
Abstract
Background:
Patients with femoroacetabular impingement syndrome (FAIS) show sex-specific differences in hip muscle function, hip morphology, and symptoms. Possible differences in hip muscle characteristics between men and women with FAIS are unknown.
Purpose:
To compare hip muscle cross-sectional area (CSA) and fatty infiltration between men and women with FAIS and investigate possible associations with patient-reported outcomes.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
We retrospectively analyzed preoperative axial pelvic magnetic resonance imaging scans of 104 patients (54 women) who underwent hip surgery for FAIS. The main outcome measures were side-to-side percentage asymmetry in hip muscle CSA and involved-side fatty infiltration as measured with the Goutallier scale for a total of 10 hip muscles. Patient-reported outcomes included duration of hip symptoms, iHOT-12 (12-item International Hip Outcome Tool), and Hip Sports Activity Scale.
Results:
Women showed larger hip abductor muscle CSA asymmetry than men (P = .018), particularly for the gluteus medius (P = .049), while men exhibited more fatty streaks (grade 1) in the gluteus medius (P = .015) than women. Duration of symptoms was associated only with fatty infiltration of obturator externus in men (r S = –0.55, P = .018). iHOT-12 was associated with CSA asymmetry of the gluteus minimus (r = –0.41, P = .011) and iliopsoas (r = –0.36, P = .028) in men and with piriformis fatty infiltration (r S = –0.56, P = .030) in women. The Hip Sports Activity Scale was associated with iliopsoas CSA asymmetry (r S = 0.32, P = .026) and with fatty infiltration of the tensor fasciae latae (r S = –0.45, P = .046) and obturator externus (r S = –0.50, P = .023) in women.
Conclusion:
Patients with FAIS demonstrated few sex-specific quantitative and qualitative alterations of hip muscles. Women showed greater hip abductor muscle atrophy than men, particularly for the gluteus medius, while men showed a higher degree of fatty infiltration in this same muscle. The duration of hip symptoms was not associated with muscle atrophy. Patient-reported hip pain/function and sport activity level were only moderately associated with isolated muscular variables.
Femoroacetabular impingement syndrome (FAIS) is a motion-related condition of the hip joint. It is caused by early contact between the proximal femur and acetabulum during hip flexion and rotations, and it results in hip pain and intra-articular lesions. 9,11 FAIS is frequently diagnosed in generally young and active individuals upon a triad of symptoms, clinical signs, and radiological features. 11 Notably, FAIS seems to be a risk factor for the early development of hip osteoarthritis (OA), 18 particularly in the presence of a structural alteration of the proximal femur (cam morphology), 1 while acetabular overcoverage/retroversion could be present (pincer morphology). 9 Patients with FAIS report hip pain and dysfunction during activities of daily living and sports. 11 Significant deficits of hip muscle strength (ie, muscle weakness) have also been observed, 8,16,21,26 especially for the hip adductors and flexors, 6 which may contribute to FAI-related functional limitations. Importantly, strength deficits were observed when patients with FAIS were compared with healthy controls 6,8,26 and when the involved hips of FAIS cases were compared with the contralateral hips (side-to-side asymmetry). 16 Hip muscle weakness in FAIS could be explained by neural and/or muscular factors. The former typically result in suboptimal or improper activation of agonist muscles (activation failure) 6 and/or antagonist or synergistic muscles (co-contraction), while the latter mainly include quantitative (muscle atrophy) and qualitative (eg, intramuscular fatty infiltration) 20 alterations occurring within the muscle.
Recent findings indicate that patients with FAIS present signs of hip muscle atrophy. For instance, Malloy et al 22 quantified the cross-sectional area (CSA) bilaterally for 17 hip and thigh muscles in 50 patients with unilateral FAIS (64% of women). They found a significantly smaller CSA on the involved side for 3 muscles (gluteus maximus, gluteus minimus, and rectus femoris), which shows the presence of muscle atrophy, but they did not account for sex as a potential effect modifier. Indeed, previous research has demonstrated sex-specific differences for hip flexor and extensor muscle strength in patients with FAIS, with women showing greater strength deficits (asymmetries) than men. 16,21 In addition, sex-related differences in hip symptoms, hip morphology, and hip/pelvic kinematics during gait were observed in patients with FAIS, which potentially influence hip muscle function. Specifically, women had more pronounced hip symptoms 26 and less severe cam morphology than men, 13 while unilateral vs bilateral FAIS-related hip alterations in gait kinematics were observed in women and men, respectively. 19 We recently identified some interesting associations between hip abductor strength asymmetry and patient-reported hip symptoms and dysfunction in women with FAIS, whereas in men, hip flexor strength asymmetry was correlated to the severity of the underlying cam morphology. 21
To better understand some of the factors underlying these sex-specific differences in hip muscle strength as well as hip symptoms and function, it appears legitimate to investigate quantitative and qualitative properties of the main hip muscles in male vs female patients with FAIS. 7 Hence, the main aims of this study were to compare hip muscle CSA asymmetries (primary outcome) and fatty infiltration (secondary outcome) between men and women with FAIS. It was hypothesized that women would show greater muscle atrophy and fatty infiltration than men. Additionally, we investigated potential sex-specific associations between hip muscle properties and patient-reported outcomes (tertiary outcomes).
