
Abstract
Background:
Lateral meniscal deficiency with valgus malalignment increases the rate of lateral compartment osteoarthritis. Lateral meniscal allograft transplantation (LMAT) with a concomitant varus-producing opening-wedge distal femoral osteotomy (DFO) is an option yet to be evaluated biomechanically.
Purpose/Hypothesis:
The purpose of this study was to clarify the biomechanical effects of the realignment procedure in the setting of LMAT. We hypothesized that (1) given the dependence of the lateral compartment on the lateral meniscus, a DFO and increasing degrees of varus would be insufficient to restore lateral compartment pressures to normal from a lateral meniscus-deficient state, and that (2) LMAT would restore lateral compartment pressures to the intact state while DFO would decrease lateral compartment pressures for any given state of the meniscus.
Study Design:
Controlled laboratory study.
Methods:
Ten cadaveric knees underwent opening-wedge varus-producing DFO secured by an external fixator. Anatomic alignment was standardized to 6° of mechanical valgus, and each joint was tested in full extension. Submeniscal placement of thin film pressure sensors allowed for the recording of contact pressure, peak contact pressure, and contact area. The specimens were loaded on a biaxial dynamic testing machine with loading angles between 9° valgus and 6° varus of mechanical alignment. Conditions tested included intact meniscus, meniscal deficiency, and meniscal transplantation.
Results:
Isolated varus-producing DFO to 6° in the meniscus-deficient state failed to restore joint pressures and contact areas to the intact state, with significant changes in mean contact pressure (175%), mean peak contact pressure (135%), and contact area (–41%) (all P < .05 vs intact), while LMAT restored all outcome measures (all P > .05 compared with intact). After LMAT, every additional 1° of DFO correction contributed to a decrease in the mean contact pressure, peak pressure, and contact area of 5.6% (–0.0479 N/mm2), 5.9% (–0.154 N/mm2), and 1.4% (–6.99 mm2) for the lateral compartment and 7.3% (+0.034 N/mm2), 12.6% (+0.160 N/mm2), and 4.3% (+20.53 mm2) for the medial compartment, respectively.
Conclusion:
Isolated DFO was inadequate to restore load distribution in meniscus-deficient knees, while concomitant LMAT restored near normal forces and improved the lateral compartment biomechanical profile.
Clinical Relevance
Our findings support the concomitant use of LMAT and varus-producing DFO in the setting of lateral meniscal deficiency with valgus malalignment. This study provides tools for the orthopaedic surgeon to individualize the correction for each patient.
Meniscal deficiency in young patients is often secondary to prior meniscectomy, significantly decreases the tibial contact area, and increases tibial contact forces. The lateral compartment is more meniscal dependent, as the lateral meniscus encompasses approximately 50% of the lateral tibial plateau and transmits 51% of the axial load across the lateral compartment compared with 30% through the medial meniscus. 36 Lateral meniscectomy is associated with a greater risk and rate of degenerative changes when compared with medial meniscectomy. 9,19,21 Paletta et al 26 showed that a total lateral meniscectomy can increase tibial contact pressure by 235% to 335%. These abnormally elevated stresses may substantially accelerate the progression of articular cartilage injury and subchondral degeneration, independently resulting in the progression of osteoarthritis (OA) within the lateral compartment of the knee. 1,10,23 In an attempt to delay degenerative disease development, lateral meniscal allograft transplantation (LMAT) has become a viable treatment option and has experienced increased clinical applicability in recent years. 29
Lateral meniscal deficiency in patients with a valgus deformity presents a unique scenario of compounded risk of articular cartilage damage. 16,31 Periarticular knee osteotomies have long been an established treatment for various pathologies in patients with coronal plane malalignment. 39 These procedures aim to correct mechanical alignment and have been used in the setting of cartilage restoration and meniscal transplantation procedures to optimize the biomechanical environment and outcomes. 17,20,39 Lateral opening-wedge varus-producing distal femoral osteotomy (DFO) has the following advantages: utilizing a single osteotomy cut; providing relative protection of neurovascular structures; and potentially having better control over the degree of correction. 5,32
DFO and LMAT have individually demonstrated to produce good clinical outcomes at short- and mid-term follow-ups. 6,22,23,29 Malalignment has been considered a contraindication to meniscal allograft transplantation (MAT) because of an increased risk of failure secondary to increased ipsilateral compartment forces. 12,35 Recent improvements in operative techniques, surgical devices, and evidence-based treatment guidelines have allowed for realignment procedures and MAT to be safely performed in combination. 18 Previous studies have shown that MAT and realignment osteotomies, when performed in combination, provide clinically meaningful patient improvements at short- and long-term follow-ups. 14,16
However, these studies are heterogeneous in terms of indications and techniques because they included patients with either medial or lateral compartment disease due to valgus or varus malalignment. There is a paucity of evidence specifically evaluating the outcomes of combined DFO and LMAT, and there are currently no available biomechanical data in the literature on the direct biomechanical influence of a transplanted meniscus in the setting of a lateral opening-wedge DFO.
