
Abstract
Background:
Glenohumeral instability represents a common cause of shoulder pain and disability among active-duty members of the military and is associated with the development of glenoid osteochondral defects.
Purpose:
To report clinical outcomes and survivorship after combined microfracture of isolated chondral lesions of the glenoid and labral repair among young, active-duty military patients and to compare outcomes with those of patients who underwent isolated shoulder stabilization.
Study Design:
Cohort study; Level of evidence, 3.
Methods:
Included were 31 active-duty military patients aged <40 years who underwent simultaneous microfracture of chondral lesions of the glenoid and labral repair for shoulder instability between January 2011 and January 2017 (microfracture group) and 209 patients without chondral defects who underwent shoulder stabilization during the same time period (instability group). Preoperative and 5-year postoperative outcomes (range of motion [ROM], visual analog scale [VAS] for pain, Single Assessment Numeric Evaluation [SANE] score, American Shoulder and Elbow Surgeons [ASES] shoulder score, and Rowe instability score) were compared within and between groups, and separate subgroup analyses were performed to determine whether variant of instability and dominant-shoulder involvement were associated with worse outcomes.
Results:
The mean follow-up was significantly longer for the microfracture group versus the instability group (95.58 ± 23.12 vs 83.38 ± 25.93 months; P = .014). Age and sex distributions were similar between groups. In both groups, there was significant pre- to postoperative improvement on all outcomes scores (P = .0001 for all). When compared with the instability cohort, microfracture patients had significantly worse postoperative VAS pain (2.65 ± 1.78 vs 1.55 ± 1.92; P = .003), SANE (79.13 ± 14.43 vs 91.23 ± 13.20; P < .0001), and ASES (79.90 ± 13.87 vs 89.03 ± 14.28; P = .001) scores, as well as decreased ROM in forward flexion (151.29° ± 11.76° vs 155.48° ± 10.3°; P = .039) and external rotation (63.65° ± 8.34° vs 65.17° ± 0.64°; P = .010). At latest follow-up, 58% of microfracture patients had returned to active-duty military service compared with 93.78% of isolated instability patients (P < .0001).
Conclusion:
Combined microfracture and arthroscopic labral repair produced modest, albeit statistically significant, improvements in patient-reported outcome measures and may be a reasonable treatment option for patients with chondral lesions who are not candidates for arthroplasty. However, microfracture patients had significantly worse outcomes than patients who underwent stabilization without concomitant chondral defects.
Members of the military experience a markedly higher incidence of shoulder pain and dysfunction when compared with civilian populations. Glenohumeral instability, in particular, represents a common cause of disability among active-duty servicemembers, with rates of shoulder dislocation reported to be 10 times higher than in the general public. 5,10,13,23,26,34,35 While anterior instability is the most common subtype observed, military patients are also at significantly greater risk for posterior and combined-type instability when compared with their civilian counterparts. 3,26,32,36 Arthroscopic labral repair has long been considered to be first line for operative management of patients with anterior shoulder instability. 1,24,34 In addition, recent data have shown promising outcomes with high rates of return to preinjury levels of activity in patients with combined-type and posterior instability following arthroscopic stabilization procedures. 9,26,36
Articular cartilage defects are typically found in patients with a history of recurrent instability or shoulder trauma. 8,16,28 Although the exact incidence of glenohumeral chondral lesions is unknown, they are not an uncommon finding during diagnostic arthroscopy. 8,16 However, management of symptomatic chondral lesions in young, active patients remains challenging. Shoulder arthroplasty is the gold standard for the surgical management of painful degenerative changes in older populations; however, it is associated with high rates of persistent limitation and subsequent discharge from active-duty service in young military patients. 19 Currently, microfracture is the most evidence-based modality for the operative management of young patients with isolated glenoid chondral lesions. 8,16,28 Multiple studies have reported promising short-term outcome data, although longer-term studies have demonstrated higher risk of reoperation and failure. 12,21,25,33 Other therapeutic options, however, such as cartilage transplantation or autologous chondrocyte implantation, currently lack sufficient evidence to support their use for the management of glenoid lesions. 16,28
The purpose of this study was to report clinical outcomes and survivorship following combined microfracture of isolated chondral lesions of the glenoid and labral repair among active-duty military patients <40 years of age. In addition, we sought to compare outcomes with patients who underwent shoulder stabilization surgery alone during the same time period. We hypothesized that combined glenoid microfracture and labral repair would produce significant improvements in patient-reported outcome measures (PROMs) at latest follow-up, however, with inferior outcomes when compared with primary labral repair in patients without concomitant chondral defects.
