
Abstract
Background:
The Hospital for Special Surgery Pediatric Functional Activity Brief Scale (HSS Pedi-FABS) has demonstrated normally distributed scores in children aged 10 to 18 years. It has been used to evaluate knee injuries; however, there is limited information regarding its use in evaluating other injury types.
Purpose:
To (1) assess the validity and utility of HSS Pedi-FABS in youth athletes with injuries to different parts of the body and (2) evaluate the association between the HSS Pedi-FABS and the Patient-Reported Outcomes Measurement Information System (PROMIS) Pediatric Global Health 7 (PGH), as well as PROMIS–Pain Interference (PGH-PI) and PROMIS-Fatigue (PGH-F) components.
Study Design:
Cohort study (diagnosis); Level of evidence, 3.
Methods:
The authors performed a retrospective review of youth athletes aged 10 to 18 years who completed the HSS Pedi-FABS as part of their previsit intake questionnaire between April 2016 and July 2020. HSS Pedi-FABS score distributions were compared and evaluated for ceiling effects in cohorts determined by demographic, injury characteristic, and sports participation variables; a ceiling effect was determined to be present if >15% of respondents received the highest possible score. HSS Pedi-FABS scores were analyzed for a correlation with PGH, PGH-PI, and PGH-F components.
Results:
Included were 2274 patients (mean age, 14.6 ± 2.1 years; 53.0% female) participating in 21 distinct primary sports for 9.6 ± 7.9 hours per week. The mean HSS Pedi-FABS scores by injury group were as follows: elbow (22.7 ± 6.7), shoulder (21.0 ± 8.7), ankle (20.2 ± 8.8), knee (19.5 ± 9.1), and hip (15.4 ± 10.4) (P < .001). Broad distribution was seen in each cohort, with no floor or ceiling effects. The HSS Pedi-FABS score correlated with patient-reported hours per week (r = 0.33), days per week (r = 0.33), and years of participation (r = 0.21) (P < .001 for all). All 3 PROMIS components correlated with HSS Pedi-FABS: PGH (r = 0.28), PGH-PI (r = –0.11), and PGH-F (r = –0.15) (P < .001).
Conclusion:
Study findings indicated that the HSS Pedi-FABS is a valid tool for measuring physical activity level in most injured youth athletes, not just those with knee injuries. The correlation of HSS Pedi-FABS with the PGH suggests a positive relationship of childhood physical activity with general health.
Keywords
While youth sports participation rates are difficult to calculate, some national surveys and league reports estimate that as many as 60 million children aged 6 to 18 years participate in organized sports. 7 In the pediatric and adolescent populations, physical activity is associated with better physical, mental, and cognitive health outcomes. 6,28,38,45,47 Although physical activity is well studied, the 2020 World Health Organization guidelines on physical activity and sedentary behavior indicate that significant knowledge gaps remain regarding potential risks and benefits inferred by volume, intensity, and other aspects of physical activity. 6 The literature indicates that children’s risk of athletic injury is rising as the average age of participants in organized youth sports decreases over time. 28,40,42 While young athletes, their parents, and their coaches may believe that more practice will lead to success in their primary sport, 11,29 evidence suggests that these athletes are at risk of early retirement from competitive sports because of burnout and chronic injury. 8,9,15,21,35,48
Accurately assessing activity level is essential for determining treatment, as treatment decisions and discussions may be different for recreational athletes compared with those interested in future collegiate sports. Activity level is also paramount in reviewing the outcomes after a sports-related injury in youth athletes and determining successful return to sports. Patient-reported outcome measures (PROMs) are important tools for objective, reproducible orthopaedic research, but implementation remains variable. 5 Adult-validated PROMs are commonly employed in the pediatric and adolescent population, although pediatric-specific PROMs are available and have been validated, such as use of the Pediatric International Knee Documentation Committee (Pedi-IKDC) over the IKDC questionnaire. 12,26,27 The Hospital for Special Surgery Pediatric Functional Activity Brief Scale (HSS Pedi-FABS) was developed in 2013 to improve the evaluation of posttreatment outcomes and patient-reported activity for athletes aged 10 to 18 years. 13 Completion of the scale results in a composite score from 0 to 30 based on 8 components of physical activity (running, cutting, decelerating, pivoting, duration, endurance, competition, and supervision) during the previous month. Representative data from 2018 demonstrated a normal distribution in a healthy population. 