Methods
Study Design
A series of patients who had a diagnosis of FAIS and were scheduled for hip surgery at our institution was retrospectively evaluated. Initially, a total sample size of 100 patients (50 women and 50 men) was defined a priori with a power analysis (G*Power 3.1). 15 We estimated an effect size of 0.77 based on previously reported gluteus maximus CSA asymmetry in men 3 and women 30 with hip OA. Considering an alpha level of 0.05, a power of 0.95 (1 – β), and a 2-tailed t test, the calculation indicated that a total sample size of 90—rounded to 100 (50 in each group)—was required for detecting a significant difference in hip CSA asymmetry between women and men with FAIS. The study was conducted in accordance with the Declaration of Helsinki ethical principles for medical research involving human subjects. The study protocol received institutional review board approval, and all participants provided informed consent.
Patients
The inclusion criteria were as follows: (1) diagnosis of FAIS based on symptoms (eg, hip pain, clicking, catching, stiffness), clinical signs (eg, limited range of motion, positive impingement test), and imaging findings (cam or pincer morphology on plain radiographs) by a hip surgeon from our institution 11 ; (2) age between 16 and 55 years; (3) unilateral hip surgery for FAIS between January 2014 and December 2019; (4) availability of preoperative axial plane pelvic magnetic resonance imaging (MRI) in the imaging database of our institution; and (5) availability of preoperative 12-item International Hip Outcome Tool (iHOT-12) score in the FAIS outcome registry of our institution. Exclusion criteria were previous hip surgery of the involved and contralateral hips and contralateral hip surgery in the 12 months after surgery of the involved hip. Because FAIS may present bilaterally 2 and in this study the contralateral hip was treated as a healthy control hip for calculating side-to-side asymmetries, it was important to rule out patients with problems affecting the contralateral hip.
Assessment of Muscle CSA and Fatty Infiltration
Measurements of muscle CSA and fatty infiltration were conducted upon a standardized protocol on axial-plane single-slice MRI scans for a total of 10 hip muscles. All measurements were performed by the first author, a physical therapist with 6 years of experience, under the supervision of a radiologist (head physician). Skewed MRI slices were systematically excluded by visual inspection. Three anatomic landmarks were used to define the axial plane on the MRI sequence where the measures were executed: anterior inferior iliac spine (gluteus maximus, gluteus minimus, gluteus medius, piriformis, iliopsoas) (Figure 1A), center of the femoral head (tensor fascia latae, sartorius) (Figure 1B), and inferior border of the greater trochanter eminence (obturator externus, pectineus, quadratus femoris) (Figure 1C). The allocation of the evaluated muscle to 1 of the 3 landmarks was based on previous studies 24,33,34 as well as on anatomic and feasibility considerations.

Axial pelvic magnetic resonance imaging of a representative woman with femoroacetabular impingement syndrome at the anatomic landmark levels of the (A) anterior inferior iliac spine (GMax, gluteus maximus; GMed, gluteus medius; GMin, gluteus minimus; IL, iliopsoas; Piri, piriformis), (B) center of the femoral head (S, sartorius; TFL, tensor fasciae latae), and (C) inferior border of the greater trochanter eminence (OE, obturator externus; P, pectineus; QF, quadratus femoris).
Muscle CSA was measured bilaterally using HOROS software (version 3.3.5; Nimble Co) with a dedicated tablet and pen (Wacom Cintiq Tablet; Wacom). The software allowed manual tracing of the muscle boundary and calculation of muscle CSA using the region-of-interest tool. All CSA measurements were conducted using a standardized procedure to minimize bias, starting with the left side and from proximal to distal. Muscle atrophy was quantified as the side-to-side percentage asymmetry (hereafter, CSA asymmetry) in single-muscle CSA, calculated as follows: (uninvolved hip – involved hip)/uninvolved hip × 100. For CSA asymmetry, the 10 muscles were also semiarbitrarily grouped according to their primary or secondary function 36 : hip flexors (iliopsoas, tensor fasciae latae, sartorius), hip extensors (gluteus maximus), hip abductors (gluteus medius and minimus), hip adductors (pectineus), and hip external rotators (piriformis, obturator externus, and quadratus femoris). The absolute CSA of each muscle contributing to a given function (eg, gluteus medius and minimus for hip abduction) was summed to provide a total absolute CSA by side. The CSA asymmetry formula was then applied on these data to respect the contribution of single hip muscles with different CSAs within a functional group.