Methods
This study was a retrospective analysis of prospectively collected data comparing active-duty military patients <40 years old who underwent simultaneous microfracture of isolated chondral lesions of the glenoid and labral repair between January 2011 and January 2017 with those who underwent labral repair alone during the same time period. Institutional review board approval was obtained for the study protocol, and informed consent was obtained from all included patients after study procedures were explained.
Patient Population
Included were active-duty military patients <40 years old who underwent labral repair with minimum 5-year follow-up, defined as having complete pre- and postoperative outcome scores at latest follow-up. 22 Excluded were patients ≥40 years old, those with a history of previous shoulder surgery, those who underwent concomitant rotator cuff repair at the time of surgery, and those with concomitant humeral head osteochondral defects.
All patients had symptoms recalcitrant to nonoperative management including physical therapy, nonsteroidal anti-inflammatory drugs, limited-duty profiling, and home exercise programs before being considered for surgery. In addition, all patients had reported subjective glenohumeral joint instability and had positive anterior and/or posterior apprehension testing on physical examination. Microfracture was indicated in patients with a single, contained Outerbridge grade 4 glenoid articular defect involving the inferior half of the glenoid. Patients with lesions that were >4 cm2, partial thickness, or confined to the superior half of the glenoid were not included in this study.
From this cohort of eligible patients, we then identified all individuals who had undergone concomitant debridement and microfracture of Outerbridge grade 4 glenoid articular cartilage defects (microfracture cohort) versus labral repair alone (instability cohort).
Surgical Procedure
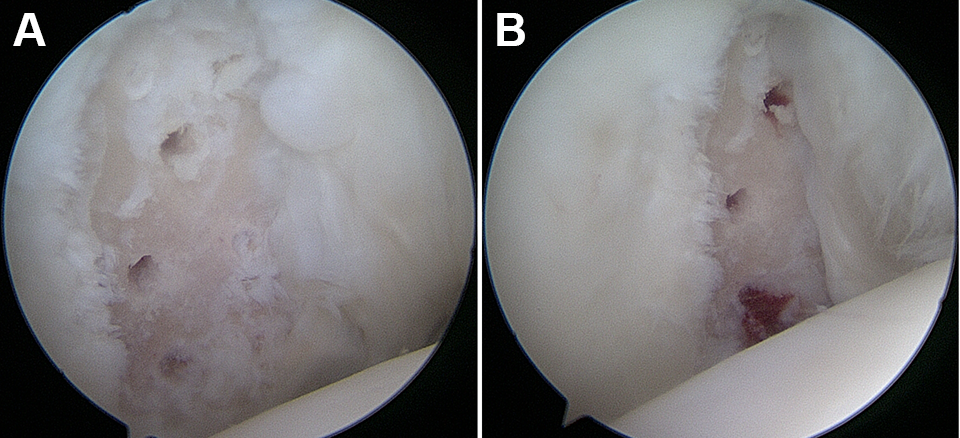
The technique of the senior surgeon (N.P.) did not change markedly throughout the duration of the study. All patients were positioned in a modified beach-chair position after administration of general anesthesia and a presurgical interscalene block. An examination was performed under anesthesia to assess range of motion (ROM) and stability in the anterior and posterior directions. A Spider hydraulic arm holder (Smith & Nephew) was then used to stabilize the operative shoulder and the patient was draped. Diagnostic arthroscopy of the glenohumeral joint was performed and the capsulolabral tear and chondral defect were identified. Any additional pathology present in the joint was noted at this time as well (Figure 1).

(A) Intraoperative image of a glenoid lesion and posterior inferior labral tear in the right shoulder of a 30-year-old male. (B) Intraoperative image of an Outerbridge grade 4 anterior inferior glenoid lesion (12 × 20 mm).