The purpose of this study was to clarify the biomechanical effects of the realignment procedure in the setting of MAT. We hypothesized that given the dependence of the lateral compartment on the lateral meniscus, a DFO and increasing degrees of varus would be insufficient to restore lateral compartment pressures to normal in a lateral meniscus-deficient state. In addition, we hypothesized that LMAT would restore lateral compartment pressures to the intact state, and DFO would decrease lateral compartment pressures in all states.
Methods
Specimen Preparation and DFO
Ten fresh frozen cadaveric knees were donated to local vendors for research and subsequently purchased by our institution for testing. There were 5 male and 5 female donors (mean age, 56 years). Specimens were excluded if any history of injury, surgery, osteoporosis, OA, or degenerative joint disease of the knee was detected. Institutional review board approval was not required, as the use of cadaveric specimens is exempt from ethics review at our institution. Specimens were thawed overnight and were grossly dissected to the joint. The capsule, anterior cruciate ligament, posterior cruciate ligament, medial collateral ligament, lateral ligament complex, and anterior intermeniscal ligament were retained. The patella, quadriceps tendon, and patellar tendon were removed to facilitate exposure. The distal tibia and proximal femur were freed of all soft tissue and potted in cylindrical molds 20 cm from the joint line using polymethyl methacrylate (Frick Dental) to facilitate rigid fixation of the bone in our testing apparatus.
Before performing the opening-wedge DFO, fluoroscopy was used to determine the native anatomic alignment of each specimen to plan an appropriate bone resection needed to standardize the correction angles throughout testing. Given that no femoral head or tibial plafond was available, 6° of anatomic valgus—as measured by combining the mean anatomical lateral distal femoral angle and the anatomical medial proximal tibial angle—was used as a proxy to create neutral mechanical alignment in each knee. 23 A cortical wedge resection was then performed to create 9° of mechanical valgus when the lateral cortex was fully closed. The wedge resection was performed using an 18-mm oscillating saw blade (Stryker) and a 1-inch (2.54 cm) osteotome. The resection was started 2 cm proximal to the lateral epicondyle and followed a trajectory aimed just proximal to the medial epicondyle, and then it was completed with osteotomes under fluoroscopic guidance ending 1 cm short of the medial cortex. The second cut of the resection was made proximal to the first, meeting the first cut at the medial hinge point. Plastic wedges with custom 3-dimensional prints were made in 3° increments from 3° to 15° and were inserted into the lateral osteotomy to consistently establish the desired degree of alignment correction and to provide lateral cortical support during each testing state. Fluoroscopy was then used to validate the desired alignment with each plastic wedge before testing.
An external fixator (Large External Fixator; Synthes) was placed on the femur to maintain the desired alignment correction during testing. Two 5.0-mm Steinmann pins were placed centrally through the femoral shaft proximal to the osteotomy and 2 additional pins were placed on the anterior and posterior aspects of the femoral condyle, ensuring not to violate the articular surfaces. Four 11.0-mm carbon fiber rods, 2 laterally and 2 medially, were then secured to the construct with the appropriate clamps. These connecting rods allowed for the stabilization of the osteotomy site before, during, and after biomechanical testing. 30
Biomechanical Testing
Thin, flexible electronic pressure sensors (1500 psi; K-scan Model 4000; Tekscan Inc) were inserted between the femoral condyles and the superior surface of the tibia in the medial and lateral compartments of the knee. The sensors were placed in the submeniscal area; the anterior and posterior ends of the sensors were sutured and tethered to screws anchored to the tibia to ensure consistent placement of the sensors during all trials and to ensure the reproducibility of pressure measurements. The sensors allowed the measuring of pressures from 0.1 to 172 MPa, with an accuracy of 0.1 MPa. The sensor model was 0.1-mm thick and comprised 2 measuring fields (medial and lateral compartments), each with an area of 33 × 22–mm and a spatial resolution of 0.1 mm. The sensors were preconditioned and calibrated before testing and placement within the knee to ensure accurate measurements within the range of forces being exerted on the knee. The joint was fixed in full extension and loaded to 350 N, and sensor placement was adjusted to capture the entirety of the contact area.