14 Among pediatric athletes who underwent knee evaluation, the HSS Pedi-FABS indicated improved utility when compared with the Tegner activity level scale, a measure designed for adults. 46 The validity of the pediatric activity measure when used in a highly active population with an array of injuries has yet to be established. Validation of HSS Pedi-FABS regardless of injury type could allow broad application of the scale in sports medicine and public health research. A widely used activity scale may contribute to a better understanding of the impact of sports participation, overtraining, and specialization in pediatric and adolescent athletes. 25
The purpose of this study was to (1) assess the validity and utility of HSS Pedi-FABS in a population of 10- to 18-year-old athletes evaluated with injuries to different parts of the body and (2) evaluate the relationship of HSS Pedi-FABS activity scores with general health as measured by the Patient-Reported Outcomes Measurement Information System (PROMIS) Pediatric Global Health 7 (PGH), as well as PROMIS–Pain Interference (PGH-PI) and PROMIS-Fatigue (PGH-F) components. We hypothesized that HSS Pedi-FABS scores would correlate with self-reported activity level in this study population, regardless of injury group, and that no floor or ceiling effects would be present.
Methods
Study Population
This study received institutional review board approval with a waiver of informed consent before initiation. A retrospective review of 2962 patients evaluated at a single pediatric sports medicine institution between April 2016 and July 2020 was performed. Participants aged 10 to <19 years were included if they completed a previsit intake questionnaire and HSS Pedi-FABS within 2 weeks of their initial assessment. Patients with injuries to the ankle, knee, hip, elbow, or shoulder had data available for review. A total of 2274 pediatric sports medicine patients met these inclusion criteria for data collection and analysis. Patients who self-reported participation in at least 1 sport on intake paperwork were considered athletes.
Data Collection
The intake questionnaire administered to patients evaluated at the clinic analyzed demographic information, sports participation history, and injury characteristics. Patient data were obtained during review of the electronic medical records for selected participants contained in Epic (Epic Systems). Demographic and injury data including date of injury, injury type, age, and sex were available for all patients. Additionally, sports participation data including competition level, aspirations to play in college or professionally, and patient-reported hours and days of activity per week were available for patients who indicated participation in athletics. The HSS Pedi-FABS and PROMIS PGH were administered through an electronic PROM management software (Oberd) on electronic tablets in the clinic. Electronic collection of PROMs has demonstrated validity and reliability in this setting and population. 31,41
The HSS Pedi-FABS evaluates running, cutting, decelerating, pivoting, duration, endurance, competition, and supervision during the past month, with higher scores indicating more activity; the maximum score is 30 (Supplemental Material 1). 13 The PROMIS PGH assesses respondents’ physical, mental, and social health in general when compared with the national average score of 50 (Supplemental Material 2). The PGH-PI and PGH-F components ask patients to recall their experiences in the past 7 days. A higher score on PROMIS PGH indicates more of the attribute being measured. 16,17,26,40
Statistical Analysis
Descriptive statistics were used to analyze HSS Pedi-FABS score distribution and the presence of a floor or ceiling effect in the whole population and cohorts determined by demographics, injury characteristics, and sports participation. A floor or ceiling effect was determined to be present if >15% of respondents scored the lowest or highest possible score. 44 Mann-Whitney or Kruskal-Wallis tests followed by the Dwass-Steel-Critchlow-Fligner method for multiple comparisons were used to compare mean scores in each cohort as appropriate. Spearman correlations were calculated to assess the association of PROMIS PGH and other continuous variables with HSS Pedi-FABS scores. Skew, kurtosis, and a Q-Q plot were used to evaluate the shape of the score distributions. Statistical significance was set at P < .05. Statistical analysis was performed using SAS version 9.4 (SAS Institute).
