
Abstract
Background:
Gymnastics requires intense year-round upper and lower extremity strength training typically starting from an early age. As such, the injury patterns observed in these athletes may be unique.
Purpose:
To characterize the types of injuries and provide return-to-sport data in male and female collegiate gymnasts.
Study Design:
Descriptive epidemiology study.
Methods:
A conference-specific injury database was utilized to perform a retrospective review of injuries for male and female National Collegiate Athletic Association (NCAA) Division I gymnasts within the Pacific Coast Conference between 2017 and 2020 (N = 673 gymnasts). Injuries were stratified by anatomic location, sex, time missed, and injury diagnoses. Relative risk (RR) was used to compare results between sexes.
Results:
Of the 673 gymnasts, 183 (27.2%) experienced 1093 injuries during the study period. Injuries were sustained in 35 of 145 male athletes (24.1%) as compared with 148 of 528 female athletes (28.0%; RR, 0.86 [95% CI, 0.63-1.19]; P = .390). Approximately 66.1% (723/1093) of injuries occurred in a practice setting, compared with 84 of 1093 injuries (7.7%) occurring during competition. Overall, 417 of 1093 injuries (38.2%) resulted in no missed time. Shoulder injuries and elbow/arm injuries were significantly more common in male versus female athletes (RR, 1.99 [95% CI, 1.32-3.01], P = .001; and RR, 2.08 [95% CI, 1.05-4.13], P = .036, respectively). In total, 23 concussions affected 21 of 673 athletes (3.1%); 6 concussions (26.1%) resulted in the inability to return to sport during the same season.
Conclusion:
For the majority of musculoskeletal injuries, the gymnasts were able to return to sport during the same season. Male athletes were more likely to experience shoulder and elbow/arm injuries, likely because of sex-specific events. Concussions occurred in 3.1% of the gymnasts, highlighting the need for vigilant monitoring. This analysis of the incidence and outcomes of injuries observed in NCAA Division I gymnasts may guide injury prevention protocols as well as provide important prognostic information.
Competitive gymnastics is a uniquely demanding sport that requires frequent, intense year-round upper and lower body strength and flexibility training typically starting at a very young age. 10,13 The distinctive biomechanics and repetitive high-impact forces in combination with the required body control and landing techniques possibly subject competitive artistic gymnasts to injury patterns that may be quite unique. 7 In the United States alone, there are >5 million individuals >6 years of age who participate in gymnastics. 26 As the popularity of gymnastics continues to increase, the injury patterns in these athletes continue to be a topic of interest. 15,26
Although there is emerging evidence on the injury characteristics in competitive gymnastics, prior studies on gymnasts have focused primarily on female athletes, were limited to 1 team, or were limited by variability in study participants’ age and skill level. 15,18,21,24,32,33,39 Even among studies that primarily investigated collegiate gymnastics, reported injury rates varied from 8.8 to 16.6 injuries per 1000 athlete-exposures. 15,21,32,33,39 This variability in injury rates is likely due to the heterogeneity of each of these studies, as they include a wide range of ages, study periods, and skill levels. Injury rates are invariably related to the level of the gymnast, thus further contributing to the discrepancy in findings. 5,13
Injuries in competitive gymnastics are thought to be due to both acute traumatic injuries from high impact and overuse injuries from frequent, intense training. 5,11,13,32 Overuse injuries, in particular, warrant close attention in this population given the frequent, intense training as well as the increased trend toward early specialization of young gymnasts. 3,5,11,13,32 Overuse injury rates vary from 23.3% to 44.2% of injuries in female gymnasts and from 27.0% to 39.7% of injuries in male gymnasts. 5 These rates are some of the highest rates among all sports, including basketball, rugby, soccer, and volleyball. 35 Even more alarming, a recent study revealed that a majority of overuse injuries can be reduced with adequate load monitoring and careful adoption of individualized training. 8 As such, a thorough understanding of the injury patterns that plague gymnasts is the crucial first step to understanding how to prevent them.