The cylindrical potting on the proximal and distal ends of the knee was rigidly fixed in a custom apparatus mounted to a biaxial dynamic testing machine (Instron) at 0° flexion. A nominal compressive load (200 N) was applied to the knee, and the tibia was free to axially rotate and translate in the transverse plane to a point of stability (neutral position). The position and axial rotation of the tibia were then locked in this position for the remainder of the experiment. Specimens were loaded from 20 to 800 N of compression in the neutral position at a rate of 20 N/s with the final load held for 10 seconds, then lowered back to the initial load of 20 N over 10 10 seconds. This process was repeated for a total of 2 trials per testing condition. Each knee underwent biomechanical testing in 3 states: (1) intact and without osteotomy; (2) meniscus-deficient; and (3) meniscal transplant. States 2 and 3 were performed in a randomized order determined by a custom MATLAB script (Version R2019a; MathWorks Inc).
Experimental Condition
For each meniscal state, the following sagittal alignment conditions were tested in a randomized order by adjusting the external fixators for changing angles:
9° of mechanical valgus
6° of mechanical valgus
3° of mechanical valgus
0°
3° of mechanical varus
6° of mechanical varus
Meniscectomy and Meniscal Transplantation
After the intact specimens had undergone testing for all alignments, a complete lateral meniscectomy was performed by detaching all capsular attachments and creating tibial bone blocks that included the anterior and posterior horns. A micro-oscillating 10-mm sagittal saw (Stryker) was used to initiate the creation of the bone blocks, which were then completed using a thin osteotome. The lateral meniscus was removed en bloc from the joint, with the roots remaining attached to the bone blocks.
Lateral meniscal transplantation was performed using a modified bone trough/slot technique. The meniscus that was previously removed from the same knee was reinserted with its bone blocks into the slots created with its removal. Two 5-mm titanium interference screws (Arthrex) were inserted below the articular surface anteriorly and posteriorly to secure the bone block and meniscus for testing. Four vertical mattress meniscal capsular repair sutures utilizing ultra–high molecular weight polyethylene sutures (2-0 FiberWire; Arthrex) were then applied, securing the transplantation.
Data Analysis
Tekscan pressure data under 800 N of the compressive load were exported for each test and analyzed using a custom MATLAB script. Three primary outcomes were computed: (1) mean contact pressure (mean of all nonzero Tekscan cells); (2) mean peak contact pressure (mean of the highest 20% of Tekscan cells); and (3) total contact area. The results of the 2 trials were averaged for each test.
Statistical Analysis
To reflect the repeated-measures experimental design, 2-factor random-intercepts linear mixed-effects (LME) models were used to compare mean and peak contact pressure and contact area among the 3 experimental meniscal conditions—intact meniscus, meniscal loss, and meniscal transplant. Meniscal state was entered into the models as a categorical variable, and DFO angle was included in the models as a continuous variable with a linear effect based on exploratory descriptive analysis. An interaction model and a main effects model were constructed for each combination of endpoint and meniscal compartment, and the model with the lowest Bayesian Information Criterion was selected for reporting. When the interaction model was selected, the interaction term was interpreted, and the 1-factor LME models were constructed to interpret the effect of the meniscal state separately within each DFO angle, and vice versa. When the main-effects model was selected, the effect estimates for meniscal states were interpreted to be consistent across the range of tested DFO angles, and vice versa. The Tukey method was used to make all pairwise comparisons among meniscal states. Residual diagnostics were inspected to ensure that the assumptions were met and the model fit. An alpha level of .05 was set to interpret the statistical significance. The statistical software R Version 4.0.5 (R Core Team; with additional packages nlme and emmeans) was used for all plots and analyses.
The fixed feasible sample size and statistical power were considered for this experimental design. Assuming an alpha level of .05, a parametric-dependent comparison of group means, and 2-tailed testing, 10 specimens were sufficient to detect an effect size of d = 1.0, with an 80% statistical power.
Results
Lateral Compartment
Mean Contact Pressure
Meniscal deficiency exhibited significantly higher mean contact pressures than the intact and transplant states at every DFO correction angle (all P < .001) (Figure 1). Mean contact pressures after meniscal transplantation were not significantly different compared with the intact meniscus (all P > .6) (Table 1). In the intact meniscus, every additional 1° of the DFO correction angle contributed to an additional decrease in the mean contact pressure of –0.0402 N/mm2 (95% CI, –0.0457 to –0.0348 N/mm2; P < .001). In the meniscus-deficient state, every additional 1° of the DFO correction angle contributed to an additional decrease in the mean contact pressure of –0.1004 N/mm2 (95% CI, –0.1177 to –0.0832 N/mm2; P < .001). This resulted in each additional 1° of the DFO correction angle contributing an additional decrease of –0.06 N/mm2 (95% CI, –0.083 to –0.038 N/mm2; P < .001) in mean lateral compartment contact pressure in the meniscus-deficient state compared with the intact meniscus. In the meniscal transplant state, every additional 1° of the DFO correction angle contributed to an additional decrease in the mean contact pressure of –0.0479 N/mm2 (95% CI, –0.0560 to –0.0397 N/mm2; P < .001). This corresponded to a decrease of 5.6% for every additional 1° of the DFO correction angle as compared with transplant forces in neutral alignment. When compared with the intact meniscus at 0° (0.77 ± 0.31 N/mm2), the mean contact pressure in the lateral compartment was significantly higher than normal contact pressure at 265%, with meniscal deficiency at 0° (2.04 ± 0.81 N/mm2), and it remained elevated to 204% despite DFO correction to 3° (1.57 ± 0.47 ± 0.81 N/mm2) and 175% at 6° of varus (1.35 ± 0.41 N/mm2) (all P < .0001).