Results
Cohort Characteristics
The 2274 participants had a mean age of 14.6 ± 2.1 years, with 53.0% being female. Of these patients, 2010 youth athletes reported participating in sports for 9.6 ± 7.9 hours per week during 32.3 ± 15.7 weeks per year, with 6.2 ± 3.4 years of participation in 21 distinct primary sports. Among these athletes, 80.3% (n = 1614) reported participation in a single sport, and the most common primary sport was soccer (n = 367). Knee injuries were the most evaluated injury type (Table 1). The average HSS Pedi-FABS score in this population of athletes was 19.7 ± 9.1. A Q-Q plot demonstrated that the data were nonparametric (Figure 1). The skewness and kurtosis were determined to be –0.86 and –0.48, respectively, indicating a broad distribution of HSS Pedi-FABS scores with moderate negative skewness and light tails. While no floor or ceiling effects were noted, the second highest possible score, 29, was the most common (13.1%) (Figure 2).
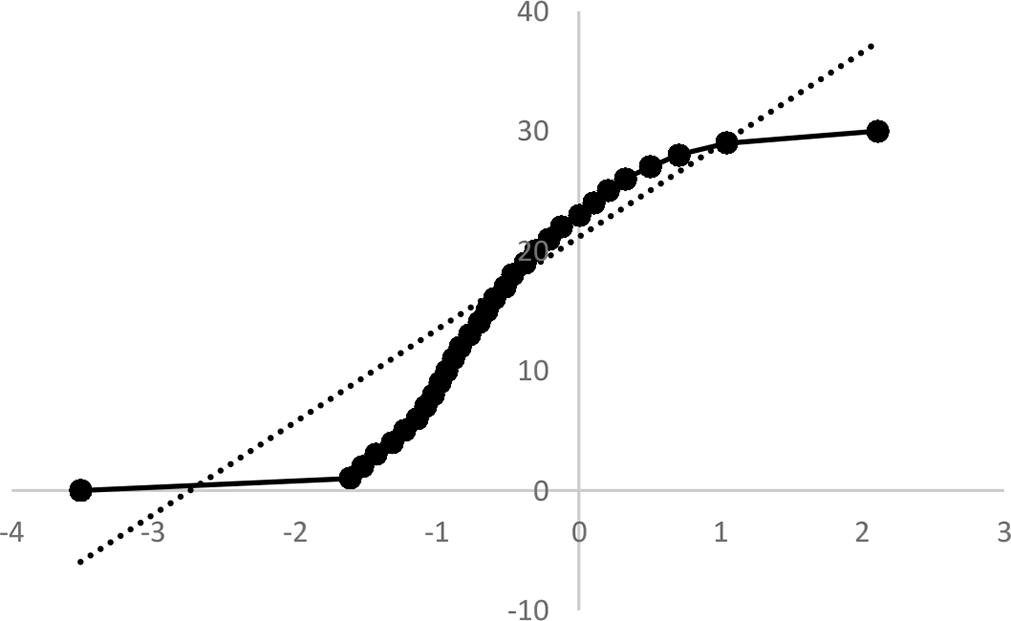
Q-Q plot comparison of Hospital for Special Surgery Pediatric Functional Activity Brief Scale scores to a normal distribution.
Primary Sports and Injury Locations of the Study Cohort


Hospital for Special Surgery Pediatric Functional Activity Brief Scale (HSS Pedi-FABS) score distribution for the overall cohort. The mean, median, mode, and quartiles are highlighted by alternating shaded regions.
On the HSS Pedi-FABS competition question, 59% (n = 1334) of respondents indicated they compete in sports with an official or judge. More than one-third (34.2%) of the athletes in this cohort reported club, select, national, or elite participation in sports on their intake form. Male athletes scored significantly higher than female athletes on the HSS Pedi-FABS (21.5 ± 8.3 vs 18.1 ± 9.4; P < .001). No association between age and HSS Pedi-FABS score was observed in this study (r = 0.02; P = .46). However, scores did correlate with total years of participation in sports (r = 0.21; P < .001). Although there were no statistical differences between mean scores by age, the score distributions varied among athletes of different ages. The shape of the curves indicated more polarized scores among older participants, as patients aged 18 years received the greatest proportion of both the highest and lowest scores (Figure 3).