After completion of diagnostic arthroscopy, the torn labrum was mobilized from the glenoid neck. A small shaver was then utilized to create a bed of bleeding bone along the neck of the glenoid. The drill guide for the 3.0 Gryphon BR PEEK anchor (DePuy Mitek) was introduced and positioned on the face of the glenoid. A pilot hole was drilled, and the anchor was positioned into the glenoid. A suture passer was then used to shuttle one of the suture limbs through the capsule and labrum. Low-profile sliding knots were tied arthroscopically with care taken to position the knots away from the glenoid face (Figure 2).

Intraoperative image demonstrating posterior labral repair.
Following the completion of labral repair, additional concomitant intra-articular procedures were completed. Slight traction was applied to the humeral head to aid with access to the inferior aspect of the glenohumeral joint. For patients undergoing microfracture of isolated glenoid chondral lesions, the loose cartilage margins surrounding the chondral defect were debrided with an arthroscopic shaver, ring curette, and/or arthroscopic biter. A ring curette was used to create vertical walls around the defect, and the layer of calcified cartilage was debrided with a curette, taking care to not violate the subchondral bone. A microfracture awl was used to pierce the subchondral bone to the depth of approximately 3 to 4 mm, spacing the holes 3 to 4 mm apart (Figure 3A). Arthroscope inflow was terminated to verify that there was appropriate fill of the defect with bone marrow elements (Figure 3B). Subacromial bursectomy was then performed on all patients, as we have found that the delay from injury to operative management often experienced by active-duty military patients predisposes the injured shoulder to the development of a reactive subacromial bursitis, which we attribute to altered glenohumeral and scapulothoracic kinematics.
(A) Debrided glenoid lesion following microfracture. (B) Blood and stem cells flowing from the microfracture site.
Postoperative Rehabilitation
Patients were discharged the same day following their procedure. Pendulum shoulder and elbow, wrist, and finger active ROM exercises without shoulder movement were begun once the patient experienced complete resolution of the nerve block. Opioid pain medications were prescribed for up to 10 days postoperatively.
There was no difference in the postoperative protocol between patients who underwent simultaneous labral repair and glenoid microfracture and those who underwent labral repair alone. All patients were immobilized for 4 weeks in a SmartSling (Ossur) in a neutral rotation position. At 4 weeks, immobilization was discontinued, and passive forward flexion was started, with a slow progression of forward flexion from 90° to 150°. Active ROM and progressive strengthening of the operative shoulder was started at 6 weeks postoperatively. All patients attended physical therapy at the same military physical therapy group and followed the same postoperative rehabilitation protocol. Return to unrestricted activity was allowed as early as 6 months postoperatively, after the patient was cleared by physical therapy and endorsed subjective readiness to return to full duty.
Data Collection
Patient demographics including age, laterality, and military occupation were collected. Preoperative and postoperative data included ROM, the Single Assessment Numeric Evaluation (SANE) score, visual analog scale (VAS) for pain, Rowe instability score, and American Shoulder and Elbow Surgeons (ASES) shoulder score; all data were obtained as part of standard of care at all patient visits. Return to activity and complications were also collected as part of the postoperative evaluation.
Statistical Analysis
Statistical analysis was performed using SPSS Statistics (Version 25.0; IBM Corp). Continuous data were described by a combination of mean, standard deviation, range and 95% CI. A paired t test was used to compare the differences between the preoperative and postoperative results within the microfracture and instability groups. A separate subgroup analysis was performed to determine whether outcomes differed between dominant and nondominant arm involvement. In addition, an ordinary 1-way analysis of variance was used to compare continuous data across three groups to determine whether outcomes differed by variant of instability. Chi-square and Fisher exact tests were used to compare categorical variables between groups. Statistical significance was set at P < .05 in all cases.
As clinical significance thresholds after combined glenoid microfracture and labral repair have not been defined, existing values for the minimal clinically important difference (MCID), substantial clinical benefit (SCB), and Patient Acceptable Symptom State (PASS) after shoulder arthroplasty were used. Similarly, previously determined values for maximum outcome improvement (MOI) for the SANE and ASES after arthroscopic rotator cuff repair were used for this analysis. 2,14,29,30
Results
During the study period, the senior surgeon performed 288 labral repairs for shoulder instability on military patients <40 years old. A total of 36 had concomitant microfracture of an isolated glenoid osteochondrosis dissecans. Of those 36 patients, 3 had concomitant rotator cuff repair and 2 were lost to follow-up, leaving 31 patients (31 shoulders) in the microfracture cohort. Of the 252 patients without chondral defects who underwent isolated labral repair, 17 underwent rotator cuff repair, 13 had an osteochondral defect of the humeral head, and 13 were lost to follow-up, leaving 209 patients for final analysis in the instability cohort (Figure 4).