Hip muscle fatty infiltration was evaluated on T1-weighted MRI scans of the involved hip, which were available for ∼40% of the patients. We used the Goutallier classification system, which is a 5-level scale that rates the grade of intramuscular fat content as follows (Figure 2): grade 0, no fatty infiltration; grade 1, some fatty streaks; grade 2, more muscle than fat; grade 3, equal amount of muscle and fat; grade 4, more fatty infiltration than muscle. 10

Representative magnetic resonance imaging scans of 3 patients with different degrees of fatty infiltration for gluteus minimus (GMin) and gluteus medius (GMed) muscles based on the Goutallier classification system. (A) GMin, grade 0; GMed, grade 0. (B) GMin, grade 1; GMed, grade 0. (C) GMin, grade 2; GMed, grade 1.
Patient-Reported Outcomes
We evaluated 3 patient-reported outcome measures. The first was the iHOT-12 German version, which is a validated short version of the 33-item iHOT. 12 This questionnaire was designed to assess hip symptoms and functional limitations, sports and recreational activities, and job-related concerns as well as aspects of the social, emotional, and lifestyle domain in young and active patients with hip disorders. 12 The score ranges from 0 to 100, with 100 indicating the best quality-of-life score. 12 The second outcome measure was the Hip Sports Activity Scale (HSAS), a validated tool to quantify the sports activity level of patients with FAIS. 25 The HSAS is a 9-level scale ranging from 0 to 8, where 8 represents competitive sport at the elite level. 25 The third outcome measure was the duration of symptoms in months, as obtained from a single standardized question. 5 Medication intake was retrieved from the database of our institution as a part of a preoperative health history patient questionnaire.
Statistical Analyses
Data were tested for normality using Kolmogorov-Smirnov tests. Descriptive statistics were calculated for general patient characteristics, hip muscle CSA, hip muscle fatty infiltration, and patient-reported outcomes. Continuous data were presented as mean and standard deviation (ratio or interval data) or median and percentile (ordinal data), whereas categorical data were presented as numbers and prevalence. Differences between women and men in general characteristics and patient-reported outcomes were evaluated using unpaired 2-tailed t tests (ratio or interval data) or Mann-Whitney U tests (ordinal data). Differences between involved and uninvolved hip muscle CSA were evaluated using paired 1-tailed t tests. Differences between women and men in hip muscle CSA asymmetry and fatty infiltration were evaluated using unpaired 1-tailed t tests (ratio or interval data) or Mann-Whitney U tests (ordinal data). Effect sizes for sex-related differences in CSA asymmetries were calculated with Cohen d. Associations between hip muscle CSA asymmetry and patient-reported outcomes were tested using Pearson (ratio or interval data; r) or Spearman (ordinal data; r S) correlation coefficients, whereas Spearman correlation coefficients were used for hip muscle fatty infiltration vs patient-reported outcomes. Intrarater test-retest reliability of hip muscle CSA and fatty infiltration measures was assessed twice by the same rater in a sample of 20 patients (10 women and 10 men), with an interval of 2 weeks between the assessments. Reliability of hip muscle CSA was evaluated using standard errors of measurement and intraclass correlation coefficients (3,1). Reliability of hip muscle fatty infiltration was evaluated using percentage agreement and Cohen weighted kappa coefficients. Missing data were not replaced, and only complete data pairs were analyzed. Statistical analyses were conducted with SPSS Statistics Version 26.0 (IBM). P values <.05 were considered significant.
Results
General Characteristics and Patient-Reported Outcomes
A total of 104 patients (54 women and 50 men) were included in this study. The women and men were similar in age (P = .801), although women had a significantly lower body mass index than men (P < .001) (Table 1). The iHOT-12 score was significantly lower in women than men (P = .037). No significant sex-specific differences were observed for HSAS score (P = .160), duration of symptoms (P = .609), medication intake (P = .068), and interval between MRI scan and surgery (P = .569).