Hospital for Special Surgery Pediatric Functional Activity Brief Scale (HSS Pedi-FABS) score distributions by age.
Activity Level by Injury Characteristics
Average HSS Pedi-FABS score distributions varied significantly across injury groups (Figure 4). Athletes with injuries to the elbow (22.7 ± 6.7) scored the highest, followed by the shoulder (21.0 ± 8.7), ankle (20.2 ± 8.8), knee (19.5 ± 9.1), and hip (15.4 ± 10.4) (P < .001). In post hoc analysis, participants with elbow injuries had significantly higher scores than those with hip (P < .001) or knee (P < .001) injuries. Participants with hip injuries scored significantly lower than all other injury cohorts (all P < .001).
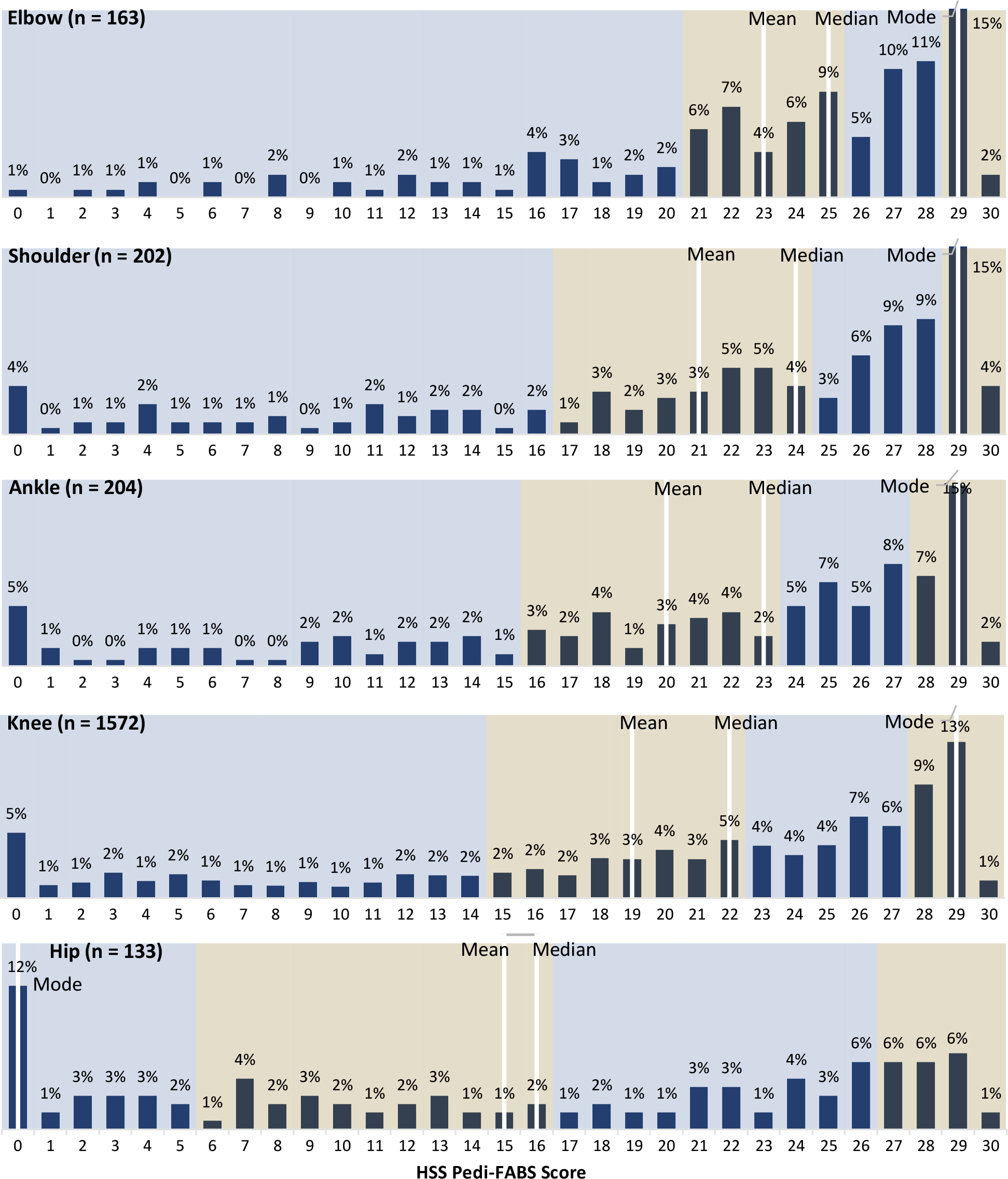
Hospital for Special Surgery Pediatric Functional Activity Brief Scale (HSS Pedi-FABS) score distributions by injury group. The mean, median, mode, and quartiles are highlighted by alternating shaded regions.
