
Abstract
Background:
The Hospital for Special Surgery Pediatric Functional Activity Brief Scale (HSS Pedi-FABS) is a specifically designed scoring system for children and has been translated into several languages. However, to date, no validated Japanese version of this scoring system is available.
Purpose:
To translate the HSS Pedi-FABS into Japanese and assess its reliability and validity.
Study Design:
Cohort study (diagnosis); Level of evidence, 2.
Methods:
The HSS Pedi-FABS was translated into Japanese and back-translated into English to confirm the appropriateness of the translation. A total of 764 children aged 9 to 15 years participated in the validation study. The participants answered the Japanese version of the HSS Pedi-FABS along with 2 other questionnaires in Japanese (the Physical Activity Questionnaire for Older Children [PAQ-C] and the physical activity questionnaire of the World Health Organization’s Health Behavior in School-aged Children [HBSC PAQ]). At 1 month after the first assessment, the children answered the Japanese version of the HSS Pedi-FABS again. We evaluated reliability using the Cronbach alpha and the intraclass correlation coefficient. Validity was evaluated by quantifying floor and ceiling effects, correlations between the HSS Pedi-FABS and the PAQ-C, the HSS Pedi-FABS discrepancy between active and inactive groups divided by the HBSC PAQ, and correlation between the HSS Pedi-FABS and body mass index.
Results:
HSS Pedi-FABS scores were slightly but significantly higher in male participants (mean = 16.7) than in female participants (mean = 13.2). The Cronbach alpha coefficient was .90, and the intraclass correlation coefficient value was 0.90, indicating excellent internal consistency and test-retest reliability, respectively. No floor (2.6%) or ceiling effect (1.0%) was observed. The HSS Pedi-FABS was significantly correlated with the PAQ-C (r = 0.70). The active group demonstrated a significantly higher score on the HSS Pedi-FABS (mean = 18.9) than did the inactive group (mean = 11.2). In terms of discriminative validity, the HSS Pedi-FABS was not correlated with body mass index (r = –0.15).
Conclusion:
The Japanese version of the HSS Pedi-FABS demonstrated appropriate reliability and validity, indicating that it is a useful tool to assess physical activity levels in Japanese children.
Continued surveillance of objective physical fitness measurements in Japan has revealed that children’s physical fitness and daily exercise are declining. 14 Physical inactivity in childhood can lead to obesity and lifestyle-related diseases in adulthood. 6,13,21 Therefore, healthy physical activity from an early age is recommended. However, excessive sports participation increases the risk of overuse and acute traumatic injury. 10 Therefore, a detailed assessment of children’s physical activity level is critical for preventing lifestyle-related diseases and maintaining sports participation.
Accelerometers are used worldwide for the direct assessment of activity. However, issues regarding adherence and high cost of these devices make their use in population-based studies challenging. In contrast, self-administered questionnaires are affordable, simple, and easy to use. Additionally, their administration does not require any specialized staff or devices, so a large sample of children can be surveyed in a short time. Although many scores are available for assessing physical activity in adults, only a few scores exist for children. An optimal tool that is reliable and valid should be selected to assess a child’s level of physical activity because the application of an adult score for children yields unreliable results. 12 The few scales used to measure a broader range of functional activity are time-consuming and limited to specific sports or joints. 11,16 Although the Physical Activity Questionnaire for Older Children (PAQ-C) and the World Health Organization’s Health Behavior in School-aged Children survey (HBSC) are well known and used worldwide, 2,4,11,23 these scoring systems are not perfect because of their complexity.
The Hospital for Special Surgery Pediatric Functional Activity Brief Scale (HSS Pedi-FABS) is a scoring tool specifically designed to quantify physical activity levels in children independent of specific sports participation. 7 The HSS Pedi-FABS asks 8 simple questions, and its reliability has been validated. 7 As well, it has been translated into several languages. 1,17 Recently, it was adopted as the primary outcome measure of the Pediatric Anterior Cruciate Ligament Monitoring Initiative, and it has been used worldwide. 19 However, no validated Japanese version of this scoring tool is available.