Mean contact pressures, peak contact pressures, and contact areas at corresponding DFO angles for the lateral compartment (top row) and the medial compartment (bottom row) according to the meniscal state. DFO, distal femoral osteotomy; LME, linear mixed-effects.
Mean Contact Pressure Within the Lateral Compartment by DFO Angle and Meniscal State a
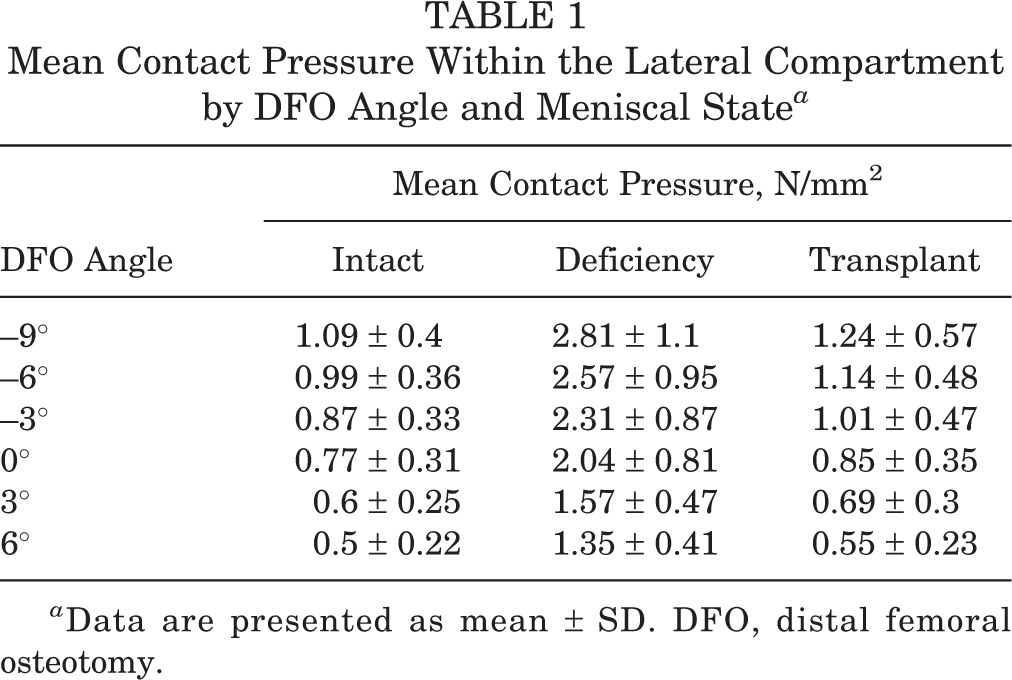
a Data are presented as mean ± SD. DFO, distal femoral osteotomy.
Mean Peak Contact Pressure
At every tested DFO angle, meniscus deficiency exhibited significantly higher mean peak contact pressure compared with the intact meniscus and meniscus transplantation (all P < .001). After meniscal transplantation, mean peak contact pressures were not significantly different compared with the intact meniscus at every correction angle (all P > .25). In the intact meniscal state, every additional 1° of the DFO correction angle contributed to an additional decrease in the mean peak pressure of –0.124 N/mm2 (95% CI, –0.146 to –0.102; P < .001) (Table 2). In the meniscus-deficient state, every additional 1° of the DFO correction angle contributed to an additional decrease in the mean peak pressure of –0.218 N/mm2 (95% CI, –0.260 to –0.177; P < .001). This resulted in each additional 1° of the DFO correction angle contributing to an additional decrease of –0.09 N/mm2 (95% CI, –0.14 to –0.04; P = .001) in mean lateral compartment peak pressure in the meniscus-deficient state compared with the intact meniscus. In the meniscal transplant state, every additional 1° of the DFO correction angle contributed to an additional decrease in the mean peak contact pressure of –0.154 N/mm2 (95% CI, –0.182 to –0.127; P < .001). This corresponded to a decrease of 5.9% for every additional 1° of the DFO correction angle as compared with transplant forces in neutral alignment. When compared with the intact meniscus at 0° (2.29 ± 1.11 N/mm2), mean peak pressure in the lateral compartment was significantly higher than normal at 210%, with meniscal deficiency at 0° (4.82 ± 2 N/mm2; P < .0001), and it remained elevated at 157% despite DFO correction to 3° (3.61 ± 1.12 N/mm2; P = .003) and 135% at 6° of varus (3.09 ± 1 N/mm2; P = .18).