When grouped into lower extremity and upper extremity injuries, participants with upper extremity injuries (n = 365; mean score 21.8) scored significantly higher than those with lower extremity injuries (n = 1909; mean score 19.3) (P < .001). HSS Pedi-FABS scores correlated with patient-reported hours of participation per week and days of participation per week (Table 2). Notably, these relationships were maintained in each of the injury groups. An inverse correlation was observed between HSS Pedi-FABS and days from injury to evaluation (r = –0.30; P < .001).
Correlation of HSS Pedi-FABS Scores With Patient-Reported Activity According to Injury Group a

aP < .001 for total cohort, elbow, shoulder, ankle, and knee; P = .02 for hip activity in hours per week; P = .01 for hip activity in days per week. HSS Pedi-FABS, Hospital for Special Surgery Pediatric Functional Activity Brief Scale.
Sports Participation Impact on Activity Level
HSS Pedi-FABS score distributions remained comparable across the sports evaluated, except for cheer/tumbling and dance/drill team/ballet, for which these athletes scored significantly lower than all other athletes (P < .001) (Table 3). Single-sport specialization did not indicate a difference in scores. However, club/select and national/elite athletes scored higher on average than those reporting only school/recreational competition (P < .001). Participants pursuing college and/or professional sports scored significantly higher than those anticipating retirement before college.
HSS Pedi-FABS Score Distributions by Sports Participation Characteristics Among Self-Reported Athletes in Study Cohort a

a Data are presented as mean ± SD. Dash indicates no comparison. HSS Pedi-FABS, Hospital for Special Surgery Pediatric Functional Activity Brief Scale.
Activity Association With General Health
PROMIS data were available for 1000 participants with mean scores of 50.9 on the PGH, 49.2 on the PGH-F component, and 51.1 on the PGH-PI component. The PGH component correlated with the HSS Pedi-FABS, with higher activity scores indicating better general health (r = 0.28; P < .001). Higher activity scores also correlated with less fatigue and pain interference, but to a lesser degree (PGH-F: r = –0.15, P < .001; PGH-PI: r = –0.11, P < .001).
Participants in the top quartile of activity level according to HSS Pedi-FABS scored significantly better on the PGH component (54.1) than all other participants (Figure 5). Athletes in the lowest quartile of HSS Pedi-FABS scores were the only group with worse than average PGH-F component scores (50.5). PGH-PI components scores were elevated on average in this cohort (51.1), but more so among those in the lowest quartile of HSS Pedi-FABS (52.2) (Figure 5).

PROMIS Global Health, PROMIS–Fatigue, and PROMIS–Pain Interference component scores grouped by HSS Pedi-FABS quartile (Q): 1st Q represents participants with the lowest 25% of HSS Pedi-FABS scores; 2nd Q, 25% to 50% of scores; 3rd Q, 50% to 75% of scores; and 4th Q, highest 25% of scores. PROMIS, Patient-Reported Outcomes Measurement Information System.
