
Abstract
Background:
A force-based tension protocol that uses a certain amount of tension at graft fixation could still give rise to variations in initial constraint levels of the knee joint in terms of side-to-side difference (SSD) in anterior translation.
Purpose:
To investigate the factors influencing the initial constraint level in anterior cruciate ligament (ACL)–reconstructed knees and compare outcomes according to the level of constraint in terms of anterior translation SSD.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Included were 113 patients who underwent ipsilateral ACL reconstruction using an autologous hamstring graft and had minimum 2-year follow-up outcomes. All grafts were tensioned and fixed at 80 N using a tensioner at the time of graft fixation. The patients were classified into the following 2 groups according to the initial anterior translation SSD, measured using the KT-2000 arthrometer: a physiologic constraint group with restored anterior laxity ≤2 mm (group P; n = 66) and a high-constraint group with restored anterior laxity >2 mm (group H; n = 47). Clinical outcomes were compared between the groups, and preoperative and intraoperative variables were evaluated to identify factors affecting the initial constraint level.
Results:
Between group P and group H, generalized joint laxity (P = .005), posterior tibial slope (P = .022), and anterior translation measured in the contralateral knee (P < .001) were found to differ significantly. Measured anterior translation in the contralateral knee was the only significant predictor of high initial graft tension (P = .001). No significant differences were found between the groups regarding clinical outcomes and subsequent surgery.
Conclusion:
Greater anterior translation measured in the contralateral knee was an independent predictor of a more constrained knee after ACL reconstruction. The short-term clinical outcomes after ACL reconstruction were comparable, regardless of the initial constraint level in terms of anterior translation SSD.
Keywords
The ultimate goal of anterior cruciate ligament (ACL) reconstruction is the restoration of the native knee kinematics by replacing an injured ACL with a functional graft. 9 In particular, adequate tension of the graft restraining anterior-to-posterior or rotational translation is necessary to reestablish the stability of the knee. 27,40 An undertensioned graft can be nonfunctional and lead to an unstable knee with excessive laxity, while an overtensioned graft can cause loss of extension, graft breakdown, and osteoarthritis attributed to altered tibiofemoral biomechanics. 7,34,36,39,55 The initial graft tension is determined by the applied tension at the time of graft fixation with the use of manual or device-assisted tensioning protocols and influences the outcomes of the ACL reconstruction. 1,10,40,46,54 Therefore, graft tension at the time of fixation is considered one of the key factors for successful ACL reconstruction. 48
The application of the initial graft tension at the time of graft fixation is based on either the applied force on the graft itself or the relative anterior-to-posterior translation of the reconstructed knee compared with the contralateral uninjured knee. 33 In the force-based tensioning protocol, the surgeon applies a certain amount of force to the graft manually or with a tensioning device. With the use of various tensioning devices, consistent quantitative tension can be applied to the graft. 45 On the other hand, the laxity-based tensioning protocol applies initial tension that is individualized for each patient by matching the laxity of the uninjured knee using an arthrometer. 5,14
Several studies have compared the amount of initial tension of force-based protocols to determine the level that produces the best clinical outcomes. 23,40,50,54,56 However, the optimal amount of initial tension remains unclear, and there is variability in adopted tensioning protocols among surgeons. The current trend in practice involves 50 to 80 N of relatively high initial tension with the use of a tensioning device that can produce a reduced side-to-side difference (SSD; compared with the contralateral healthy knee) in anterior laxity and a lower failure rate compared with using a lower tension. 3,26,27,37 Previous studies have compared 2 laxity-based protocols: a high-tension protocol that overconstrains the anterior-to-posterior translation by 2 mm versus the contralateral knee, and a low-tension protocol that adjusts it to within 1 mm. 1,15 Both laxity-based protocols have produced similar outcomes.
Even though the same amount of initial tension is applied to the graft, there may be individual variations in initial constraint levels of the knee joint in terms of anterior translation SSD. However, the effect of the force-based initial tension on initial anterior translation SSD and ACL reconstruction outcomes have not yet been elucidated.