In this study, we aimed to translate the HSS Pedi-FABS into Japanese and assess its reliability and validity. We hypothesized that our Japanese version of the HSS Pedi-FABS would demonstrate good reliability and validity, similar to versions in other languages.
Methods
Translation of the HSS Pedi-FABS From English to Japanese
Translation into Japanese was carried out according to the method described in previous reports. 9,22 First, we contacted the original author to confirm that the HSS Pedi-FABS had not been translated into Japanese, and we obtained permission to use it. Then, the original HSS Pedi-FABS (Appendix 1) was translated into Japanese by a native Japanese speaker who was fluent in English (Appendix 2). Due to cultural differences, some wording needed to be revised. For example, in the competition section, we translated “competition without an official or judge” as “play” because the term pickup games is not familiar to Japanese children. The revised items were reviewed by elementary and junior high school teachers and by researchers to ensure that the wording was appropriate for the Japanese cultural environment. Next, back-translation was conducted by a native English speaker who was fluent in Japanese. The original author then checked the back-translated the HSS Pedi-FABS to ensure that the questions’ original meaning was preserved.
The translated HSS Pedi-FABS (Appendix 2) was tested in a pilot study involving 40 Japanese children (age range, 9-15 years) to determine whether they fully understood all items and whether they had problems understanding the meaning of each item’s phrases.
Data Collection
In the current study, 835 children aged 9 to 15 years were enrolled from elementary and junior high schools affiliated with Chiba University. A total of 65 participants who did not complete the measurement in the first or second assessment were excluded. Additionally, we excluded 6 participants who did not undergo periodic health checkups and whose height and weight data were unavailable. The final sample size was 764 children (Figure 1). The study protocol was approved by our ethics committee, and informed consent was obtained from all parents and participants.
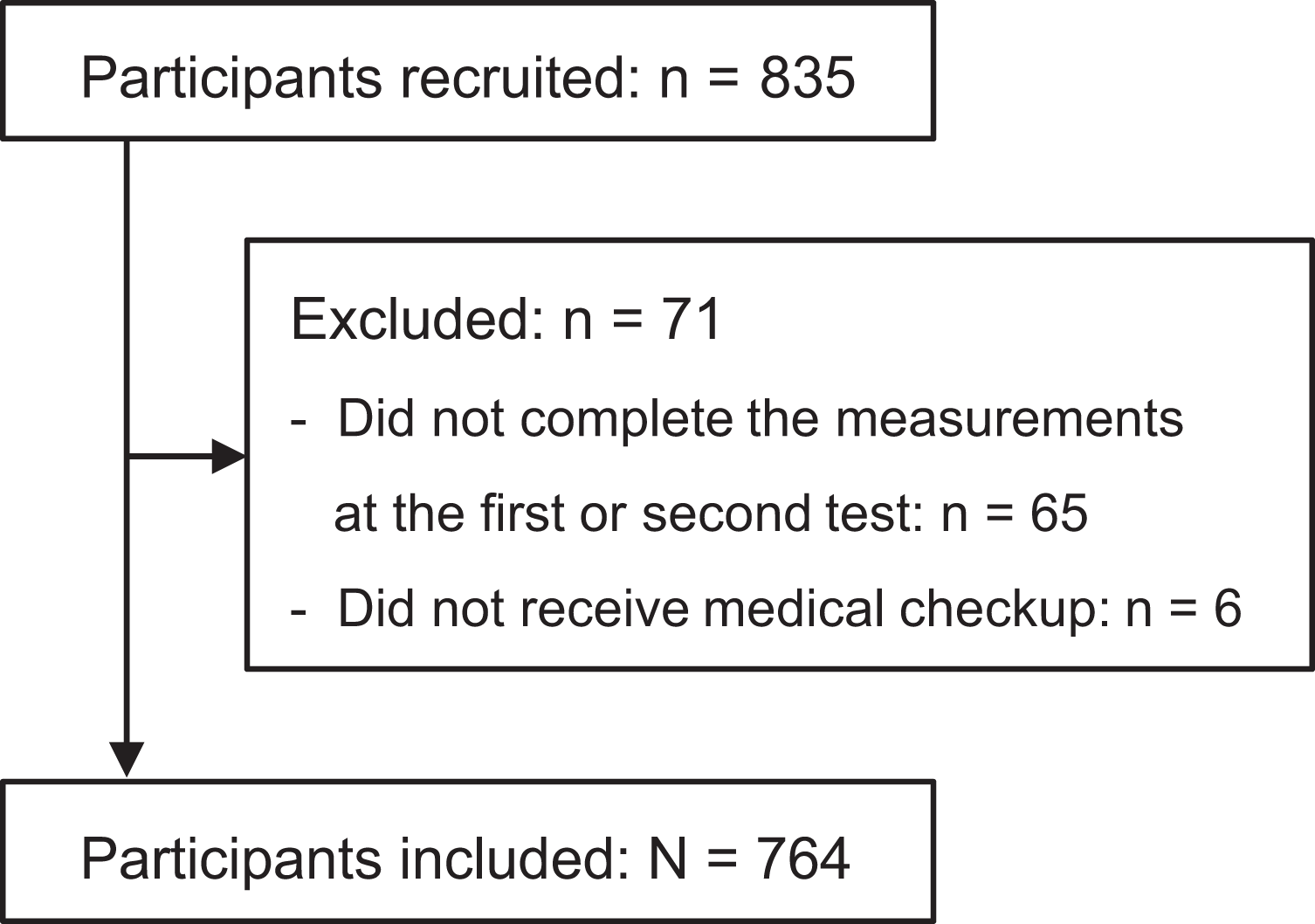
Flowchart of participants included in the validation analysis.
Procedures