Flowchart of patient selection. w/out, without.
All patients in the microfracture group and 93.30% of instability patients were male, and the mean patient age was 31.90 years in the microfracture cohort and 29.84 years in the instability group. The microfracture cohort had a significantly longer average follow-up when compared with the instability group (95.58 ± 23.12 vs 83.38 ± 25.93 months; P = .014) (Table 1). Within the microfracture cohort, 11 patients had posterior instability (35.48%), 9 patients had anterior instability (29.03%), and 11 had combined anterior posterior instability (35.48%). This did not differ significantly from the distribution observed in the instability group, in which 73 patients had posterior instability (34.93%; P = .9517), 84 patients had anterior instability (40.19%; P = .2340), and 52 patients had combined instability (24.88%; P = .2105). Cartilage damage according to 1.5-T magnetic resonance arthrogram was seen in 18 patients (58%) in the microfracture cohort.
Comparison of Baseline Demographics, Preoperative Outcome Scores, and Concomitant Procedures Between Study Groups a

a Data are reported as mean ± SD or n (%) unless otherwise indicated. ASES, American Shoulder and Elbow Surgeons; RC, rotator cuff; ROM, range of motion; SANE, Single Assessment Numeric Evaluation; SLAP, superior labrum anterior-posterior; VAS, visual analog scale.
b Defined as nonadministrative/nonsupport infantry, artillery, and/or military police.
c Measured as highest thoracic level reached.
All patients in both cohorts were active-duty military at time of surgery; 23 (74.19%) of the microfracture patients and 157 (75.12%) of the instability patients were soldiers in a combat arms military occupation specialty (P = .9115). Combat arms was defined as nonadministrative, nonsupport infantry, artillery, or military police occupations. Of the 8 patients in the microfracture cohort who were not combat arms, 2 were mechanics, 2 were drivers, 1 was a computer technician, 1 was a supply specialist, 1 was a radar operator, and 1 was a firefighter.
Regarding concomitant procedures, arthroscopic subacromial bursectomy was performed on all patients in both cohorts. There was no significant difference in the number of patients undergoing concomitant arthroscopic debridement of a rotator cuff partial tendon tear, arthroscopic debridement of a type 1 superior labrum anterior-posterior lesion, or arthroscopic distal clavicle resection. A total of 78 patients in the instability cohort underwent arthroscopic-assisted subpectoral biceps tenodesis compared with 6 in the microfracture group (19.35% vs 37.32%; P = .0401). All chondral lesions were located in the inferior aspect of the glenohumeral joint. The average size of the glenoid defect in the microfracture group was 1.23 ± 1.03 cm2. Patients in the microfracture group had significantly higher preoperative VAS scores (8.10 ± 1.47 vs 7.43 ± 1.80; P = .049) and decreased internal rotation (T 10.55 ± 2.53 vs T 9.41 ± 2.91; P = .040). At the latest follow-up, statistically significant improvements in VAS pain, SANE, ASES, and Rowe scores were observed in both groups (P = .0001 for all) (Table 2). Outcome scores in the microfracture cohort did not differ significantly by shoulder dominance, size of chondral defect, or type of instability. When comparing postoperative outcomes between groups, patients in the microfracture cohort had significantly worse VAS, SANE, and ASES scores (P = .003, <.0001, and .001, respectively). In addition, postoperative ROM in forward flexion and external rotation was significantly, although only slightly, less in the microfracture cohort (P = .039 and .010, respectively).
Preoperative Versus Postoperative Outcomes Within Groups a

a Data are presented as mean ± SD. Internal rotation measured to thoracic spine level. Boldface P values indicate statistically significant difference (P < .05). ASES, American Shoulder and Elbow Surgeons; SANE, Single Assessment Numeric Evaluation; VAS, visual analog scale.
In the instability cohort, 93.78% of patients had returned to active duty at latest follow-up compared with 58.06% of microfracture patients (P < .0001). A total of 13 patients (41.94%) in the microfracture group had been medically discharged from the military at the end of the study period. There was no difference in the number of complications or patients requiring revision surgery between the 2 groups (Table 3). One patient (3.23%) in the microfracture cohort reported worsening of symptoms when compared with his preoperative status at latest follow-up.