The purpose of the study was to (1) investigate the factors influencing the initial constraint level of the ACL-reconstructed knee in terms of anterior translation SSD and (2) compare patient outcomes according to constraint level. We hypothesized that patients with a more constrained knee would experience better clinical outcomes after ACL reconstruction.
Methods
Study Population
We reviewed the records of 286 consecutive patients who underwent single-bundle ACL reconstruction between January 2015 and January 2019; all procedures were performed by a single senior surgeon (S.H.-K.) with the transportal technique using an autologous quadruple hamstring graft. Patients were included if they were aged 15 to 50 years. Exclusion criteria were as follows: (1) revisional ACL reconstruction; (2) concomitant ligamentous injury; (3) meniscectomy of more than one-third of the meniscus; (4) cartilage lesion of International Cartilage Regeneration & Joint Preservation Society grade ≥3; (5) >12 months elapsed from injury to surgery; (6) previous contralateral ACL reconstruction; (7) osteoarthritis classified as Kellgren-Lawrence grade >1; (8) history of previous knee surgery; (9) postoperative infection; and (10) <2 years of follow-up data. Ultimately, 113 patients were included in the study. The institutional review board of our institution approved the study and waived the requirement for obtaining informed patient consent.
The study patients were then classified into 2 groups according to the initial postoperative anterior translation SSD, measured immediately after surgery using a KT-2000 arthrometer (MEDmetric) with a force of 134 N. Patients with an initial anterior translation of the affected knee ≤2 mm of that of the contralateral knee were assigned to the physiologic constraint group (group P; 66 patients), and those who were overconstrained (>2 mm) were assigned to the high-constraint group (group H; 47 patients) (Figure 1). 15,16

CONSORT (Consolidated Standards of Reporting Trials) flowchart of the inclusion and exclusion process. ACL, anterior cruciate ligament; ICRS, International Cartilage Regeneration & Joint Preservation Society; SSD, side-to-side difference.
Operative Procedures and Tensioning Protocol
Before the operation, the anterior laxity of the affected and contralateral knees at 20° of knee flexion, measured using a KT-2000 arthrometer with a force of 134 N, were evaluated under anesthesia. 38 The measured values of the affected knee were recorded and compared with those of the contralateral knee. Rotational laxity, measured using a manual pivot-shift test, was assessed and graded as either 0 (absent), 1 (glide), 2 (clunk), or 3 (transient lock). 29
Diagnostic arthroscopy was performed in each compartment of the knee using a parapatellar high anterolateral portal. Concomitant meniscal tears were managed with an appropriate surgical option in consideration of the patient factors and tear characteristics before the ligament reconstruction. 21 After identification of the ACL injury via diagnostic arthroscopy, the semitendinosus and gracilis tendons were harvested for a quadrupled graft. After the removal of excess muscular and unstable tendinous tissues from the tendons, both ends of each tendon were whipstitched, and the tendons were folded in half in a 4-stranded configuration. The graft was pretensioned at approximately 88 N for 20 minutes using a graft preparation board (Graft Master III; Smith & Nephew). 20,42 The femoral tunnel and tibial tunnel for ACL reconstruction were created on the respective footprints of the ACL in reference to ACL remnants and anatomic landmarks with a diameter matched to the prepared graft. 18,53 An accessory anteromedial portal, just above the medial meniscus, was used to create the femoral tunnel.
The graft was inserted into the femoral tunnel with a fixed-loop cortical suspensory device (Endobutton CL; Smith & Nephew) and pulled through the tibial tunnel distally with a force of 80 N by using a tensioning device (SE Graft Tensioning System; ConMed). Thereafter, the graft was preconditioned with 20 flexion-extension cyclic loads. Along with tension maintenance, the graft was fixed with a bioabsorbable interference screw in the tibial tunnel and supplemented with a cortical screw and washer outside the tibial tunnel. The immediate postoperative anterior translation of the operated and contralateral knees was recorded after aseptic dressing.
Immediately after the operation, crutch-assisted tolerable weightbearing was allowed, and exercises for range of motion (ROM) and isometric quadriceps strengthening were encouraged.
Clinical Assessment
The presence of generalized joint laxity (GJL) was evaluated according to the Beighton and Horan criteria by a point score of ≥4 preoperatively. 6,24 The affected knee was not included in the evaluation of GJL, to preclude the effect of injury to the knee ROM.
