
Abstract
Background:
Although the identification of patellar tendon rupture is a clinical diagnosis aided by standard radiography, magnetic resonance imaging (MRI) may aid in identifying the location of the rupture and concomitant pathology.
Purpose:
To evaluate the characteristics of patellar tendon tears needing surgical repair and to determine whether patient or injury factors were predictive of tear location.
Study Design:
Case series; Level of evidence, 4.
Methods:
Consecutive patients who underwent primary patellar tendon repair for rupture between May 15, 2017, and April 10, 2020, were reviewed retrospectively. Exclusion criteria included age <18 years, surgical treatment of multiligamentous knee injury, laceration injury, and knee arthroplasty. Radiographs, MRI scans, MRI reports, clinic notes, and operative notes were evaluated. Statistical analysis was performed to determine factors associated with tear location, complications, and reoperation.
Results:
In total, 147 patients and 156 tendon tears were included; 82.1% of the tears were patellar avulsions, 14.7% were midsubstance or complex tears, and 3.2% were tibial avulsions. Patient and injury characteristics (body mass index, race, medical comorbidities, presence of patellar tendinitis, mechanism of injury, Insall-Salvati ratio, and the presence of infrapatellar bone fragments) were not predictive of tear location (P > .05). Patellar tendon ruptures were able to be clinically diagnosed correctly in >99% of cases. MRI was used to evaluate 77 (49.4%) knees. Patients who underwent MRI before surgery were more likely to have a history of preexisting tendinitis (P = .015) and a lower preoperative Insall-Salvati ratio (1.68 vs 1.52; P = .017).
Conclusion:
Patient and injury factors were not predictive of tear location. The majority of patellar tendon tears were avulsion-type injuries from the inferior patella. MRI was not necessary to aid in the diagnosis of patellar tendon rupture, as 99.4% of tears were able to be diagnosed clinically without advanced imaging.
Rupture of the patellar tendon is thought to occur primarily in patients 30 to 40 years of age, though it is well-recognized in older patients with certain medical comorbidities or those who have had previous injections into the area. 1,4 Identification of patellar tendon rupture is generally considered to be a clinical diagnosis aided by standard radiography. 1,4 The decision to obtain additional imaging is often provider-dependent, and magnetic resonance imaging (MRI) is considered a valuable modality to aid in diagnosis. 7,8 MRI also has the benefit of determining the location of the rupture (infrapatellar pole, midsubstance of the tendon, or at the tibial tuberosity) and whether there is concomitant intra-articular pathology. 5 Approximately half of tendon ruptures may be midsubstance or from the tibial tuberosity, 3,6 and the specific location of the tear and chronicity may dictate how a surgeon will repair the tendon, with some choosing to augment certain tear types. 2
Despite the utility of MRI to aid in the diagnosis of patellar tendon ruptures, it is unclear if obtaining an MRI scan alters the management of the patient. In addition, it is unclear whether certain patient or injury characteristics may affect tear location. The purpose of this study was to review patients who underwent repair of patellar tendon ruptures to determine whether patient presentation, demographics, and other characteristics correlate with location of the tear.
Methods
This was a retrospective review of consecutive patients who underwent primary patellar tendon repair for patellar tendon rupture at a single institution. Before beginning the study, institutional review board approval was obtained. Patients were identified using Current Procedural Terminology code 27380 and were included if they had undergone surgery between May 15, 2017, and April 10, 2020, and had an available operative report. Patients were excluded from analysis if they were <18 years, treated surgically for a multiligamentous knee injury, had sustained injury due to a laceration, had undergone previous knee arthroplasty in the ipsilateral knee, had undergone previous ipsilateral patellar tendon repair, presented with a chronic patellar tendon rupture, or if they were being treated for chronic patellar tendinitis without complete rupture (Figure 1).
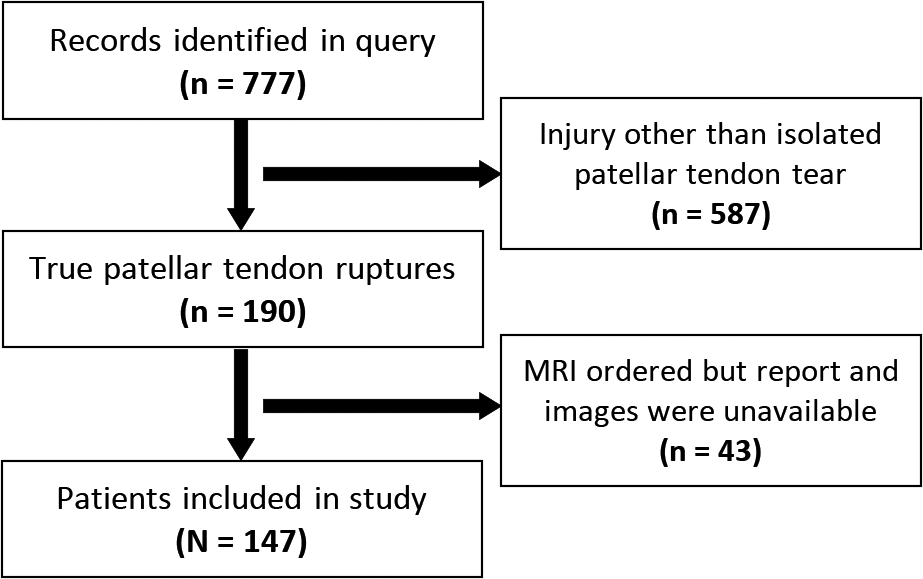
Flowchart of patient inclusion in the study. MRI, magnetic resonance imaging.