Participants answered the Japanese version of the HSS Pedi-FABS, along with 2 other questionnaires in Japanese for convergent validity testing: the PAQ-C 11 and the physical activity questionnaire of the HBSC (HBSC PAQ). 2,23 To calculate body mass index (BMI), we obtained participants’ height and weight from health checkups performed within 1 month of the survey. At 1 month after the first assessment, the children answered the Japanese version of the HSS Pedi-FABS again so we could determine test-retest reliability. The interval between the first and second assessments was set to 1 month so we could conduct both assessments in the same physical setting as much as possible, with minimum changes in school activity status between assessments.
Assessments
Each score was assessed as described next.
HSS Pedi-FABS
Scoring of the HSS Pedi-FABS is performed by assigning points to each question as indicated in Appendix 2. For questions regarding running, cutting, decelerating, pivoting, duration, and endurance, each question is given a score ranging from 0 to 4 points. For the questions regarding competition and supervision, each question is given a score ranging from 0 to 3 points, identical to the original English-language version of the scale. 7 The total score ranges from 0 to 30, with higher scores indicating higher physical activity levels.
Physical Activity Questionnaire for Older Children
The PAQ-C is a self-administered questionnaire that is used to assess the physical activity level in the previous 7 days of children aged 8 to 14 years. The PAQ-C score was calculated as the mean score of 9 items, each scored from 1 to 5, with higher scores indicating higher physical activity levels. 4,11
Physical Activity Questionnaire of HBSC
The HBSC PAQ is used to assess the frequency and duration of physical activity in the previous 7 days. The questionnaire consists of 2 items: frequency and duration. It explicitly categorizes both frequency and duration into 6 levels representing varied levels of physical activity engagement from low (inactive) to high (active).
Participants who answered “2 to 3 times a week” or more for the frequency item and “about 1 hour a week” or more for the duration item on the HBSC PAQ were placed into an active group, whereas the remaining participants were placed into an inactive group. 2,23
Statistical Analysis
Data were analyzed using the BellCurve for Excel (Social Survey Research Information Co Ltd). Mann-Whitney U test was used to analyze nonparametric variables such as age, height, weight, BMI, PAQ-C score, and HHS Pedi-FABS score between male and female participants.