Comparison of Postoperative Outcomes Between Groups a

a Data are presented as mean ± SD or n (%). Boldface P values indicate statistically significant difference between groups (P < .05). ASES, American Shoulder and Elbow Surgeons; SANE, Single Assessment Numeric Evaluation; VAS, visual analog scale.
Most microfracture patients met the MCID for the pain VAS, SANE and ASES, and 7 (22.58%), 17 (54.84%), and 20 (64.52%) microfracture patients achieved the PASS for VAS, SANE, and ASES, respectively (Table 4). When compared within the microfracture cohort by maintenance of active duty, patients who were able to return to military service were significantly more likely to achieve the PASS and MOI for the ASES and SANE, as well as reach the PASS for the VAS, when compared with those who were medically discharged (Table 5). When compared with instability patients, patients in the microfracture cohort were significantly less likely to meet the SCB, PASS, and MOI for the ASES (P = .004, .004, and <.0001, respectively), the PASS and MOI for the SANE (P < .0001 for both), and the PASS for the VAS (P = .0001).
Comparison of Patients Meeting the MCID, SCB, and PASS Between Groups a

a Data are presented as n (%). Boldface P values indicate statistically significant difference between groups (P < .05). ASES, American Shoulder and Elbow Surgeons; MCID, minimal clinically important difference; MOI, maximum outcome improvement; PASS, Patient Acceptable Symptom State; SANE, Single Assessment Numeric Evaluation; SCB, substantial clinical benefit; VAS, visual analog scale.
Comparison of Microfracture Patients Meeting the MCID, SCB, and PASS by Maintenance of Active Duty a

a Data are presented as n (%). Boldface P values indicate statistically significant difference between groups (P < .05). ASES, American Shoulder and Elbow Surgeons; MCID, minimal clinically important difference; MOI, maximum outcome improvement; PASS, Patient Acceptable Symptom State; SANE, Single Assessment Numeric Evaluation; SCB, substantial clinical benefit; VAS, visual analog scale.
Discussion
In our cohort of 31 young, active-duty servicemembers, combined microfracture and labral repair were found to produce modest, albeit statistically significant, improvements in PROMs at midterm follow-up. However, patients in the microfracture cohort had significantly worse postoperative outcome scores compared with patients undergoing labral repair without concomitant glenoid microfracture. At the end of the study period, only 58% of microfracture patients had returned to active-duty military service compared with over 93% of patients in the instability group.
Symptomatic glenoid chondral defects are at baseline a difficult pathology to treat, with little evidence to support or refute the few existing options for surgical management. In our study cohort, this was compounded by the reality that military patients with shoulder pain are a historically challenging population to manage. This population has a much higher incidence of shoulder instability when compared with civilians, as well as an increased likelihood of poor postoperative outcomes and complications. 24,26,34 –36 This is likely attributable to the high physical demands of many active-duty military jobs. 4,17,20 While the exact incidence of symptomatic glenoid osteochondral defects in military patients is unknown, it would be reasonable to presume that these lesions occur more often in members of the military than in civilians given their close association with instability and previous dislocation. 16,28 Out of the 288 young, active-duty military patients screened for inclusion in this study, 12.5% were found to have a glenoid osteochondral defect. Although there is a paucity of outcome data concerning the operative treatment of glenoid osteochondral defects in young patients, microfracture is currently the most evidence-based modality available. 8,16,28
We are not aware of any previously published studies reporting outcomes following combined glenoid microfracture and stabilization; however, our findings are of interest when compared with available outcome data following microfracture of glenohumeral cartilage lesions. One analysis of 17 shoulders showed a 10-year survivorship rate of 66.7%. 33 Another study by Hill et al 18 reported modest improvements in pain and functional scores following concurrent rotator cuff repair and glenohumeral microfracture. A study by Frank et al 11 showed a return to preoperative activity level of 88% in a cohort of 16 patients at midterm follow-up. However, other longer-term studies have reported clinical failure rates as high as 42% with over one-fifth of patients converting to arthroplasty. 12,21,25,31 While 42% of patients in our study were medically discharged from the military, 58% were able to maintain active-duty status at latest follow-up. No patients in our cohort had progressed to further surgery at the conclusion of the study period, and of the 13 patients that were medically discharged, all but 1 demonstrated improvement in symptoms following surgery.