A chart review was performed to collect patient demographics, body mass index (BMI), injury mechanism, physical examination findings, and preoperative diagnosis. Comorbidities that predispose to patellar tendon injury, 1 the presence of preexisting tendinitis in either knee, and previous injuries were also recorded. When available, radiographs were analyzed to determine the Insall-Salvati ratio and whether there was an infrapatellar bone fragment on radiographic imaging (defined as a calcification or ossification distal to the patella within the tendon) consistent with an avulsion or tendinopathy. When performed and available, MRI scans and reports were included for evaluation. Operative notes were used to determine tear location, surgery performed, and the utilization of any additional augmentation technique. Augmentation included cerclage suturing through the patella and tibial tubercle or biologic graft augmentation. If a question remained about the tear location after reading the operative report, MRI scans, reports, and the operative technique employed were used to deduce the tear location. Available postoperative visits were reviewed to identify any complications, such as rerupture, arthrofibrosis, or infection, or reoperations for other pathology in the time period after the index procedure.
Statistical Analysis
To determine if any factors were associated with tear location or complications, statistical analysis was performed with significance determined at P < .05. A Mann-Whitney U test was used to calculate P values for continuous data and a chi-square test was used for categorical data. Kruskal-Wallis tests were used to calculate P values when comparisons were done using 3 variables. Data are presented as mean ± SD or as mean (interquartile range [IQR]).
Results
In the final analysis, 147 patients and 156 tendons were included, as 9 patients sustained simultaneous rupture of bilateral patellar tendons. A total of 152 tendons (97.4%) were treated within 4 weeks of the injury. Mean patient age at the time of surgery was 42.8 ± 12.7 years. Of the 147 patients, 135 (91.2%) were male. 17.9% of tears were atypical tears. See Table 1 for additional patient, injury, and demographic data. The mean Insall-Salvati ratio was 1.59 ± 0.33, and 87.1% of tears were repaired using transosseous tunnels. The remainder were primary end-to-end repair or suture anchors. Evidence of a bony avulsion or calcification within the proximal tendon was present on 49.1% of radiographs obtained.
Patient, Injury, and Imaging Characteristics a