Mean Peak Contact Pressure Within the Lateral Compartment by DFO Angle and Meniscal State a
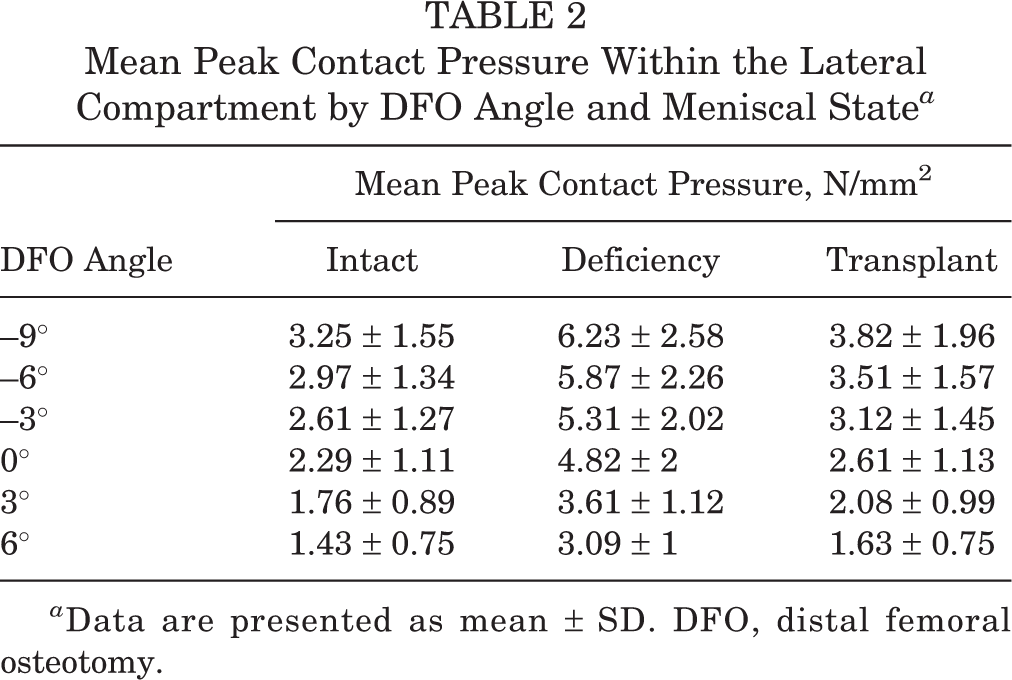
a Data are presented as mean ± SD. DFO, distal femoral osteotomy.
Total Contact Area
Meniscal deficiency produced a significantly lower total contact area compared with both the intact and the transplant states at every DFO correction angle (all P < .001). Meniscal transplantation resulted in significantly lower total contact areas compared with the intact meniscus at DFO correction angles from 9° of valgus through 0° (neutral) (all P < .05). At DFO correction angles of 3° of varus (β = 55.8 [95% CI, –9.1 to 121]; P = .010) (Table 3) and 6° of varus (β = 34.9 [95% CI, –43.6 to 113]; P = .506), the total contact area with meniscal transplantation was not significantly different from the intact meniscus. In the intact meniscal state, each additional 1° increase in the DFO correction angle resulted in a reduction in the total contact area of 10.1 mm2 (95% CI, –12.94 to –7.33; P < .001) within the lateral compartment. In the meniscus-deficient state, each additional 1° increase in the DFO correction angle resulted in a reduction in the total contact area of 3.21 mm2 (95% CI, –4.57 to –1.85; P < .001). In the meniscus-deficient state compared with the intact state, each additional 1° increase in the DFO correction angle resulted in an additional increase of 6.93 mm2 (95% CI, 2.77-11.09; P = .002) in total contact area in the lateral compartment. In the meniscal transplant state, each additional 1° increase in the DFO correction angle resulted in a reduction in the total contact area of 6.99 mm2 (95% CI, –9.27 to –4.70; P < .001). This corresponded to a decrease of 1.4% for every additional 1° of the DFO correction angle as compared with transplant forces in neutral alignment. When compared with the intact meniscus at 0° (572.98 ± 90.75 mm2), the total contact area in the lateral compartment was significantly lower than normal at 44%, with meniscal deficiency at 0° (254.6 ± 61.32 mm2; P < .0001), and it remained decreased to 44% despite DFO correction to 3° (252.26 ± 54.72 mm2; P < .0001) and to 41% at 6° of varus (234.03 ± 69.38 mm2; P < .0001).