The patients were followed up at 3, 6, 9, 12, and 24 months postoperatively. At every visit, anterior knee laxity was evaluated using the KT-2000 arthrometer as well as with stress radiography, performed with a force of 150 N using a Telos stress device (Telometer; Daiseung Medics) at 30° of knee flexion in the lateral decubitus position. Along the reference line parallel to the medial tibial plateau, 2 intersection points on the reference line were determined by the lines perpendicular to the reference line and tangential to the midpoint between the most posterior contour of the medial and lateral femoral condyles (line F) and tibial condyles (line T). 19,31 The values of anterior translation as determined by stress radiography were presented positively if the intersection point of the reference line and line T was anterior to the intersection point of the reference line and line F along the reference line, and negatively if not.
Rotational knee laxity was assessed using manual pivot-shift testing. The International Knee Documentation Committee (IKDC) examination was used for assessing ACL reconstruction outcomes objectively. 16 All physical examinations were performed by the senior surgeon.
Radiographic assessments were performed using simple radiographs. The hip-knee-ankle angle was measured with weightbearing on an entire lower extremity anteroposterior radiograph. The posterior tibial slope was measured on the lateral radiograph by the angle between the line drawn tangentially to the tibial plateau and the line drawn through the anatomic axis of the proximal tibia. 51
Functional assessments were conducted using the Lysholm knee score, Tegner activity scale, Knee injury and Osteoarthritis Outcome Score, and IKDC subjective score preoperatively and at every follow-up visit. 8,32,43,47 Subsequent surgical procedures were reviewed from medical records and verified by telephonic interview for all patients.
Statistical Analysis
The sample size was calculated using G*Power (Version 3.1), based on a pilot study of patients who satisfied the inclusion and exclusion criteria between January 2016 and January 2018. 12 The sample size was chosen to be able to differentiate anterior laxity at the 2-year follow-up between the groups. The minimum sample size required was 36 per group, with a significance level (α) of 5% and power (1 – β) of 80%.
The independent t test or Mann-Whitney U test was used for continuous variables, and the chi-square or Fisher exact test was used for categorical variables. Multivariable linear regression was used to compare the clinical outcomes between the groups considering the presence or absence of GJL as a confounding factor. Univariable and multivariable logistic regression analyses using the enter method were applied to identify factors influencing the initial constraint level of the reconstructed knee joint. A receiver operating characteristic curve was used to determine the cutoff point for a preoperative variable that predicted postoperative overconstraint. The threshold for significance was set at P < .05. SPSS (Version 26.0; IBM) was used for statistical analysis.
Results
The mean initial anterior translation SSD was –0.5 ± 1.2 mm in group P and –4.1 ± 1.5 mm in group H (P < .001). No patient showed loose tension (>2 mm SSD). GJL was significantly more common in group H than in group P (P = .005) (Table 1). Anterior translation as measured in the contralateral knee was significantly higher in group H than in group P (P < .001), while that of the affected knee was similar between the groups (Table 2). The posterior tibial slope was significantly lower in group H than in group P (P = .022). All other patient characteristics and preoperative and intraoperative variables were comparable between the groups (Appendix Table A1).
Comparison of Characteristics Between the Study Groups a

a Data are reported as mean ± SD or n (%). Boldface P value indicates a statistically significant difference between groups (P < .05).
Comparison of Preoperative Variables Between the Study Groups a

a Data are reported as mean ± SD or n (%). Boldface P values indicate a statistically significant difference between groups (P < .05). ADL, Activities of Daily Living; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; QOL, Quality of Life; SSD, side-to-side difference.
b Positive values indicate varus alignment; negative values indicate valgus alignment.
Anterior laxity of the reconstructed knee increased gradually over time (Figure 2). The SSDs in anterior translation in both groups increased significantly until 6 months postoperatively (P < .05) and differed significantly between the groups at 3 (P < .001) and 6 (P = .006) months. However, knee stability, knee ROM, and clinical outcomes at the 2-year follow-up were similar between the groups (Table 3). The clinical outcomes at the 2-year follow-up were comparable between the groups, even considering the presence or absence of GJL as a confounding factor (Table 4).