To assess reliability, we calculated internal consistency using the Cronbach alpha, 5 and test-retest reliability was assessed using the intraclass correlation coefficient (ICC). 18 Floor and ceiling effects were assessed by determining the percentage of respondents with minimum and maximum scores, respectively, with ≥15% of either indicating that a floor and/or ceiling effect was present. 24 To assess convergent validity, we evaluated correlations between the HSS Pedi-FABS and the PAQ-C using the Pearson correlation coefficient. HSS Pedi-FABS scores between the HBSC PAQ active and inactive groups were assessed using Mann-Whitney U test. The Pearson correlation coefficient between HSS Pedi-FABS score and BMI was evaluated to assess discriminant validity.
Results
The characteristics of the participants and obtained scores are summarized in Table 1.
Characteristics of the Participants a

a Data are expressed as mean ± SD or No. of participants. BMI, body mass index; HBSC PAQ, Health Behavior in School-aged Children–physical activity questionnaire; HSS Pedi-FABS, Hospital for Special Surgery Pediatric Functional Activity Brief Scale; PAQ-C, Physical Activity Questionnaire for Older Children.
Japanese HSS Pedi-FABS scores were slightly but significantly higher in male participants than in female participants (mean ± SEM: male = 16.7 ± 0.42, female = 13.2 ± 0.38; P < .001), as were PAQ-C scores (mean ± SEM: male = 2.74 ± 0.04, female = 2.48 ± 0.038; P < .001). Distributions of HSS Pedi-FABS scores in the first and second assessments are shown in Figure 2.

Histograms demonstrating the proportion of the Japanese version of the Hospital for Special Surgery Pediatric Functional Activity Brief Scale (HSS Pedi-FABS) scores in the first and second assessments, which were administered 1 month apart.
Reliability
The Cronbach alpha coefficient for internal consistency was .90, indicating excellent internal consistency. For test-retest reliability, the ICC value was 0.90 (95% CI, 0.89-0.92), indicating excellent reliability (P < .001).
Validity
No significant floor effect (2.6.%) or ceiling effect (1.0%) was observed. In assessments for convergent validity, the Japanese version of the HSS Pedi-FABS was significantly correlated with the Japanese version of the PAQ-C (r = 0.70; P < .001) (Figure 3A). The active group demonstrated a significantly higher score on the Japanese version of the HSS Pedi-FABS (mean ± SEM, 18.9 ± 0.34) compared with the inactive group (mean ± SEM, 11.2 ± 0.38; P < .001) (Figure 3B). In discriminant validity testing, the Japanese version of the HSS Pedi-FABS was appropriately not correlated with BMI (r = –0.15; P < .001) (Figure 3C).

(A) Distributions of HSS Pedi-FABS and PAQ-C scores. The HSS Pedi-FABS was significantly correlated with the PAQ-C. (B) Mean HSS Pedi-FABS scores in the Japanese versions of the HBSC PAQ active and inactive groups. The active group demonstrated a significantly higher score on the HSS Pedi-FABS compared with the inactive group (P < .01). Error bars indicate SDs. (C) Distribution of the HSS Pedi-FABS and BMI. The Japanese version of the HSS Pedi-FABS was not correlated with BMI. BMI, body mass index; HBSC PAQ, Health Behavior in School-aged Children–physical activity questionnaire; HSS Pedi-FABS, Hospital for Special Surgery Pediatric Functional Activity Brief Scale; PAQ-C, Physical Activity Questionnaire for Older Children.
Discussion
In the present study, we developed a Japanese version of the HSS Pedi-FABS and assessed its reliability and validity by administering it to 764 students aged 9 to 15 years. The mean HSS Pedi-FABS score was slightly (3.5 points) but statistically significantly higher (P < .001) in male participants than in female participants, which is consistent with previous reports of the English version demonstrating a small difference of 2.4 points. 7,8,11 In the current study, internal consistency, test-retest reliability, and construct validity (both convergent and discriminant validity) were acceptable for the Japanese version of the HSS Pedi-FABS.