General Characteristics and Patient-Reported Outcomes by Sex a
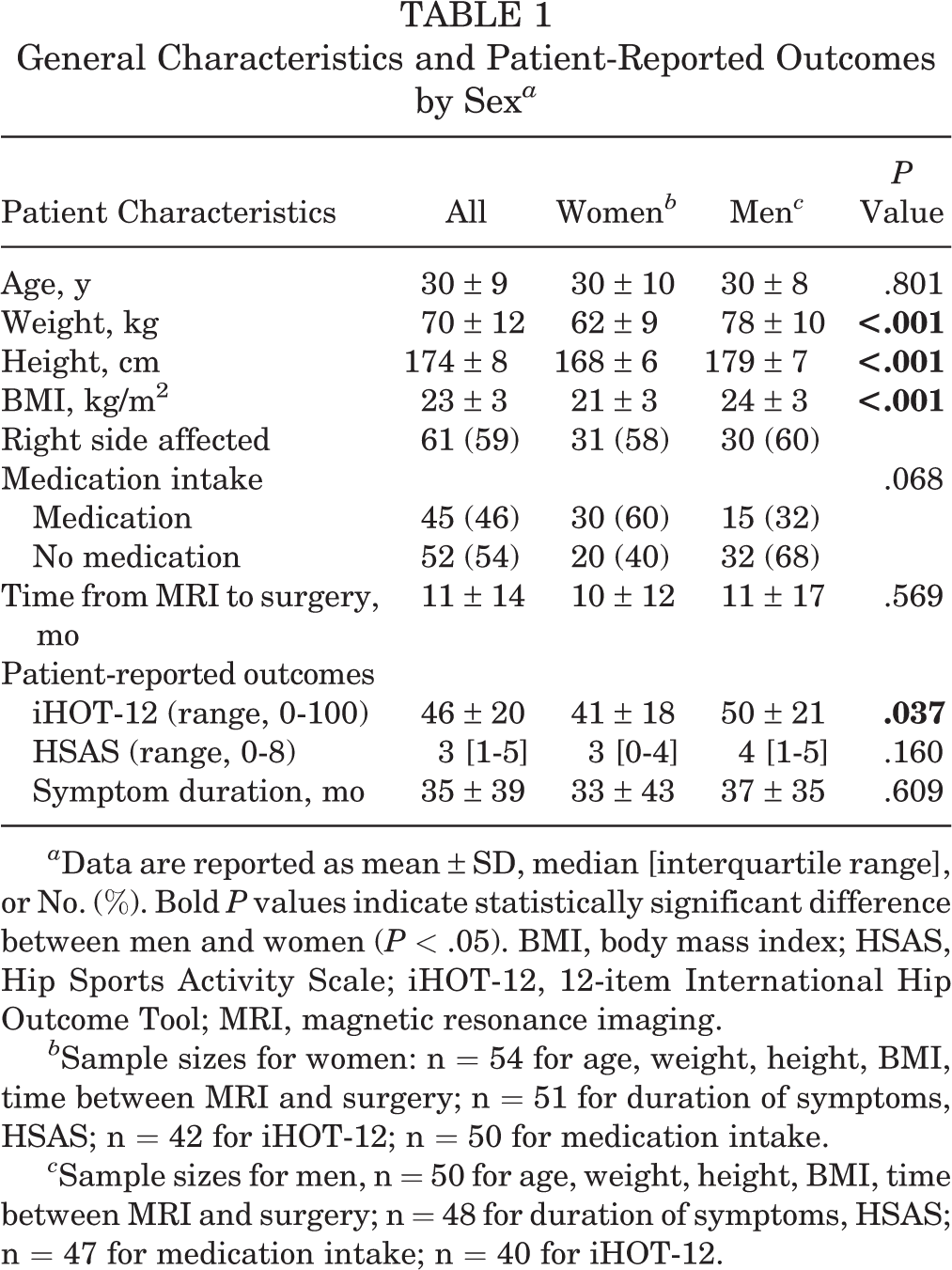
a Data are reported as mean ± SD, median [interquartile range], or No. (%). Bold P values indicate statistically significant difference between men and women (P < .05). BMI, body mass index; HSAS, Hip Sports Activity Scale; iHOT-12, 12-item International Hip Outcome Tool; MRI, magnetic resonance imaging.
b Sample sizes for women: n = 54 for age, weight, height, BMI, time between MRI and surgery; n = 51 for duration of symptoms, HSAS; n = 42 for iHOT-12; n = 50 for medication intake.
c Sample sizes for men, n = 50 for age, weight, height, BMI, time between MRI and surgery; n = 48 for duration of symptoms, HSAS; n = 47 for medication intake; n = 40 for iHOT-12.