Changes in anterior translation side-to-side difference (SSD) measured with a KT-2000 arthrometer over a 24-month period. Only patients in whom we were able to obtain measurements at every follow-up visit are included (group P, n = 42; group H, n = 28). *Significantly different between follow-up periods (P < .05). ‡Significantly different between groups (P < .05).
Comparison of 2-Year Postoperative Outcomes Between the Study Groups a

a Data are reported as mean ± SD or n (%). ADL, Activities of Daily Living; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; QOL, Quality of Life; SSD, side-to-side difference.
b Patients who underwent revision or contralateral anterior cruciate ligament reconstruction during the 2-year follow-up were excluded from the final postoperative outcome evaluation (group P, n = 3; group H, n = 4).
Multivariable Linear Regression of Postoperative Outcomes at the 2-Year Follow-up Considering Both Initial Knee Constraint Level and GJL a
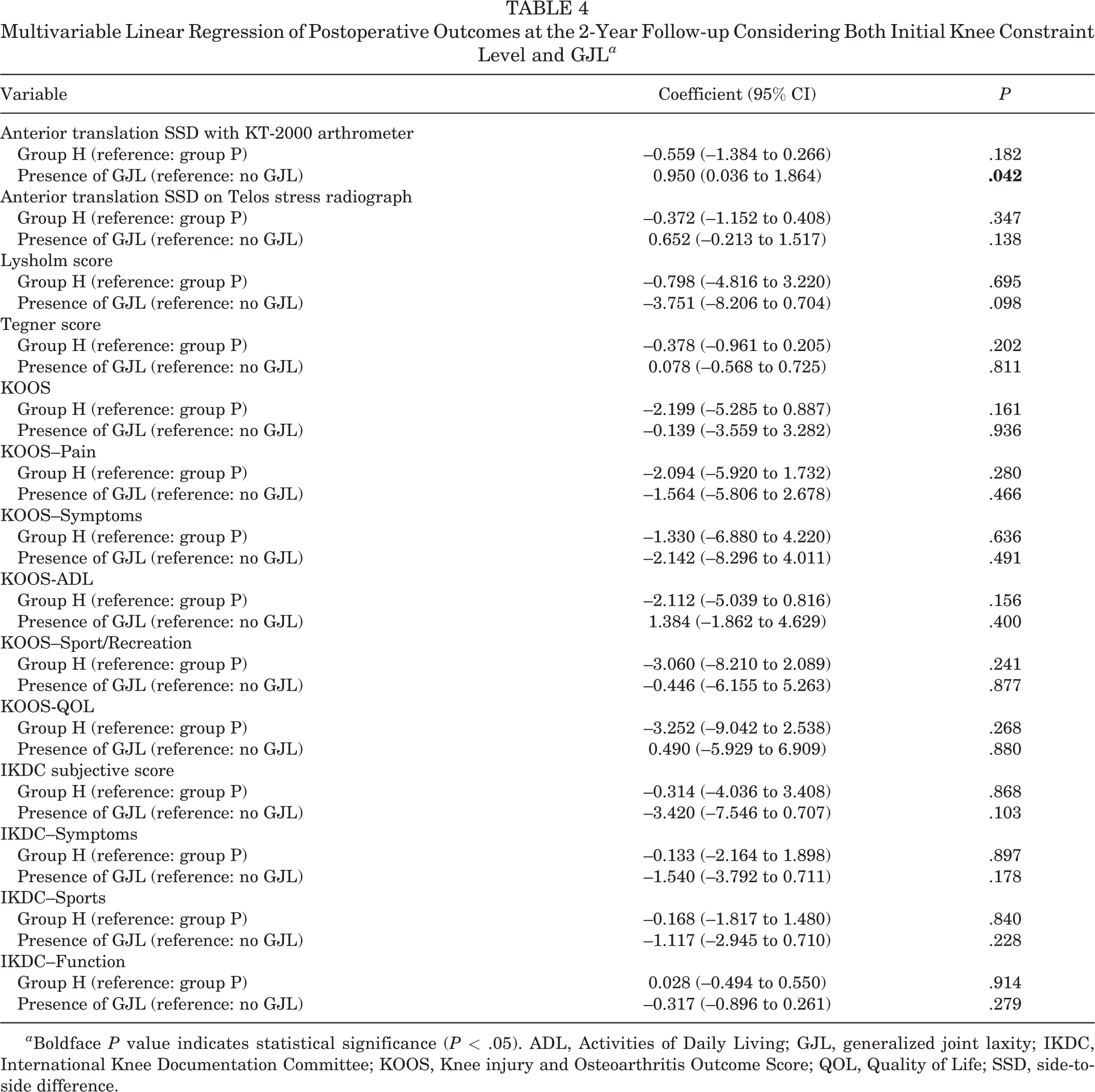
a Boldface P value indicates statistical significance (P < .05). ADL, Activities of Daily Living; GJL, generalized joint laxity; IKDC, International Knee Documentation Committee; KOOS, Knee injury and Osteoarthritis Outcome Score; QOL, Quality of Life; SSD, side-to-side difference.