Total Contact Area Within the Lateral Compartment by DFO Angle and Meniscal State a

a Data are presented as mean ± SD. DFO, distal femoral osteotomy.
Medial Compartment
Mean Contact Pressure
Increasing DFO correction angles resulted in higher mean contact pressures, with each additional 1° increase leading to a 0.034-N/mm2 increase within the medial compartment (95% CI, 0.029-0.040; P < .001) (Table 4). This corresponded to an increase of 7.3% for every additional 1° of the DFO correction angle as compared with forces in neutral alignment. This result was independent of the lateral meniscal state. The lateral meniscal state was not significantly associated with a change in mean contact pressure through the medial meniscus (P = .113).
Mean Contact Pressure Within the Medial Compartment by DFO Angle and Meniscal State a

a Data are presented as mean ± SD. DFO, distal femoral osteotomy.
Mean Peak Contact Pressure
Increasing DFO correction angles resulted in higher peak contact pressures, with each additional 1° increase leading to a 0.160-N/mm2 increase within the medial compartment (95% CI, 0.112-0.208; P < .001) (Table 5). This corresponded to an increase of 12.6% for every additional 1° of the DFO correction angle as compared with forces in neutral alignment. This result was independent of the lateral meniscal state. However, the lateral meniscal state was significantly associated with a change in peak contact pressure through the medial compartment (P = .029). The lateral meniscal loss state produced elevated mean peak contact pressure on the medial compartment compared with both the intact meniscal state (β = 0.236 [95% CI, 0.003-0.469]; P = .046) and the meniscal transplant state (β = 0.235 [95% CI, 0.001-0.469]; P = .049).
Mean Peak Contact Pressure Within the Medial Compartment by DFO Angle and Meniscal State a

a Data are presented as mean ± SD. DFO, distal femoral osteotomy.
Total Contact Area
Increasing DFO correction angles resulted in a higher mean total contact area, with each additional 1° increase leading to a 20.53-mm2 increase within the medial compartment (95% CI,17.87-23.18; P < .001) (Table 6). This corresponded to an increase of 4.3% for every additional 1° of the DFO correction angle as compared with forces in neutral alignment. This result was independent of the lateral meniscal state. However, the lateral meniscal state was significantly associated with a change in mean total contact area through the medial compartment (P < .001). Specifically, lateral meniscal transplantation produced mean total contact area on the medial side that was not significantly different compared with the lateral meniscus-deficient state (β = 15.54 [95% CI, –23.93 to 55.01]; P = .626) but was significantly different compared with the intact lateral meniscal state (β = –98.94 [95% CI, –138.41 to –59.46]; P < .001).
Total Contact Area Within the Medial Compartment by DFO Angle and Meniscal State a
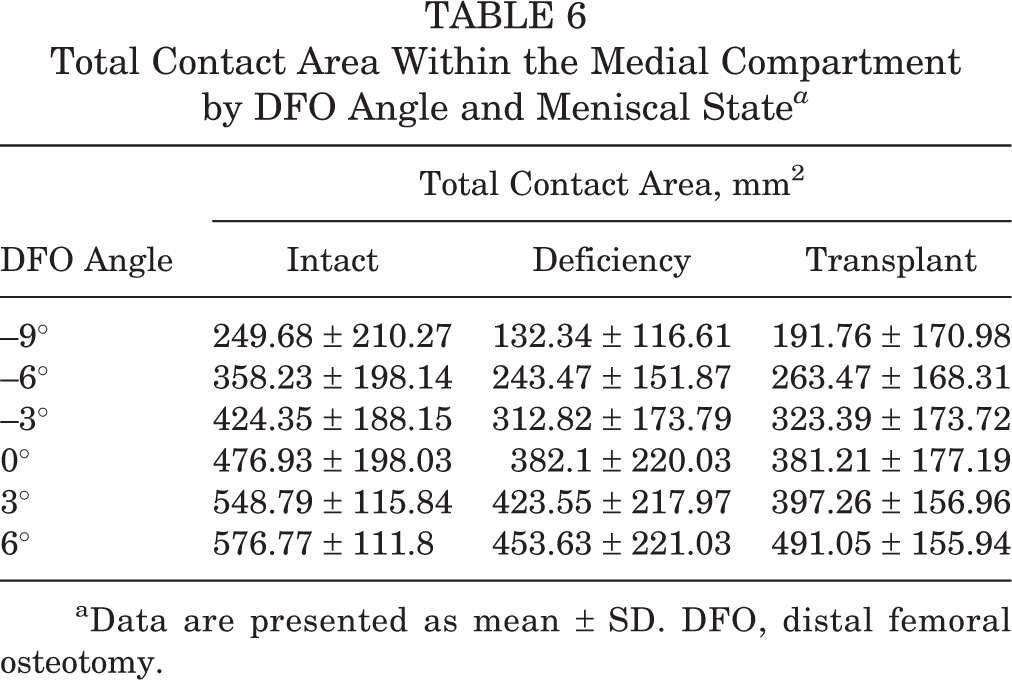
aData are presented as mean ± SD. DFO, distal femoral osteotomy.