Given the unique demands placed on the body in gymnastics, return-to-play decisions after an injury present a challenge to sports medicine physicians. 36 Physicians must weigh the risks and benefits of allowing an athlete to return to frequent, high-impact practice and competition, occasionally without any clear principles to provide guidance. The competitive nature of collegiate athletes also complicates clinical decision making, as these athletes may feel the need to train despite pain or minimize their pain. 2 Thus, there is an identified need for literature analyzing how injuries affect return to play and how long injuries typically prevent gymnasts from competing. 36
By utilizing a conference-specific national collegiate injury database, we aimed to investigate the injury patterns among National Collegiate Athletic Association (NCAA) Division I male and female gymnasts, determining any sex-specific differences between injury patterns and analyzing how these injuries affect return to sport.
Methods
Men’s and women’s collegiate gymnastics rosters for all university teams in the Pacific Coast Conference (Pac-12) were collected during the 2016-2017, 2017-2018, 2018-2019, and 2019-2020 academic years to determine the total number of athletes to be included in this data set. Individual websites from the respective institutions were used to create this roster, and athletes who remained on the team roster for multiple years were not counted more than once. Furthermore, athletes who transferred within the Pac-12 conference were not included in this analysis.
After receiving institutional review board approval for the study protocol and given our institution’s membership in the Pac-12, we queried the Pac-12 Sports Injury Research Archive between 2017 and 2020 in the same fashion as prior studies. 34,37 Included for analysis were all male and female collegiate gymnasts from Pac-12 universities (2 men’s teams and 8 women’s teams) who had a documented “injury event” as reported by a physician, athletic trainer, or physical therapist during either practice or competition, both in season and out of season. “Athletes affected” was defined as the number of athletes who experienced ≥1 recorded injury during the study period. Injuries were stratified by setting, body location, year, and diagnosis. All these stratifications were further substratified by sex. Injury setting was defined as where the injury took place and included practice facility, competition facility, weight room, other facility, or not specified. Body locations included for analysis were as follows: head/face, spine/neck, chest/abdomen, shoulder, elbow/arm, forearm/wrist/hand, groin/hip/pelvis/buttock, knee/thigh, lower leg/ankle/foot, or not specified.
As in prior studies, 25,31 injury incidence per 1000 athlete-exposure hours (AEH) was calculated using the following equation:

Total athlete time at risk was calculated by multiplying the number of weeks in a season (15 weeks) by 20 hours per week, as well as by multiplying the number of weeks out of season (16 weeks) by 8 hours given that this is the maximum duration of sport allowed according to NCAA and Pac-12 bylaws. The Pac-12 website was used to determine season start and end dates as well as off-season training dates. 27,28
When available, return-to-play data were also documented. This included whether there was any time missed away from sport (practice or in-season competition), if the athlete was able to return during the same season, if the athlete was unable to return until the following season (season ending), or if the athlete was unable to return to sport completely (career ending). The most common diagnoses as well as their associated return-to-play data were also reported, with these also being stratified by sex.
Statistical Analysis
Similar to a prior study utilizing the Pac-12 injury database, 37 we defined the percentage of injury events for each stratification as the number of specific injuries divided by the total number of injuries. The percentage of athletes affected for each stratification was defined as the number of athletes affected at least once by the specific injury divided by the total number of gymnasts included in this study. In order to analyze sex-based differences for all stratifications, relative risk (RR) for the percentage of athletes affected was utilized and an associated 95% CI and P value were calculated. Statistical significance was defined as a P value <.05. Statistical analyses were performed using Microsoft Excel Version 16.49 (Microsoft Corp).
Results
Overall, 673 gymnasts were included in the analysis. The results indicated that 27.2% of the gymnasts (183/673) experienced 1093 total injuries between 2017 and 2020. Each injured gymnast experienced a range of 1 to 32 injuries. Of 145 male athletes, 35 (24.1%) as compared with 148 of 528 female athletes (28.0%; RR, 0.86 [95% CI, 0.63-1.19], P = .390) experienced an injury. The injury incidence per 1000 AEH was calculated to be 2.26. Approximately 66.1% (723/1093) of injuries occurred in a practice setting, compared with just 84 of 1093 injuries (7.7%) occurring during competition. Male athletes were significantly less likely to sustain an injury during competition than female athletes (RR, 0.37 [95% CI, 0.15-0.92]; P = .031). A total of 626 of 1093 injuries (57.3%) resulted in missed time away from sport, and 417 injuries (38.2%) resulted in no missed time away from sport. Return-to-sport data were unavailable for 50 injuries (4.6%) (Table 1).