During the 2-year follow-up, a similar number of patients underwent revision ACL reconstruction or contralateral ACL reconstruction in both groups (group P, n = 3; group H, n = 4) (Table 5). There were 2 subsequent brisement procedures for limited knee ROM in group H compared with none in group P (P = .171).
Comparison of Revision and Contralateral ACL Reconstruction and Subsequent Procedures Between the Study Groups a

a Data are reported as n (%). ACL, anterior cruciate ligament; ROM, range of motion.
Anterior translation measured in the contralateral knee with a KT-2000 arthrometer was the only independent predictor of high initial constraint in the reconstructed knee (Table 6). The cutoff value was found to be 8.4 mm (sensitivity, 63.0%; specificity, 74.2%; area under the curve, 0.741) (Figure 3).
Univariable and Multivariable Logistic Regression Analyses Showing Factors Influencing the Initial Constraint Level of the ACL-Reconstructed Knee a
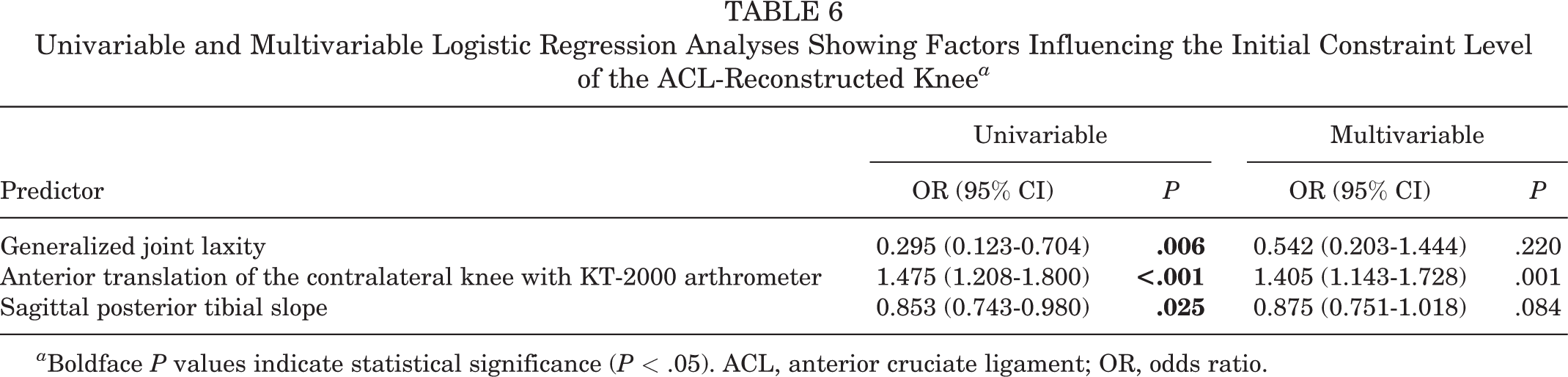
a Boldface P values indicate statistical significance (P < .05). ACL, anterior cruciate ligament; OR, odds ratio.

Receiver operating characteristic curve for determining the cutoff point for anterior translation in the contralateral knee (8.4 mm; sensitivity, 63.0%; specificity, 74.2%; area under the curve [AUC], 0.741).