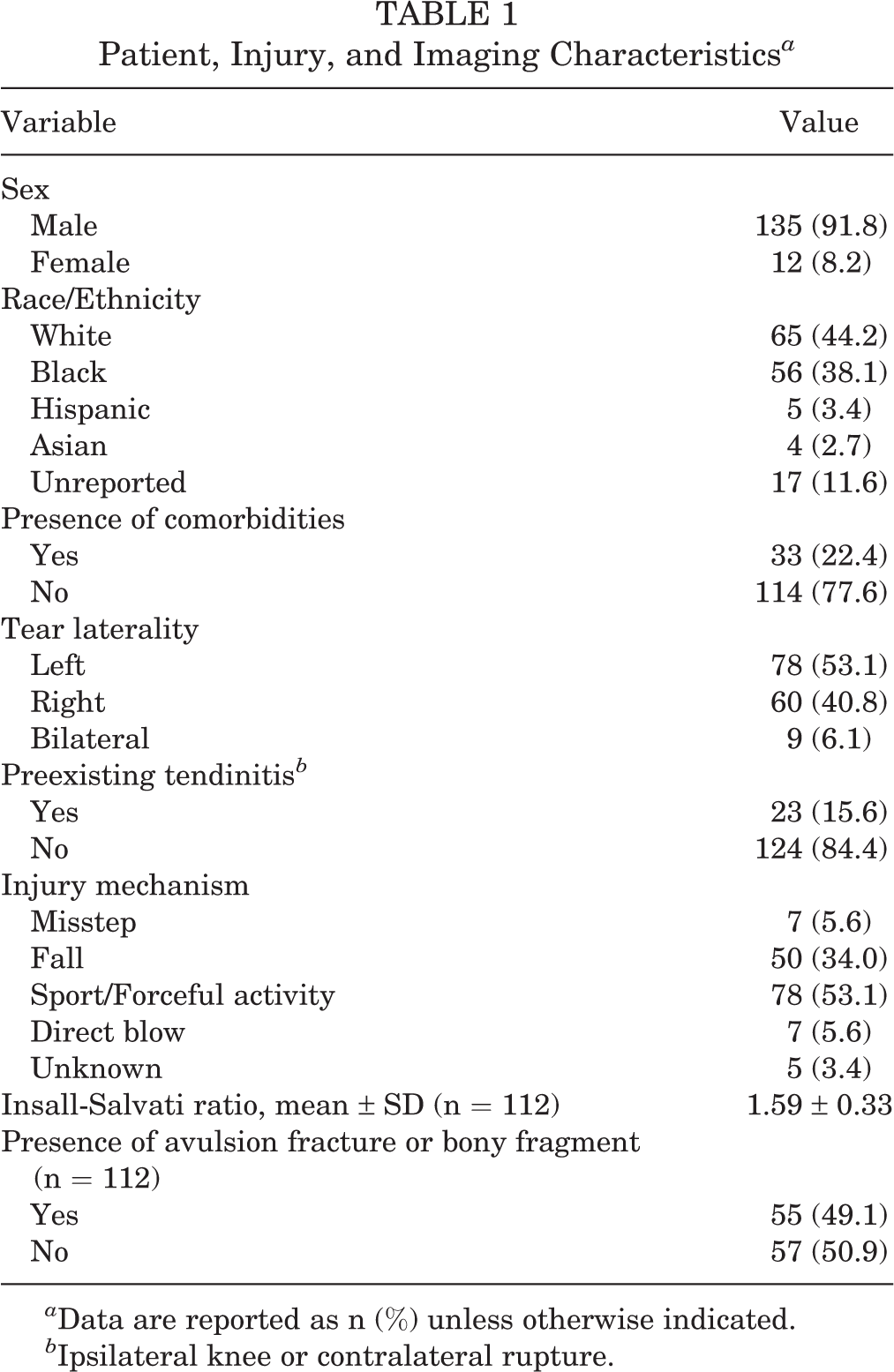
a Data are reported as n (%) unless otherwise indicated.
b Ipsilateral knee or contralateral rupture.
MRI was performed to evaluate 49.4% of the patellar tendon ruptures. In all but 1 case, the preoperative diagnosis of the orthopaedic surgeon was correct in identifying the patellar tendon rupture (99.4%). The 1 case was misdiagnosed as a “patellar subluxation,” and MRI confirmed the rupture of the patellar tendon. After review of operative reports and MRIs, 82.1% of tears were classified as having occurred from the inferior pole of the patella, 14.7% were midsubstance or complex tears, and 3.2% were avulsions from the tibial tubercle. Concomitant pathology was noted in 83.6% of MRIs. Meniscal tears were present in 12 patients (21.8%) with a mean age of 56.3 ± 10.9 years. Three high-grade ligament tears were noted on MRI: a 57-year-old with grade 2 lateral collateral and medial collateral ligament tears, a 52-year-old with a grade 2 posterior cruciate ligament tear, and a 24-year-old with a grade 2 anterior cruciate ligament tear that was felt to be stable on examination. In this population, there were no reoperations to address concomitant pathology. Intraoperatively, repair augmentation was used in 14.1% of cases. Seven complications were identified, including 3 reruptures (4.8%), 2 cases of arthrofibrosis (1.4%), and 2 pulmonary embolisms, with 1 resulting in death (Table 2).
Tear Location, Concomitant Pathology, Operative Technique, and Postoperative Complications a

a MRI, magnetic resonance imaging.
b Of the 77 MRIs, 55 (71.4%) were available for review.
c 1 death.
Patient age, sex, race, and BMI were not associated with tear location. Similarly, bilateral tears, a history of knee injury, preinjury tendinopathy (ipsilateral tendinitis or contralateral patellar tendon ruptures), mechanism of injury, and the presence of medical comorbidities or bony fragments were not associated with tear location. Similarly, the percentage of patients undergoing MRI did not differ based on tear location (P > .05). The mean (IQR) preoperative Insall-Salvati ratios were 1.59 (1.37-1.79) for infrapatellar ruptures, 1.58 (1.36-1.71) for midsubstance ruptures, and 1.36 (1.07-1.58) for tibial tubercle avulsion (P = .231). Intraoperative augmentation of the repair was utilized in 11.3% of infrapatellar tears, 34.8% of midsubstance tears, and 20% of tibial avulsions (P = .003) (Table 3).
Surgical Repair Technique Based on Tear Location a

a Data reported as n (%).