Injury Data Stratified by Year, Setting, and Any Time Missed for Male and Female Collegiate Gymnasts, 2017-2020 a

a Data are reported as n (%) unless otherwise indicated. RR, risk ratio (male vs female).
b Statistically significant difference between male and female athletes (P < .05).
The most common injuries were foot/ankle/lower leg (376/1093; 34.4%), knee/thigh (176/1093; 16.1%), shoulder (150/1093; 13.7%), spine/neck (134/1093; 12.3%), and hand/wrist/forearm injuries (96/1093; 8.8%). Shoulder injuries were significantly more common in male gymnasts (RR, 1.99 [95% CI, 1.32-3.01]; P = .001). Elbow/arm injuries were also significantly more common in male gymnasts (RR, 2.08 [95% CI, 1.05-4.13]; P = .036) (Table 2).
Injuries Stratified by Body Location for Male and Female Collegiate Gymnasts, 2017-2020 a

a Data are reported as n (%) unless otherwise indicated. The dash indicates calculation not applicable. RR, risk ratio (male vs female).
b Statistically significant difference between male and female athletes (P < .05).
The most common injury diagnoses were lumbar muscle strains/spasms/imbalance (61/1093; 5.6%); ankle sprains (60/1093; 5.5%), with lateral ankle sprains accounting for 70% (42/60); Achilles tendinopathy (23/1093; 2.1%); and concussion (23/1093; 2.1%). Male athletes experienced significantly more shoulder impingement/synovitis than female athletes (RR, 7.28 [95% CI, 1.84-28.77]; P = .005) (Table 3).
Most Common Injury Diagnoses for Male and Female Collegiate Gymnasts, 2017-2020 a

a Data are reported as n (%) unless otherwise indicated. Dashes indicate calculation not applicable. MTSS, medial tibial stress syndrome; RR, risk ratio (male vs female).
a Statistically significant difference between male and female athletes (P < .05).