Intrarater Test-Retest Reliability
All intraclass correlation coefficients for hip muscle CSA measures ranged from 0.77 to 0.99 for the involved hip, except for the obturator externus (range, 0.60-0.92), and from 0.74 to 0.99 for the uninvolved hip. Standard errors of measurement ranged from 0.08 to 2.08 cm2 for the involved hip and from 0.16 to 1.59 cm2 for the uninvolved hip. The Cohen weighted kappa coefficients for fatty infiltration ranged from 0.62 to 1.00 for the involved hip and from 0.61 to 1.00 for the uninvolved hip, except for piriformis (0.23), with a percentage agreement ranging from 85% to 100% and from 80% to 100%, respectively.
Muscle CSA
The sample size for muscle CSA differed from muscle to muscle (n = 51-53 for women and n = 46-50 for men), as certain muscles could not be entirely measured. The main reasons were the lack of MRI slices at a specific anatomic landmark and low qualitative images/slices with no detectable muscle boundary. Women showed a smaller CSA on the involved side vs the uninvolved side for 3 muscles: gluteus medius (P = .022), gluteus minimus (P = .035), and piriformis (P = .020) (Table 2). No other significant differences in muscle CSA were observed between the involved and uninvolved hips.
Hip Muscle CSA by Muscle, Side, and Sex a
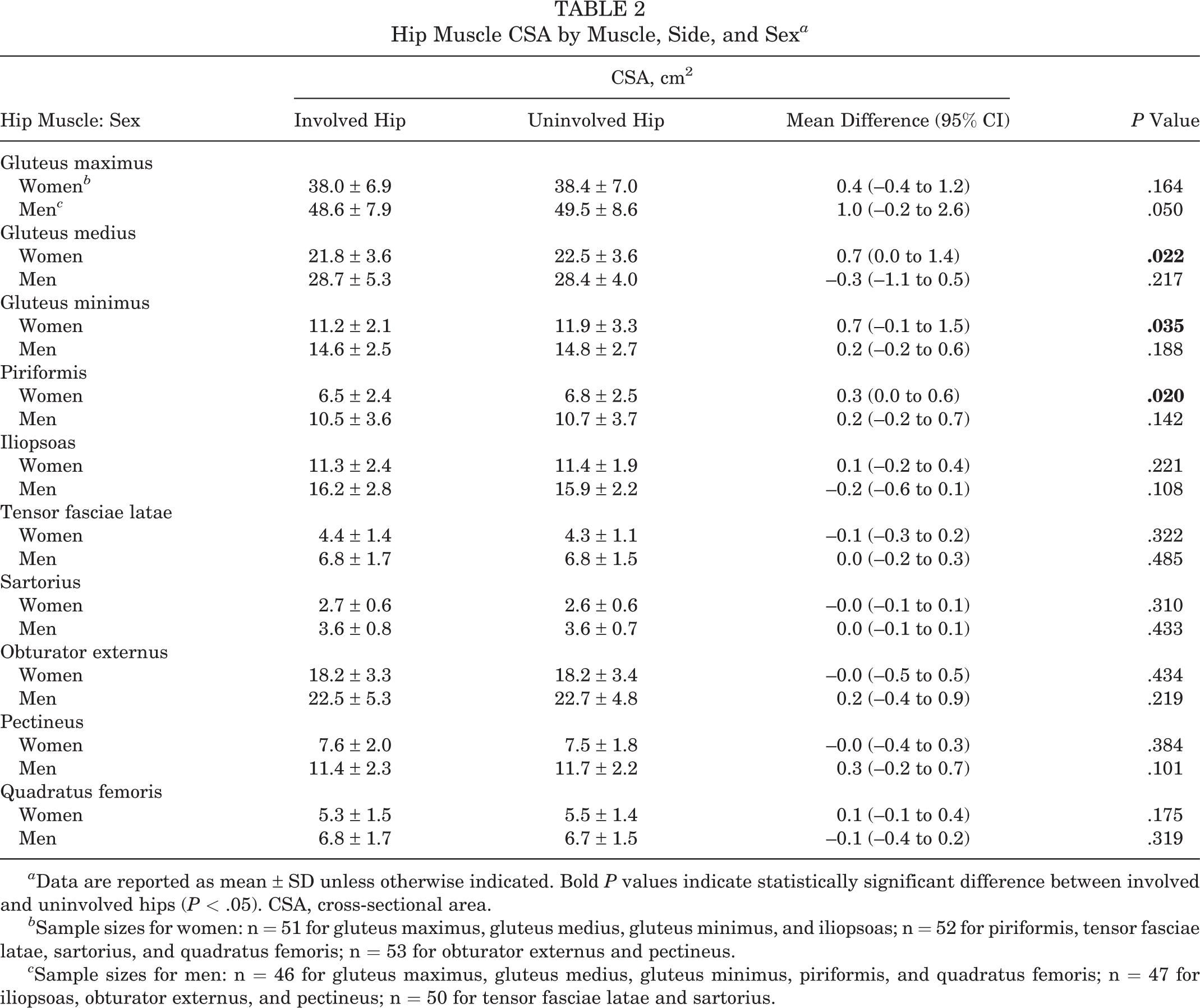
a Data are reported as mean ± SD unless otherwise indicated. Bold P values indicate statistically significant difference between involved and uninvolved hips (P < .05). CSA, cross-sectional area.