When comparing patients with preexisting tendonitis with those without preexisting tendonitis, there was no difference in tear location, sex, BMI, race, or use of intraoperative augmentation. However, patients with tendinitis tended to be younger (36.5 ± 10.9 vs 43.6 ± 12.8 years; P = .02) and have a lower preoperative Insall-Salvati ratio (1.45 ± 0.27 vs 1.61 ± 0.31; P = .04). They were also more likely to receive an MRI (47.6% vs 78.3%; P = .02).
Discussion
The majority of patellar tendon tears are avulsion-type injuries from the inferior patella, and no risk factors for midsubstance or tibial avulsion tears were identified. MRI was not necessary to aid in the diagnosis of patellar tendon rupture, as orthopaedic surgeons have a high rate of assigning a correct diagnosis (99.4%) at presentation. In this study, which excluded multiligamentous knee injuries, it was unnecessary to use MRI to make the diagnosis in nearly all cases of patellar tendon tear.
We found that 82.1% of patellar tendon ruptures either occurred from the inferior pole of the patella or could be addressed as such, utilizing a standard transpatellar tunnel repair technique. Roudet et al 6 had found that only 52.6% of patellar tendon tears could be classified as from the inferior pole of the patella, while Hsu et al 3 found that number to be 45.7%. With atypical tears (ie, avulsions) from the tibial tubercle or complex tears involving the midsubstance of the tendon, surgeons may elect to use tissue or suture augmentation. 2 In our investigation, we were unable to identify any risk factors that would predict tear location, information that might be helpful in weighing the utility of obtaining an MRI scan.
MRI scans may have affected the surgical repair performed. When no MRI was performed, there were no instances of biologic or suture cerclage usage, although there were 5 instances of each in the group who underwent MRI, despite having similar numbers in each group. Suture augmentation (ie, suture or suture tape spanning the tendon repair) was used in both the MRI and the no-MRI group and may represent a standard repair technique for surgeons regardless of tear location. Increased use of augmentation techniques after advanced imaging suggests that surgeons may obtain an MRI to aid in surgical planning. It is possible that more severe injuries required surgical augmentation and that MRI was performed before surgery to help identify the need for surgical augmentation. Further, the health insurance status of patients was not analyzed in this study, and it is possible that both MRIs and augmentation were performed in cases where it was financially viable.
In our study, an MRI scan was also more likely to be obtained in instances of preexisting tendinitis (P = .015) and in instances with a lower preoperative Insall-Salvati ratio (1.68 vs 1.52; P = .017), although preexisting tendinitis was not predictive of tear location and preoperative Insall-Salvati ratios were 1.59 (IQR, 1.37-1.79) for infrapatellar ruptures, 1.58 (IQR, 1.36-1.71) for midsubstance ruptures, and 1.36 (IQR, 1.07-1.58) for tibial tubercle avulsions (P = .231).
During the follow-up period, no patients returned to the operating room for concomitant pathology, despite being present on 83.6% of MRIs. Meniscal pathology was noted in 21.8% of patients who underwent MRI, with a mean age of 56.3 ± 10.9 years, which may explain the successful nonoperative management of these injuries. Ligamentous injuries were present in 23.6%, of which 5.5% were grade 2 or 3 injuries on MRI. We excluded multiligamentous knee injuries with concomitant patellar tendon rupture, of which there were 6 during the study period, demonstrating the need for careful physical examination at the time of presentation. Overall, the complication rate was low, with 7 complications identified during the follow-up period. Given the small number, analysis could not be performed to identify risk factors for experiencing a complication.
Limitations
A major limitation of this study was its retrospective nature. Data collection relied on chart notes from multiple surgeons, and there may have been omissions with regard to patients’ preexisting conditions and other information. Follow-up and complication information may have been incomplete if patients were lost to follow-up. Despite reviewing multiple years of data, the number of atypical tears remained low at 17.9%, which was lower than previously reported data and may have limited our ability to identify risk facts for their occurrence. Patellar tendon tear locations were defined most often by the surgeon but, in several instances, the location of the tear was deduced through a combination of the repair technique and MRI, if available. Finally, patients with multiligamentous knee injuries were excluded from analysis given that the focus of the present study was to determine the utility of MRI in the setting of isolated patellar tendon tears.
Conclusion
Patient and injury factors were not predictive of tear location. The majority of patellar tendon tears are avulsion-type injuries from the inferior patella. MRI was not necessary to aid in the diagnosis of patellar tendon rupture, as 99.4% of tears were able to be diagnosed clinically without advanced imaging.
Footnotes
Final revision submitted August 9, 2022; accepted September 13, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: P.O. has received education payments from Liberty Surgical, Smith & Nephew, and Summit Surgical. K.B.F. has received education payments from Liberty Surgical, consulting fees from Medical Device Business Services, and speaking fees and honoraria from Vericel. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Thomas Jefferson University.