commonly affects the medial compartment, which can lead to the gradual development of varus malalignment and a subsequent shift of the weightbearing line to pass more medially through the tibial plateau. 26 Regardless of OA or FCDs, osteotomy effectively offloads the medial or lateral compartment of the knee joint and therefore can improve symptoms in either case. Previous studies 1,33 have illustrated that correction to valgus alignment is necessary to avoid a postoperative return to varus alignment and a subsequent failure. A study by Ishizuka et al 15 demonstrated that in patients with severe medial compartment OA, HTO effectively offloads the compartment with high survivorship at 10 years. Malalignment leads to increased tibiofemoral contact and cartilage wear within the loaded compartment, worsening the degree of deformity. 19 Biomechanical studies have shown that deviation of even 3° can produce significantly elevated peak stresses in the loaded compartment and that HTO offloads the affected compartment and increases contact pressure in the opposite compartment in proportion to the degree of correction. 19
A recent systematic review 8 compared clinical outcomes of patients undergoing isolated cartilage repair of the knee joint versus cartilage repair with concomitant osteotomy. The study included 1747 patients and found significant improvements in multiple clinical outcomes favoring the combined treatment group, with no significant differences between groups with regard to procedure costs and complication rates. Similar to our systematic review, Filardo et al 10 performed a systematic review of combined cartilage treatment and osteotomy for knee OA and found mostly low-quality studies with insufficient evidence to recommend this treatment approach in patients with knee OA. Another systematic review 18 published in 2017 that looked solely at HTO combined with cartilage restoration found reliable outcomes in terms of pain relief and functional scores for patients with OA at the mid- to long-term follow-ups and had the potential to delay or avoid the need for knee arthroplasty surgery. However, this previous systematic review did not compare outcomes with another treatment group; based on our review, there is currently insufficient evidence for recommending cartilage repair in patients with unicompartmental OA undergoing osteotomy because of a lack of comparative studies. Furthermore, while 4 studies 4,9,20,27 included patients with OA and FCD, only 1 study 4 distinguished results between patients with OA and FCDs. Therefore, further mid- and long-term outcome studies are needed to determine the effects of isolated osteotomy versus combined treatment in patients with FCDs or OA while making sure to distinguish results between the 2 pathologies. Regarding future studies, we recommend studies using the IKDC subjective knee form and the Knee injury and Osteoarthritis Outcome Score, both of which are endorsed by the ICRS, as they represent 2 PRO measures that fulfill the basic requirements for reliability, validity, and responsiveness in patients undergoing cartilage repair. 5
Limitations
A limitation of this study was that only 6 studies were included and 4 studies were considered a low level of evidence (level 3 or 4). There was heterogeneity in the type of cartilage restoration procedures performed and the reported PROs between studies. Another limitation to be noted is that some studies included patients with OA or FCDs, while 3 studies 9,20,27 did not distinguish results between the 2. It is important to distinguish between OA or FCDs, as FCDs are isolated injuries that can range from small partial-thickness to large full-thickness lesions. Although knee OA is associated with progressive loss of articular cartilage, OA is a pathological process that differs from FCDs. 12 Most of the cartilage restoration procedures used in the included studies were either MFx or ACI, and thus these results cannot be applied to other cartilage procedures. Finally, all patients in this review had varus deformity with medial compartment cartilage lesions, and therefore our results do not necessarily reflect the results of cartilage repair with distal femoral osteotomy for lateral compartment pathology.
Conclusion
There was limited evidence and substantial heterogeneity between studies in this review of clinical outcomes after osteotomy alone versus osteotomy with cartilage repair for OA or FCDs of the knee joint. No conclusion can be made at this time regarding the role of additional cartilage procedures in treating medial compartment OA or FCDs. Further studies are needed to isolate specific disease pathology and specific cartilage procedures.
Footnotes
Final revision submitted December 5, 2022; accepted January 19, 2023.
One or more of the authors has declared the following potential conflict of interest or source of funding: A.J.S. has received consulting fees from DePuy Synthes Products and Medical Device Business Services; hospitality payments from Globus Medical; and hospitality payments from DePuy Synthes Sales. P.C.M. has received compensation for services other than consulting from Arthrex; consulting fees from Arthrex and Vericel; education payments from Medinc of Texas and Smith & Nephew; hospitality payments from Medinc of Texas; consulting fees from Smith & Nephew; and honoraria from Vericel Corp.