Discussion
We found that the same amount of initial tension applied to the graft at graft fixation produced varying constraint levels in terms of the initial anterior translation SSD. A measured anterior translation in the contralateral knee >8.4 mm was found to be an indicator of postoperative high constraint in the affected knee. However, patients with a highly constrained knee (group H) did not experience better clinical outcomes after ACL reconstruction than those with a physiologically constrained knee (group P).
The optimal amount of initial tension for knee stability after ACL reconstruction remains unclear. However, it seems rational to consider that the tension needed to be applied to the graft is tissue-specific. While an initial tension of 20 to 60 N for a bone–patellar tendon–bone graft has been used for ACL reconstruction, higher tensions of approximately 70 to 80 N have been preferred for soft tissue grafts. 2,27 Yasuda et al 54 demonstrated that using an initial tension of 80 N for ACL reconstruction with a hamstring autograft provided more anterior-to-posterior knee stability than 20 N at the 2-year follow-up. In a comparison of 78.4, 117.6, and 147 N of initial tensions for semitendinosus tendon grafts, there were no reported differences in the anterior laxity or clinical outcomes. 23 A recent systematic review showed that an initial force of 78.5 to 90 N reduced the anterior laxity after ACL reconstruction. 26 Accordingly, and considering that highly tensioned grafts might produce unfavorable outcomes in terms of histology and stability, we applied 80 N of initial force to the grafts. 22,55 Our results also suggested that 80 N of initial force for an ACL reconstruction was favorable regarding the knee stability and clinical outcomes at short-term (2-year) follow-up.
Fleming et al 14,15 have conducted studies on laxity-based graft tensioning, either matching or overconstraining the graft by 2 mm compared with the anterior laxity of the contralateral knee. At 36, 60, and 84 months postoperatively, the authors found no significant differences between the matched and overconstrained groups in knee laxity and on most of the clinical outcomes. 1,15 More recently, a study on laxity-based graft tensioning reported that overconstrained hamstring autografts produced better outcomes than did matched-tensioned autografts, whereas no differences were found for patellar tendon grafts at 84 months. 10 Our finding of no difference in clinical outcomes between the physiologic constraint and high-constraint groups at 24 months was concordant with those of previous studies with short-term follow-up. However, the mean initial anterior translation SSD in the high-constraint group of our study was –4.1 ± 1.5 mm, which is more constrained than that of the overconstrained group in the study by Fleming et al 15 (–2.2 ± 0.2 mm). Consequently, we assume that the force used in the laxity-based protocol to overconstrain by 2 mm might be <80 N. This might imply that a higher tension than that used in the overconstrained graft in laxity-based tensioning could be employed. Future long-term studies are needed to draw a solid conclusion about the impact of the initial level of knee constraint after ACL reconstruction.
In both study groups, anterior translation SSD increased over time postoperatively, and the increase was significant at 6 months postoperatively, but not at 12 and 24 months. The changes in anterior translation SSD with time are similar to those found in previous studies. 1,15 Akelman et al 1 and Fleming et al 15 showed that anterior laxity for both the overtensioned and matched-tensioned groups increased over time, particularly over 6 months, although the anterior translation SSD at the 3-month follow-up was not stated. Nicholas et al 40 compared 45 and 90 N of initial tension for ACL reconstruction, using bone–patellar tendon–bone autografts, and showed that the graft loosened over the first 6 months, but the loosening was no longer statistically significant thereafter up to 4 years. Notably, most of the increase in the anterior laxity already appeared 1 week after surgery, although the immediate postoperative value was not reported.