Although lumbar muscle strains/spasms/imbalance were the most common injuries, only 39.3% (24/61) resulted in missed time, with all those athletes returning within the same season. A total of 7.1% (3/42) of lateral ankle sprains were season ending. In total, 23 concussions affected 21 of the 673 athletes (3.1%). A total of 2.8% (4/145) of the male gymnasts experienced a concussion as compared with 3.2% (17/528) of female gymnasts (RR, 0.86 [95% CI, 0.29-2.51]; P = .784). While all concussions resulted in missed time, 73.9% (17/23) of concussions resulted in the ability to return to sport during the same season. A total of 13.0% (3/23) of the concussions were season ending, and 2 of 23 concussions (8.7%) were career ending. Follow-up data for 1 concussion were unavailable (Table 4).
Return to Play Data for the Most Common Injury Diagnoses a
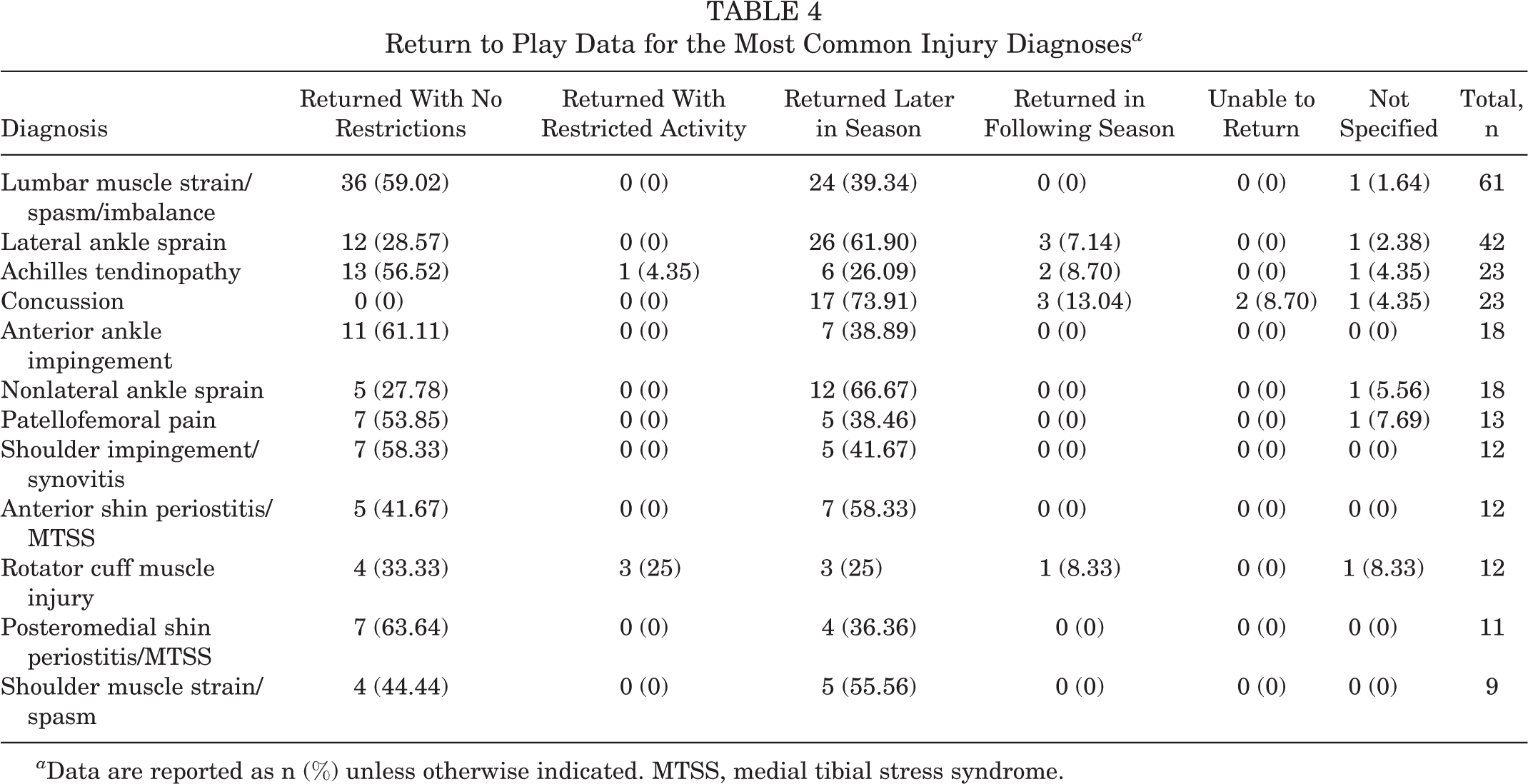
a Data are reported as n (%) unless otherwise indicated. MTSS, medial tibial stress syndrome.
A total of 1.6% of injuries were career ending (17/1093), with all those injuries occurring in female athletes. Knee ligament sprains accounted for 3 of (17.6%) those injuries, knee ligament tears accounted for an additional 3 (17.6%), and concussions accounted for 2 (11.8%). Other causes of career-ending injuries were a knee/thigh tendon rupture, knee chondral damage, thigh muscle strain, ruptured ankle/lower leg tendon, shoulder subluxation, spinal disk degeneration, and an adductor strain.
In total, 21 fractures were noted during the study period, 9 (42.9%) of which occurred in the foot/ankle/lower leg and 6 (28.6%) of which occurred in the hand/wrist/forearm. Twenty dislocations were noted during the study period, with 9 (45.0%) localized to the hand/wrist/forearm. The most common tendon ruptures occurred in the foot/ankle/lower leg (10/13; 76.9%), with 9 of those 10 (90.0%) occurring in female athletes. Eight out of 10 (80%) of all ligament tears occurred in the knee, with all these injuries occurring in female athletes (Table 5).
Fracture, Dislocation, Tendon Rupture, and Ligament Tear Injuries Stratified by Body Location for Male and Female Collegiate Gymnasts, 2017-2020 a

a Data are reported as n (%) unless otherwise indicated. Dashes indicate calculation not applicable. RR, risk ratio (male vs female).