Discussion
The findings of the present study confirm that lateral opening-wedge varus-producing DFO improves the biomechanical environment of the lateral compartment in the setting of an LMAT in the valgus knee. Meniscal deficiency demonstrated significantly increased lateral compartment pressures and decreased total contact area compared with the intact and transplant states in every testing condition. Meniscal transplantation also significantly improves mean contact and peak pressures compared with meniscal deficiency by restoring these forces back to the native meniscal intact state as thought in our hypothesis. Mean contact and peak pressures in the lateral compartment were significantly decreased with incremental varus-producing mechanical axis correction angulation. For each additional 1° of DFO correction angle, we found a decrease of 5.9% in peak pressure and a decrease of 5.6% in mean contact pressure within the lateral compartment after meniscal transplantation as compared with transplant forces in neutral alignment. Importantly, unloading the lateral compartment to both 3° and 6° of varus in the setting of meniscal deficiency was unable to restore mean contact and peak pressures back to the levels of an intact meniscus in neutral alignment. Meniscal deficiency also produced significantly lower total contact areas compared with both the intact and the transplant states. Meniscal transplantation did significantly increase total contact areas compared with meniscal deficiency. However, total contact area remained decreased compared with the intact meniscus from 9° of valgus through 0° but was restored to the level of the intact meniscus at 3° and 6° of varus.
Biomechanical changes to the medial compartment were also evaluated. Increasing varus-producing DFO correction angles resulted in higher forces, with each additional 1° increase leading to a 0.034-N/mm2 increase in mean total contact pressures and a 0.160-N/mm2 increase in peak pressures within the medial compartment. Notably, peak pressure within the medial compartment after lateral meniscal transplantation remained elevated compared with the intact meniscal state and was not significantly different compared with the lateral meniscus-deficient state. Increasing DFO correction angles resulted in higher mean total contact areas, with each additional 1° increase leading to a 20.53-mm2 increase in the area within the medial compartment. However, we did demonstrated that lateral meniscal transplantation did not fully restore the mean total contact area in the medial compartment compared with the lateral meniscus-deficient state and continued to significantly differ compared with the intact meniscal state.
Lateral meniscectomy is associated with both a significantly greater risk of tibiofemoral OA and a greater rate of deterioration when compared with medial meniscectomy. 7,9,19,21 Englund and Lohmander 9 reported radiological OA in 58% of lateral meniscectomies compared with 45% of medial meniscectomies at 15 to 22 years of follow-up. Increased permeability and reduced shear modulus have also been found in the patellofemoral articular cartilage after lateral meniscectomy in animal models. 2 Valgus knee malalignment may be constitutional or develop after partial or subtotal ipsilateral meniscectomy. 27 The combination of lateral meniscal deficiency and valgus deformity compounds the risk of articular cartilage damage. 16,31 This is supported by the present study, as meniscal deficiency resulted in significantly higher mean contact and peak pressures that were amplified with valgus malalignment.
While knee arthroplasty is an excellent treatment option for older patients with unicompartmental degenerative disease, this procedure is suboptimal in young patients with preserved joint space on radiographs who wish to return to higher-level activities. 32,34 LMAT is a viable alternative to arthroplasty for this patient population, and a varus-producing DFO can correct valgus malalignment and improve the biomechanical environment for a concomitant LMAT to heal. 15 Novaretti et al 24 found that LMAT partially restored medial translation of the tibia, and the resultant forces in the meniscal allograft were 50% to 60% of the intact lateral meniscal forces in the cadaveric model. While the authors noted that LMAT may improve but not fully restore intact meniscal kinematics, the study highlights the load-bearing function of the lateral meniscus, as the LMAT experienced increased forces in response to anterior, compressive, and rotatory loads after transplantation. In contrast, our study found that LMAT restored mean contact and peak pressures to the meniscal intact level. Additionally, we demonstrated that each incremental DFO correction in the present study resulted in significantly decreased forces across the lateral compartment and offloaded the transplanted tissue. The unloading of the lateral compartment may decrease forces and improve the healing potential of the LMAT, and it may also potentially reduce the functional burden of the lateral meniscus and improve its longevity.