One reason for the increased anterior laxity after ACL reconstruction is stress relaxation and the creep phenomenon. 17 Pretensioning on a graft board and/or cyclic preconditioning of knee flexion and extension are often performed to obviate graft elongation and tension loss. 11,13,41 We used pretensioning at 88 N for 20 minutes and 20 flexion-extension cycles of preconditioning. Graft elongation and the resultant increased anterior laxity are partly attributed to the viscoelastic behavior of the graft. However, the graft loosened significantly over 6 months, and its viscoelastic behavior alone may not account for this. Another possible reason is the graft ligamentization process after ACL reconstruction. In an animal study, the vascularity and cellularity of the graft approached those of the native ACL around 6 to 12 months after reconstruction. 4,49,52 Histological analysis after ACL reconstruction with hamstring autografts showed that the collagen content and cross-linking differed significantly from those of the native ACL at 6 months but became identical at 1 year postoperatively. 35 A recent quantitative magnetic resonance imaging study found that the proteoglycan content and collagen structure were significantly higher at 6 months than at 12, 24, and 36 months. 30 The time course of the ligamentization process showed similarities to our results, in which anterior laxity after ACL reconstruction increased significantly over 6 months and plateaued thereafter.
GJL adversely affects knee stability, graft failure rates, and functional outcomes after ACL reconstruction. 24,25,28 However, there has been a paucity of publications that describe the relationship between the presence of GJL and the initial constraint level of the knee. In the current study, the presence of GJL was significantly more common in the high-constraint group; however, it was not an independent predictor for the high constraint level of the knee. Furthermore, the clinical outcomes were comparable regardless of the knee constraint level, even considering GJL as a confounding factor. However, patients with GJL produced less-stable knees in terms of KT-2000 arthrometer anterior translation SSD than those without GJL at the 2-year follow-up (coefficient, 0.950; 95% CI, 0.036-1.864; P = .042). While there is a lack of consensus on the surgical strategy regarding GJL for ACL reconstruction, such as graft selection and graft tension, our results imply that knees with GJL could be initially overconstrained after ACL reconstruction using a soft tissue graft and may be one of the key adjustment factors in patients with GJL.
Limitations
The study had several limitations. First, information and selection bias were inevitable because of the retrospective nature of the study. Second, the sample size was relatively small, although a priori sample-size calculation was performed. Third, the short-term clinical outcomes might be insufficient to draw a clear conclusion regarding the effect of initial anterior translation SSD. Fourth, measurements using the KT-2000 arthrometer throughout the study were performed by a single senior surgeon. The measurements were consistent and reasonable because the intrarater reliability for the KT-2000 arthrometer measurement of anterior tibial translation was acceptable; however, the interrater reliability was poor. 44
Conclusion
Anterior translation >8.4 mm in the contralateral knee was an independent predictor of more constraint in the affected knee. The short-term clinical outcomes after ACL reconstruction were comparable, regardless of the initial level of constraint in terms of anterior translation SSD. In force-based tensioning, the measured anterior translation of the contralateral knee could be useful for forecasting the initial knee constraint level and adjusting for “individualized” constraints for ACL reconstruction.
Footnotes
Acknowledgment
The authors thank Seok-Jae Heo, PhD, for the statistical assistance.
Final revision submitted September 6, 2022; accepted October 21, 2022.
The authors declared that they have no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Yonsei University Gangnam Severance Hospital (reference No. 3-2021-0308).
Appendix
Comparison of Intraoperative Variables Between the Study Groups a

| Variable | Group P (n = 66) | Group H (n = 47) | P |
|---|---|---|---|
| Tunnel length, mm | 37.7 ± 3.9 | 37.3 ± 3.0 | .330 |
| Graft diameter, mm | 7.9 ± 0.7 | 8.1 ± 0.7 | .229 |
| Meniscal procedure | .811 | ||
| Yes | 38 (57.6) | 26 (55.3) | |
| No | 28 (42.4) | 21 (44.7) | |
| Medial meniscal procedures | .967 | ||
| None | 36 (54.5) | 25 (53.2) | |
| Partial meniscectomy | 9 (13.6) | 6 (12.8) | |
| Meniscal repair | 21 (31.8) | 16 (34.0) | |
| Lateral meniscal procedures | .912 | ||
| None | 49 (74.2) | 35 (74.5) | |
| Partial meniscectomy | 7 (10.6) | 4 (8.5) | |
| Meniscal repair | 10 (15.2) | 8 (17.0) | |
| Medial collateral ligament release | .640 | ||
| Yes | 3 (4.5) | 1 (2.1) | |
| No | 63 (95.5) | 46 (97.9) |
a Data are reported as mean ± SD or n (%).