Discussion
In this study, we used an injury database in order to better characterize injuries and their effect on return to sport among collegiate competitive gymnasts. Although we only analyzed gymnasts from the Pac-12 conference, we believe these results are likely comparable with all collegiate gymnasts. Our findings indicated that the injury incidence per 1000 AEH in collegiate gymnasts was 2.26. This is generally consistent with prior literature indicating an injury incidence of 2.16 per 1000 exposure hours in precollegiate female gymnasts, with evidence of higher rates in this population at more competitive levels. 18,22,31 This injury rate has been previously reported as being comparable with American football as well as wrestling, 2 of the most injury-prone sports. 22 Given the intense training starting at an early age associated with gymnastics, it is important that injury rates continue to be monitored and published so that training protocols can be optimized and these athletes can be counseled appropriately.
A total of 24.1% of male gymnasts experienced an injury, with a comparative injury rate of 28.0% seen in female gymnasts. Although there was no significant difference in overall injury rates between the sexes (P = .390), several sex-based differences were noted in this study. Male athletes experienced significantly more shoulder and elbow/arm injuries (RR, 1.99 [95% CI, 1.32-3.01], P = .001; and RR, 2.08 [95% CI, 1.05-4.13], P = .036, respectively). Existing literature confirms that male gymnasts sustained mostly upper limb injuries, with female gymnasts sustaining mostly lower limb injuries. 5,39 This is very likely due to differences in events, with women competing in events that place relatively more stress on the lower body (vault, uneven parallel bars, beam, and floor) compared with men, who compete in events that place relatively more stress on the upper body (floor, pommel horse, rings, vault, even parallel bars, and high bar). The pommel horse and the high bar, both exclusively male events, have also been shown to potentially predispose male gymnasts to hand and wrist injuries. 4,39 Interestingly, female gymnasts were significantly more likely to experience an injury during competition than male gymnasts (RR, 0.37 [95% CI, 0.15-0.92]; P = .031). The exact reason for this finding in this study is unknown; however, one plausible rationale is that psychosocial factors have been shown to discourage male athletes from reporting symptoms compared with female athletes. 16
We also found that 9 fractures occurred in the foot/ankle/lower leg, with rates comparable in male and female gymnasts. Gymnastics has been shown to have some of the highest rates of stress fractures among all sports, with these injuries mostly attributed to overuse. 30 As such, although the exact mechanism of fractures observed in this study is unknown because of limitations of the study database, it is likely that many of the fractures reported were overuse-related stress fractures. In addition, we found that 8 ligament tears occurred in the knee, with all these injuries occurring in female gymnasts. With female athletes at a substantially higher risk of experiencing an anterior cruciate ligament rupture among collegiate athletes, the fact that all observed knee ligament tears occurred in female athletes is somewhat expected. 1,12 Ligament tears in gymnasts have been thought to be the result of trauma during landing, suggesting dismount/landing as a possible mechanism. 5,26
The results indicated that 7.1% of ankle sprains were season ending. These injuries likely occur during takeoff and landing. The treatment of these injuries typically requires immobilization for a period of time, followed by physical therapy focusing on ankle strengthening and proprioception training. 13 One possible rationale for the relatively high incidence of season-ending ankle sprains seen in this study is the increased force at the time of injury. As seen in basketball players, this may lead to chronic ankle instability and may possibly delay return to sport, thus highlighting the importance of full ankle strength to return to sport. 20 If gymnasts have not fully recovered from an ankle sprain, they may not be able to maintain appropriate balance and proprioception and subsequently lack the ability to place the high magnitude of forces on their ankle that are required to competitively partake in their events. Gymnasts are also unable to wear rigid, supportive ankle braces when performing, further necessitating a higher level of recovery before returning to play.
Research suggests that injuries in competitive gymnasts occur far more frequently in competition compared with a practice setting. 21 This is not consistent with the results of the current study, as far more injuries occurred during practice versus competition. Although we did not have data on how many practices were held overall and thus could not accurately compare injury frequency that occurred in practice versus competition, findings indicated that the injuries that occurred during practice (n = 723) were >8 times the injuries that occurred in competition (n = 84). A recent study by Chandran et al 6 found an upward trajectory of practice injury rates and suggested that early specialization in sport may be a contributing factor. As athletes continue to specialize in yearlong gymnastics at an early age, the risk of overuse injuries may become higher, especially in a practice setting, where they may be repeatedly performing the same technically difficult maneuvers in order to master them. 3,11,32 According to a study by Kolar et al, 17 gymnasts perceived the cause of their injuries to be related to poor technique, improper methods of teaching, and training by overload. As such, appropriate technique, adequate stretching, and other injury treatment prevention strategies must be employed in a practice setting as well as in a competitive setting.