Studies that evaluate the outcomes of combined DFO and LMAT are limited in the literature. Recently, Puzzitiello et al 28 evaluated a cohort of 17 patients who underwent DFO/LMAT and found significantly improved visual analog scale for pain scores and a return to sport rate of 82.4% at a mean time of 16.9 months postoperatively. When stratified by the demand level of a sport, 100%, 72.7%, and 53.3% of patients returned to low-, medium-, and high-demand sports, respectively. Also, 88.2% of these patients reported being satisfied with their ability to participate in sporting activities at the final follow-up. Cameron and Saha 4 reported on 63 patients who underwent MAT in 1997, of whom 6 also underwent a DFO. Overall, there were significantly improved outcomes and activity scores: 2 patients reported an excellent outcome, 3 patients a good outcome, and 1 patient a poor outcome. 4 Cameron et al 5 reported on 2 patients with combined DFO/LMAT in a cohort of 31 patients who underwent lateral opening-wedge DFO, and Verdonk et al 37 reviewed 2 patients with combined DFO/LMAT from a larger group of 61 patients who underwent LMAT. Gomoll et al 14 reported on 7 patients who underwent osteotomy, meniscal transplantation, and osteochondral allograft, of whom 2 had lateral-sided procedures. Overall, these studies described improved functional outcomes and return to activities in patients who underwent combined DFO/LMAT; however, overall quantitative evaluation is difficult given the small number of patients.
While there is a paucity of published results about to combined LMAT and DFO, significant literature exists that evaluates the mid- and long-term outcomes of varus-producing DFO for valgus malalignment. 5,25,33,38,40 The long-term success rate of isolated DFO has been reported to be 91% at 8 years, 64% to 87% at 10 years, but only 45% by 15 years after surgery. 3,8,11,38,40 However, these results should be interpreted with the context that most of these studies reviewed DFO in the setting of unicompartmental OA as opposed to being utilized in knee preservation surgeries with LMAT or osteochondral restoration.
The findings of this study corroborate the current literature, demonstrating that the intact meniscus and meniscal deficiency provided 5.72 cm2 and 2.55 cm2 of the lateral compartment contact area in neutral alignment, respectively. The total contact area remained decreased in the setting of meniscal deficiency despite DFO correction, likely resulting in continued focal articular cartilage loading and potentially accelerating chondral degeneration despite lateral compartment loading. Meniscal transplantation resulted in continued decreased contact areas from 9° of valgus to neutral alignment compared with the intact meniscus but was subsequently restored to the native meniscal intact levels at 3° and 6° of varus. We similarly found that mean contact and peak pressures in the lateral compartment remained significantly elevated with meniscal deficiency compared with the intact meniscus, even when unloaded to 6° of varus. This emphasizes the meniscus-dependent nature of the lateral compartment anatomy, indicating that isolated DFO is inadequate for the treatment of meniscal deficiency in the setting of a pre-arthritic knee and reinforces the benefits of LMAT in this setting. Taken together, the present findings suggest that the addition of a varus-producing DFO to biomechanical neutral alignment would be beneficial to the biomechanical environment of the lateral compartment after an LMAT.
Limitations
As with many biomechanical studies, the effects seen in this controlled laboratory experiment must be translated to the clinical setting with care. The present study represents time-zero data in regard to DFO and lateral meniscal transplantation. Results may differ after the healing of the procedures in clinical patients. Additionally, the same meniscus that was removed from the knee after the meniscus-deficient state was used in the meniscal transplant in this study. This essentially provided a “perfectly matched” transplant as opposed to true allografts used in clinical practice, which would most likely not be the exact same dimensions. Furthermore, the current testing protocol used knees in a static extension position because of maintaining the correct weightbearing alignment. Although this does provide relevant data, we acknowledge that the knee is variably influenced by the meniscus along the arc of motion. Follow-up studies should attempt to quantify the effect of a meniscal transplantation and osteotomy throughout the range of motion.
Conclusion
There is expert consensus that realignment osteotomies be performed in patients with malalignment. 13 Isolated varus-producing DFO without LMAT was unable to significantly improve lateral compartment forces after meniscal deficiency. LMAT restores lateral compartment forces back to near intact levels and DFO improves the lateral compartment biomechanical profile in the setting of an LMAT. By determining the biomechanical changes experienced within the joint for every degree of correction, the present study provides orthopaedic surgeons with a unique tool to assist in determining the desired amount of lateral compartment unloading after an LMAT and to understand the concomitant effects on forces across the medial compartment. Our findings support the use of varus-producing DFO in conjunction with LMAT to improve biomechanics across the joint and potentially delay osteoarthritic degeneration.
Footnotes
Final revision submitted October 28, 2022; accepted December 8, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: S.L. has received grant support from Arthrex; education payments from Arthrex and Smith & Nephew; and hospitality payments from Medical Device Business Services. R.M.F. has received education payments from Arthrex and Smith & Nephew; consulting fees and nonconsulting fees from Arthrex; and hospitality payments from JRF Ortho. A.F.V. has received consulting fees from Arthrex and Stryker; speaking fees from Arthrex and Smith & Nephew; and honoraria from Vericel. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval was not sought for the present study.