While the rate of return to active-duty service observed was lower in the microfracture cohort than anticipated, we believe this finding is attributable to multiple factors. First, it is possible that prolonged time on restricted duty may have initiated medical separation in some patients. 6,7 Extended periods from diagnosis to definitive treatment are common among injured military patients, often due to variables such as deployment and transfer between bases. 35 In addition, despite experiencing statistically significant improvements in shoulder function and pain, active-duty military service may simply be too physically strenuous for these patients postoperatively. Interestingly, the rate of medical discharge in the microfracture cohort was noticeably higher when compared with rates in both our instability cohort, as well as those reported by previously published studies looking at shoulder stabilization in military patients. In a cohort of 52 patients undergoing 270° labral repair for combined instability, 92.31% were able to maintain active-duty service. 26 Similarly, 91.67% of patients returned to military duty after double-pulley remplissage in a cohort with off-track anterior shoulder instability, 27 and 93.75% of patients were able to return to preinjury levels of work following combined biceps tenodesis and labral repair for type VIII superior labrum anterior-posterior lesions with posterior instability. 15 These findings align with the high rate of return to active-duty observed in our instability cohort and suggest that patients with concurrent cartilage pathology may be significantly less likely to return to preinjury levels of activity when compared with those with instability alone.
It is noteworthy that, whereas fewer microfracture patients achieved the SCB or PASS for the ASES and SANE, all microfracture patients included in the study met the MCID for pain VAS and nearly 90% achieved the SCB for pain VAS. While the objective when treating young, active patients is to restore function and allow patients to return to preinjury levels of activity, these findings do suggest that combined microfracture and arthroscopic stabilization may offer some clinical benefit, particularly with regard to pain control, in patients with coexistent labral and cartilage injuries. It is also of interest that fewer patients in our study experienced postoperative complications or progressed to further surgery when compared with military patients undergoing total shoulder arthroplasty. While shoulder arthroplasty may be indicated for the operative management of older patients with chondral damage, a study by Kusnezov et al 19 found that in a cohort of young military patients undergoing shoulder arthroplasty, 46.2% experienced short-term complications and 23.1% required reoperation. In addition, weight-lifting restrictions are generally imparted upon patients following shoulder arthroplasty, which is generally incompatible with the physical demands of active-duty military service. Further studies are needed to fully elucidate the ideal management of osteochondral lesions in unstable shoulders; however, our results indicate that combined microfracture and labral repair may offer young patients some clinically meaningful improvement in shoulder pain and function with lower rates of complication and need for further surgery when compared with arthroplasty at a young age.
Limitations
There are several limitations to this study. First, our limited sample size and observational study design both represent potential sources of selection bias in this investigation. In addition, our microfracture cohort was composed of an entirely male active-duty population, potentially limiting the generalizability of our results to nonmilitary patients. The MCID, PASS, SCB, and MOI values used in this study have not been defined previously for this procedure, and therefore values previously established for shoulder arthroplasty and/or arthroscopic rotator cuff repair were used. 2,14,29,30 Follow-up imaging was not performed, limiting our ability to determine the extent of fibrocartilage formation at the site of the defect. Due to the nature of our database, additional information regarding mechanism of injury or number of instability events was not available, nor was information regarding activity restriction profile status for patients who returned to active-duty military service. Last, all surgeries were performed by the senior surgeon, who is a shoulder-elbow fellowship–trained surgeon.
Conclusion
Combined microfracture and arthroscopic labral repair produced modest, albeit statistically significant, improvements in PROMs and may be a reasonable treatment option for patients with isolated chondral defects who are not candidates for arthroplasty. However, microfracture patients had significantly worse PROMs than patients who underwent stabilization without concomitant chondral defects. At latest follow-up, only 58% of microfracture patients were able to maintain active-duty military service at midterm follow-up compared with >93% of patients with isolated instability.
Footnotes
Final revision submitted September 8, 2022; accepted September 26, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: J.C.D. has received hospitality payments from Stryker. N.P. has received consulting fees from Mitek. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Carson-Carthage (ref. No. 2021-17).