b Sample sizes for women: n = 51 for gluteus maximus, gluteus medius, gluteus minimus, and iliopsoas; n = 52 for piriformis, tensor fasciae latae, sartorius, and quadratus femoris; n = 53 for obturator externus and pectineus.
c Sample sizes for men: n = 46 for gluteus maximus, gluteus medius, gluteus minimus, piriformis, and quadratus femoris; n = 47 for iliopsoas, obturator externus, and pectineus; n = 50 for tensor fasciae latae and sartorius.
Gluteus medius CSA asymmetry was significantly larger in women than men (P = .049), with a small effect size (Table 3). For all other muscles, no sex-specific difference was observed for CSA asymmetries. This was true also when considering hip muscles grouped by function, as women showed larger CSA asymmetry for hip abductors than men (P = .018), while no sex-related differences were observed for the other muscle groups.
Hip Muscle CSA Asymmetries by Sex and Muscle/Muscle Group a

a Positive percentages (asymmetries) indicate a smaller CSA on the involved side when compared with the uninvolved side. Bold P values indicate statistically significant difference between men and women (P < .05). CSA, cross-sectional area; ES, effect size (calculated as Cohen d).
b Hip extensors: gluteus maximus. Hip abductors: gluteus medius and minimus. Hip external rotators: piriformis, obturator externus, and quadratus femoris. Hip adductors: pectineus.
c Sample sizes for women: n = 51 for gluteus maximus, gluteus medius, gluteus minimus, iliopsoas, hip extensors, and hip abductors; n = 52 for piriformis, tensor fasciae latae, sartorius, quadratus femoris, and hip flexors; n = 53 for obturator externus, pectineus, hip adductors, and hip external rotators.
d Sample sizes for men: n = 46 for gluteus maximus, gluteus medius, gluteus minimus, piriformis, quadratus femoris, hip extensors, and hip abductors; n = 47 for iliopsoas, obturator externus, pectineus, and adductors; n = 48 for hip external rotators; n = 50 for tensor fasciae latae, sartorius, and hip flexors.
Fatty Infiltration
The total sample size for fatty infiltration was 42 or 43 patients (n = 22 for women and n = 20-21 for men), as only a small proportion (41%) of the MRI scans were T1 weighted. Men showed a significantly higher degree of fatty infiltration in the gluteus medius muscle than women (P = .015) (Table 4). For all other muscles, no sex-specific differences in fatty infiltration were observed.
Hip Muscle Fatty Infiltration (Goutallier Grade) by Muscle and Sex a

a Data are reported as No. (%). Bold P value indicates statistically significant difference between men and women (P < .05).
b Sample size for women: n = 22.
c Sample sizes for men: n = 20 for gluteus maximus, gluteus medius, gluteus minimus, piriformis, and iliopsoas; n = 21 for tensor fasciae latae, sartorius, obturator externus, pectineus, and quadratus femoris.
Association of CSA Asymmetry and Fatty Infiltration With Patient-Reported Outcomes
No significant correlations were found between hip muscle CSA asymmetry and duration of hip symptoms. The iHOT-12 score was significantly correlated to the CSA asymmetry of the gluteus minimus (r = –0.407, P = .011) and iliopsoas (r = –0.356, P = .028) muscles in men but not women, with men with higher pain and dysfunction showing greater muscle atrophy. The HSAS score was positively correlated with iliopsoas CSA asymmetry (r S = 0.321, P = .026) in women but not men. No other significant correlations were observed.
Fatty infiltration of the obturator externus was negatively associated with the duration of hip symptoms (r S = –0.552, P = .018) in men but not women. The iHOT-12 score was significantly correlated to piriformis fatty infiltration (r S = –0.560, P = .030) in women but not men, with women with higher pain and dysfunction showing greater fatty infiltration. The HSAS score was significantly correlated to fatty infiltration of the tensor fasciae latae (r S = –0.450, P = .046) and obturator externus (r S = –0.504, P = .023) muscles in women but not men, with women with lower levels of sport activity showing greater fatty infiltration. No other significant correlations were observed.