There is a relative lack of literature investigating the incidence of concussions in gymnastics and how concussions affect return to play. 13 Concussions can occur when gymnasts hit their head on an apparatus/mat or hit their chin with their own knee when in a flip/tuck position. 14 In the current study, there were 23 concussions that affected 21 of 673 athletes (3.1%), with comparable rates between male and female gymnasts. Although not reaching rates seen in football, wrestling, men’s and women’s lacrosse, and women’s soccer, the reported rate of concussions in this study is still substantial. 29,38 It is crucial that coaches and health care providers remain highly vigilant for concussive symptoms, as gymnasts may play through pain, worsening their symptoms and ultimately prolonging their recovery time. 2,9
All concussions resulted in missed time, but in 73.9% of concussions, the athlete was able to return the same season. Return to sport after concussion for gymnasts may be particularly challenging, as the athlete must return to not only high-impact activities, but also activities that involve positions of inversion, twisting, and air awareness, all of which can worsen postconcussive symptoms. 13 Gymnasts can place themselves in danger of serious injury should they experience an impaired sense of position in space during inversion (colloquially named the “twisties” among elite gymnasts), due to either task-specific dystonia or possibly returning to sport too soon after a concussion. 19 Therefore, it is of great importance that an athlete meets established criteria before returning to play after a concussion.
Limitations
This study has a number of limitations, including those inherent to its retrospective nature. Similar to prior studies utilizing this injury database, diagnoses could be assigned by athletic trainers, physical therapists, primary care physicians, orthopaedic surgeons, and psychologists. 37 As the diagnostician is undefined in this data set, this presents a theoretical inconsistency with regard to diagnostic criteria. Furthermore, injury reporting within this database became more standardized during 2018, possibly attributing to the low injury rates seen in 2017 and 2018. Exposure time was also assumed to be the maximum time allotted by the NCAA. Additionally, event/apparatus-specific data were not available, limiting any analysis regarding potential mechanisms of injury as well as determining whether injuries were traumatic or overuse in nature. As noted by McSweeney et al, 23 biomechanical data are needed for comprehensive risk stratification and the complete design of injury prevention and return-to-play programs. Additionally, in order to maintain de-identification of the data set, details regarding an athlete’s educational class (freshman, senior, etc) as well as the specific number of days, weeks, or months an athlete missed were omitted and thus could not be reported in the current study. This data set also did not report on the treatment of any injuries, limiting any analysis on treatment regimens. Given that there were only 10 total teams included for analysis, this study alone is not exhaustive enough to allow for the development of robust injury prevention protocols. However, it is one of the only studies to date that has analyzed time away from sport based on injury among both male and female intercollegiate competitive gymnastics athletes and constitutes an important first step in developing prognostic data that clinicians can use to guide these athletes.
Conclusion
The relatively comprehensive nature of this multicenter data capture makes this analysis a valuable contribution to our epidemiological understanding of factors related to athletic injuries among competitive gymnasts. The results of this study highlight the importance of injury prevention and the implementation of these practices at both practices and competitions. Furthermore, coaches and medical staff members should be particularly vigilant when looking for concussive symptoms in both male and female collegiate gymnasts. Establishing skill-specific injury prevention techniques among these at-risk athletes starts with an understanding of the injury characteristics that affect both male and female athletes and how these injuries can affect return to play. Thus, the information presented here may better equip health care providers to guide the expectations for these athletes, ultimately optimizing the patient-athlete relationship while keeping our collegiate gymnasts safe.
Footnotes
Final revision submitted October 31, 2022; accepted December 8, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: D.J.C. has received grant support from Arthrex and education payments from Smith & Nephew. K.J.J. has received education payments from Arthrex and Micromed; consulting fees from Linvatec; nonconsulting fees from Arthrex, Linvatec, and Vericel; and honoraria from JRF Ortho, MTF, and Vericel. T.J.K. has received education payments from Micromed, consulting fees from Heron Therapeutics, honoraria from Fidia Pharma and MTF, and hospitality payments from Surgalign Spine Tech. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of California, Los Angeles (reference No. 20-000264).