Discussion
Among 2274 patients evaluated at a pediatric sports medicine clinic, the HSS Pedi-FABS demonstrated a broad distribution of scores without any floor or ceiling effects. Additionally, our hypothesis was confirmed, as HSS Pedi-FABS scores correlated with self-reported activity level in each injury group. These findings suggest that HSS Pedi-FABS may be used to accurately assess physical activity level for most pediatric and adolescent athletes. Higher scores were associated with more recent onset of injury/symptoms, college or professional aspirations, and better global health. Additionally, athletes evaluated with appendicular injuries were associated with higher scores than those evaluated with more core injury locations. These clinically relevant patient qualities were associated with their HSS Pedi-FABS score at the time of evaluation.
In 2018, the HSS Pedi-FABS was shown to have a normal distribution in the general population with elevated scores among athletes. 14 A greater proportion of respondents in the current study reported participation in organized competitive sports with an official or judge compared with the normative paper from 2018 (59% vs 38%). A corresponding higher average HSS Pedi-FABS score was noted in our cohort (19.7 ± 9.1) compared with the general population (15.4 ± 8.5), which resulted in a left-skewed distribution. Although there was a remarkably high proportion of competitive athletes, a wide range of scores were reported without any ceiling effects. This indicates that the scale is capable of accurately assessing activity level among the most active and competitive youth athletes.
In many academic sports medicine settings, multiple, joint-specific, functional PROMs are administered to patients at their initial visit to establish baseline values to compare with outcomes after treatment. 2,10,18,27,39,50 A particularly important outcome for athletes is return to previous level of activity. Some PROMs have a component dedicated to activity, but even dedicated activity scales such as the Tegner demonstrate ceiling effects in youth athlete populations. Among athletes with knee injuries, Wagner et al 46 noted that one-third of respondents received the maximum score when using the Tegner score to evaluate activity level, in contrast to a robust score distribution from the HSS Pedi-FABS instrument. We found that the HSS Pedi-FABS score correlated with self-reported activity level in 5 cohorts of youth athletes with injuries to different joints of the body. Although the knee is among the most frequently injured parts of the body during sports participation, generalized use of the HSS Pedi-FABS may allow for adequate assessment of injuries to other joints or bones. This may simplify PROM administration for clinical staff and provide an additional cross-injury comparison for researchers. 23,30
In this cohort, patients with elbow injuries exhibited significantly higher HSS Pedi-FABS scores than those with knee injuries, and patients with hip injuries scored lower than all other injury groups. Although not all differences achieved statistical significance, athletes with appendicular and/or upper extremity injuries reported higher activity scores than those with hip or lower extremity injuries. While the movements included in the scale are associated with lower extremity injuries, these movements are components of agility that are common to both upper and lower extremity intensive sports. Therefore, high levels of engagement with the agility-based movements measured by HSS Pedi-FABS may be associated with elbow and ankle injuries. Considering that the HSS Pedi-FABS asks about activity during the previous month, some athletes may have experienced a decrease in activity level before the time of evaluation. Subsequently, we observed lower HSS Pedi-FABS scores as the time from injury to initial evaluation increased. The scale’s correlation with time from injury to evaluation may disseminate information regarding delayed evaluation or chronic injury to providers and may impact research when used as a measure of baseline activity.