Discussion
The aims of the current study were to examine sex-specific differences in hip muscle CSA asymmetry and fatty infiltration in patients with FAIS and possible associations with patient-reported outcomes. The main findings were that women with FAIS had greater gluteus medius muscle atrophy than men, while men had a higher degree of fatty infiltration in the same muscle. Another key finding was the greater hip abductor muscle atrophy in women, when considering muscles grouped by function. No significant sex-specific differences were observed for the other hip muscles. Interestingly, the duration of hip symptoms did not correlate with muscle atrophy, just with fatty infiltration of the obturator externus muscle in men. Patient-reported hip pain/function and sport activity level were only moderately associated with isolated muscular variables.
Women showed significantly smaller CSA on the involved vs uninvolved side for the gluteus medius, gluteus minimus, and piriformis muscles. These results are in line with the findings of Malloy et al, 22 who were the first to show the presence of atrophy in some hip muscles of patients with FAIS. They found a significantly smaller CSA for the gluteus maximus, gluteus minimus, and rectus femoris muscles on the symptomatic side as compared with the asymptomatic one, although they did not account for sex as a potential confounding factor. In the current study, we preferred to exclude the rectus femoris from the analyses because its CSA was measured at the level of the center of the femoral head (vs the inferior border of the acetabulum in Malloy et al), which resulted in extremely small CSAs. Interestingly, Malloy et al did not find any side-to-side difference for gluteus medius muscle CSA, an extremely important muscle for frontal-plane hip and pelvic stability during walking. 36 A possible explanation for this might be that sex-specific differences for gluteus medius CSA asymmetry, as found in the current study, could have masked significant muscle atrophy. However, the sample size in the study of Malloy et al was relatively small (n = 50) with an imbalanced sex distribution (64% of women), which could have invalidated the comparison between men and women. The lack of gluteus medius CSA asymmetry was already reported by Mendis et al 24 in patients with acetabular labral joint pathology. Nevertheless, they highlighted the presence of gluteus medius atrophy in their patients as compared with a healthy control group, thereby indicating possible bilateral involvement of the gluteus medius muscle. This was explained by the possible influence of altered hip and pelvic biomechanics on hip muscle size, even if these results were obtained from a relatively small sample of 12 patients and 12 healthy controls. Lewis et al 19 demonstrated that FAIS-related hip kinematic alterations occurred unilaterally in women vs bilaterally in men. A speculative interpretation is that our male patients could have shown bilateral gluteus medius atrophy and/or fatty infiltration, but this was not verified in our study as muscle CSA was not evaluated in healthy controls and fatty infiltration was quantified only on the involved side.
Surprisingly, Mastenbrook et al 23 found larger gluteal muscle volume in women with chronic hip pain as compared with healthy controls, despite lower hip abductor strength. One possible explanation that they proposed was increased noncontractile tissue in the muscle (eg, intramuscular fat), which resulted in the overestimation of the real amount of muscle mass. A similar interpretation could be proposed to explain the lack of gluteus medius CSA asymmetry for the male patients whom we tested (contrary to women), in the presence of greater fatty infiltration with respect to their female counterparts. We cannot give a plausible explanation for men having more intramuscular fat than women, except for the significantly higher body mass index of the former 27 (mean ± SD, 25 ± 3 vs 22 ± 3 kg/m2; P = .001), which is suggestive of a greater proportion of overweight men than women. However, no correlation was found between body mass index and gluteus medius fatty infiltration in our patients. It is important to bear in mind that the sample size for fatty infiltration analyses was relatively small (n = 42), as only T1-weighted MRI scans were considered. Moreover, despite its ease of use, the Goutallier classification system is highly subjective and has low reliability. 32 These findings therefore need to be interpreted with caution.
Previous studies have demonstrated some differences in hip muscle strength between women and men with FAIS. 16,21 Maffiuletti et al 21 observed larger hip flexor strength asymmetry in women, which cannot be explained by the hip flexor muscle CSA results from the current study (no significant CSA asymmetry in women and no sex-specific differences for hip flexors). As mentioned, we did not consider the rectus femoris muscle; consequently, hip flexor muscles were not completely represented. The lack of hip flexor muscle atrophy that we observed could have been influenced by this choice. The patients tested by Maffiuletti et al were younger than our patients (18-35 years) and had no urgent indication for hip surgery. Accordingly, we assumed that our patients, who were older and had a more advanced stage of FAIS, would have displayed more pronounced changes in hip muscle characteristics. In fact Zacharias et al 35 reported greater alterations of muscle volume and fatty infiltration of the glutei muscles in patients with more advanced hip OA. However, no association between the stage of the pathology and the extent of muscle atrophy in patients with hip OA was found in a recent systematic review. 17
We expected smaller asymmetries in hip muscle CSA than those previously reported for hip muscle strength. Indeed, Arokoski et al 3 assessed hip muscle strength and CSA in men with hip OA and observed smaller impairments in muscle CSA (6%-13%) than in muscle strength (13%-22%) when comparing the involved and contralateral hips. Kierkegaard et al 16 evaluated involved and contralateral hip strength in 60 patients with FAIS (64% women) scheduled for hip surgery and showed larger strength asymmetries in women for hip flexors and extensors. In contrast to these findings, we did not find any significant sex-specific difference in hip extensor muscle CSA and fatty infiltration.
Previous studies have demonstrated that women with FAIS are more likely to have worse symptoms and greater functional limitations than men. 14,26 Consistent with the literature, in our study, women had lower iHOT-12 scores than men (41 ± 18 vs 50 ± 21), indicating higher hip pain and dysfunction. Contrary to the expectations, however, women did not show any significant associations between muscle CSA asymmetries and hip pain/function, only between iliopsoas CSA asymmetry and sport activity level. Yet, men showed a significant association between muscle CSA asymmetries and hip pain/function for the gluteus minimus and iliopsoas muscles. In agreement with the findings of Malloy et al, 22 we did not find any significant association between the duration of hip symptoms and muscle CSA asymmetries, just with obturator externus fatty infiltration in men. Furthermore, fatty infiltration was negatively associated to iHOT-12 for the piriformis muscle and to HSAS for tensor fasciae latae and obturator externus muscles in women. Contrary to these results, Malloy et al presented positive correlations between preoperative pain level and pectineus, tensor fasciae latae, obturator externus, and adductor longus muscle CSA, therefore indicating a possible link between hip muscle mass and pain. Although self-reported hip pain and function were found to correlate with strength asymmetries in women with FAIS, 21 it was not the case for CSA and fatty infiltration in the current study. We hypothesize that muscle strength is more likely to be associated with patient-reported outcomes than muscle morphologic variables, likely because of the influence of pain-related activation failure on functional outcomes.
This well-powered study provided an overview of the differences in quantitative and qualitative hip muscle characteristics between women and men with FAIS. Early identification of possible muscular alterations is clinically important to address eventual deficits with tailored treatment options. This study showed that the extent of muscle atrophy and intramuscular fatty infiltration was specific for isolated hip muscles and differed by sex. The growing relevance of nonsurgical treatment options for FAIS stresses the importance of exercise therapy with a particular focus on hip-strengthening exercises. 4 Since women showed more pronounced hip abductor muscle atrophy than men, particularly for the gluteus medius muscle, we suggest implementing specific strengthening exercises targeting these muscles in female patients with FAIS. This possibly has positive implications on hip dynamic stability and functional task performance. Nevertheless, whether hip muscle weakness or atrophy in patients with FAIS is a causative factor or a consequence of FAI-related symptoms and movement impairments (eg, adaptive gait strategies) is unclear and deserves further investigation.
Limitations
This study has some limitations that need to be acknowledged. The main limitation is its retrospective design, which implies that MRI scans were performed in different hospitals and that no other concomitant measures of hip muscle function were conducted (eg, muscle strength with dynamometry or muscle activity with electromyography). Another limitation is that muscle CSA and fatty infiltration were assessed using only a single MRI slice. Indeed, muscle CSA is just an estimate of the total muscle size. Mean CSA measures on consecutive MRI slices over the whole muscle length or volumetric muscle analysis is recommended for future studies, 28 also to adjust for possible skewness of the axial MRI slices. The multicenter origin of the MRI scans did not allow this procedure to be conducted in the current study. In the same way, it is known that intramuscular fat content varies within the muscle, 29,31 which emphasizes the importance of finding standardized anatomic landmarks or considering the whole muscle length. Therefore, as a result of the intrinsic limitations of the Goutallier classification system discussed earlier and the lack of bilateral assessments, our fatty infiltration results should be interpreted with extreme caution. Last, measurements were performed by only 1 assessor and could not be completely blinded to patient demographics and the involved side, as some MRI scans had contrast agents in the hip joint.
Conclusion
Patients with FAIS presented some sex-specific quantitative and qualitative alterations of the main hip muscles. Women showed larger side-to-side asymmetry in gluteus medius CSA, while men exhibited more fatty streaks in this muscle. Women showed greater muscle atrophy for the hip abductor muscle group. In neither women nor men was the duration of hip symptoms associated with muscle CSA asymmetries. Patient-reported hip pain and function as well as sport activity level were only moderately associated with isolated muscular variables, with no sex-specific differences.
Footnotes
Final revision submitted September 22, 2022; accepted October 11, 2022
The authors have declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the ethics commission of the canton of Zurich (No. 2020-00662).