The various health benefits of physical activity for developing children have been studied extensively. 22,34,37,43 These benefits form the foundation of many guidelines created by leaders in pediatric and adolescent health, such as the World Health Organization and the American College of Sports Medicine. 24,49 The positive correlation between HSS Pedi-FABS and PGH in this study provides additional support for this association; however, a distinctive quality of this cohort was participants’ injured status. Early specialization, overtraining, and burnout in youth sports have demonstrated elevated injury risk and caught the attention of sports media outlets. 3,8,9,19,20,33 The prevalence of these risk factors may be a result of athletes attempting to develop the skill necessary to compete at increasingly high competition levels and obtain scholarships. 1,4,32,36 In this cohort, 71% of respondents reported aspirations to play at least collegiately, and 34% reported aspirations to compete professionally. Previous literature describes decreasing HSS Pedi-FABS scores with increasing age, which may indicate a natural attrition from sports as children get older and available team positions reduce. No correlation with age was observed in this study of currently active athletes. Instead, greater total years of participation was associated with higher HSS Pedi-FABS scores, which further highlights that aging youth athletes face the decision to retire or prepare to compete beyond high school. This study demonstrates that HSS Pedi-FABS can effectively measure the activity level of highly active pediatric and adolescent athletes with injuries to 5 different joints. Therefore, it may play an important role in future clinical and public health research investigating the impact of the timing, intensity, and variety of physical activity during childhood development.
Limitations
The limitations of this study include those inherent to retrospective studies. The participants in this study were injured, but the inclusion criteria required completion of the PROMs within 2 weeks of evaluation to assess activity level near the time of injury. Since HSS Pedi-FABS asks about activity during the previous month and time from injury to evaluation varied in this cohort, recall bias is another important consideration for the analysis of this data set. Organized sports are seasonal in nature; therefore, some athletes may score differently depending on the point in the season. The large sample size across multiple years should minimize this effect. Although injuries to multiple joints were included, the sample was made up primarily of participants with knee injuries, and not all sports injuries are represented. HSS Pedi-FABS measures general activity rather than joint-specific function; however, the scores of upper extremity athletes may be influenced by attributes not assessed in this study because the content of the scale is more closely related to lower extremity function. All participants in this cohort were treated at a single institution in an area with high levels of youth sports participation. Multicenter research is needed to improve the generalizability of the results in this study.
Conclusion
The HSS Pedi-FABS is a valid tool for measuring physical activity level in youth athletes with injuries to various joints in addition to the knee. Youth athletes with high activity levels according to HSS Pedi-FABS may be at elevated risk of upper extremity or appendicular injury. HSS Pedi-FABS scores indicate that aging youth athletes should retire or increase their activity level in order to continue participation in sports. Although a positive association of physical activity with general health is well-established, HSS Pedi-FABS may be useful in future research efforts to identify injury risk factors for youth athletes.
Supplemental Material for this article is available at https://journals.sagepub.com/doi/full/10.1177/10.1177/23259671221143534#supplementary-materials
Supplemental Material
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671221143534 - An Activity Scale for All Youth Athletes? Clinical Considerations for the HSS Pedi-FABS
Supplemental Material, sj-pdf-1-ojs-10.1177_23259671221143534 for An Activity Scale for All Youth Athletes? Clinical Considerations for the HSS Pedi-FABS by Connor M. Carpenter, Savannah B. Cooper, Philip L. Wilson, Shane M. Miller, Charles W. Wyatt, Benjamin L. Johnson, Kevin G. Shea and Henry B. Ellis in Orthopaedic Journal of Sports Medicine
Supplemental Material
Supplemental Material, sj-pdf-2-ojs-10.1177_23259671221143534 - An Activity Scale for All Youth Athletes? Clinical Considerations for the HSS Pedi-FABS
Supplemental Material, sj-pdf-2-ojs-10.1177_23259671221143534 for An Activity Scale for All Youth Athletes? Clinical Considerations for the HSS Pedi-FABS by Connor M. Carpenter, Savannah B. Cooper, Philip L. Wilson, Shane M. Miller, Charles W. Wyatt, Benjamin L. Johnson, Kevin G. Shea and Henry B. Ellis in Orthopaedic Journal of Sports Medicine
Footnotes
Final revision submitted August 2, 2022; accepted September 16, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: P.L.W. has received education payments from Pylant Medical. K.G.S. has received education payments from Evolution Surgical and hospitality payments from Arthrex. H.B.E. has received education payments from Pylant Medical, speaking fees from Smith & Nephew, and hospitality payments from Stryker. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from the University of Texas Southwestern Medical Center (reference No. STU-2019-0701).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.