The PAQ-C and the World Health Organization’s HBSC are well-known scores for assessment of physical activity in children. In the Global Matrix 2.0, an international comparison of physical activity among children and adolescents in 38 countries, the HBSC was the most commonly used scoring tool to assess physical activity. 25 The PAQ-C was also used extensively in the same survey and was used to validate the original HSS Pedi-FABS. 7 Both have been translated into Japanese and validated. However, each score has several limitations, so we adopted both scores for assessment. The PAQ-C contains 39 items and may take a long time to answer, possibly resulting in inaccurate answers from children due to questionnaire fatigue. The HBSC PAQ has only 2 questions and is difficult to score as a continuous variable. The HSS Pedi-FABS consists of 8 simple questions and is scored from 0 to 30, which is sufficient for analysis as a continuous variable. Although the PAQ-C considers the frequency of each sport activity, it does not take into account the type of movement, which may affect the injury incidence. For example, a child who swims every day and a child who plays soccer every day would both receive the same scores, but it could be assumed that these 2 children would have different injury risk profiles. In contrast, HSS Pedi-FABS scores the frequency of activity according to the type of movement (eg, running, cutting, decelerating, pivoting), duration, and competitiveness. Therefore, the HSS Pedi-FABS can be expected to detect the effect of different types and intensity of sports activity.
In this study, male participants scored slightly higher than female participants on both the HSS Pedi-FABS and the PAQ-C. In Japan, school-aged boys tend to be more active than girls, as the Japanese Sports Agency reported that 75% of boys belong to an athletic club in Japanese junior high school compared with only 50% of girls. 15 This result indicates the more frequent opportunities for physical activity for boys than girls. Previous reports in Japan showed higher physical activity levels and PAQ-C scores in male participants, consistent with the present study. 11,23
The HSS Pedi-FABS has been translated into several languages, and each version has demonstrated acceptable reliability (English: ICC = 0.91, α = .91; Italian: ICC = 0.94, α = .93; French: α = .87). 1,7,17 The current study demonstrated comparable results for the Japanese version of the HSS Pedi-FABS. Furthermore, no floor or ceiling effect was found in the Japanese version, similar to other language versions (floor/ceiling: English, 0%/3.9%; Italian, 19%/0%; French, 2.3%/7.0%). 1,7,17
In convergent and discriminant validity assessments, all expected relationships were demonstrated. Although a significant relationship was found between the HSS Pedi-FABS and the PAQ-C, the HSS Pedi-FABS score was not associated with BMI. The relationship between physical activity and BMI remains controversial. In American children of European descent, BMI was significantly associated with the PAQ-C. 20 However, previous studies on children in Japan reported that BMI was not related to self-reported physical activity or PAQ-C. 3,11 In the Japanese pediatric population, BMI can be irrelevant to physical activity. From these results, we were able to demonstrate good reliability of the Japanese version of the HSS Pedi-FABS.
Limitations
This study had several limitations. First, direct physical activity assessment using an accelerometer was not conducted in this large cohort of children because we considered it unfeasible for all children to appropriately wear the accelerometer during the study period. Second, the data were collected from only 2 schools, both of which are affiliated with Chiba University, and this could have caused selection bias in the participants. Further evaluation including children from more diverse schools may cause a slight difference in the results. However, considering the large number of children included in this study, our results could be applied to other Japanese cohorts of the same age. Third, we performed the study under the assumption that the activity status of the children would not change significantly within the 1-month interval before the retest. Some changes that would affect physical activity levels, such as injuries and family situations, could have occurred. However, the test-retest results were good, and we considered there were no major issues in the data for analysis.
A final limitation was that we conducted this study during the coronavirus disease 2019 pandemic. During the study, schools in Japan had just resumed physical activities, including gymnasium classes and athletic club activities. Thus, the obtained results may be different from those obtained under normal conditions. However, the current mean PAQ-C score (2.6 ± 0.79) was not significantly different from that previously reported in Japan (2.76 ± 0.69). 11 Although direct comparison is difficult, the currently obtained HSS Pedi-FABS score (15.0 ± 8.0) was comparable with that obtained in the United States (15.4 ± 8.5). 8 Thus, the validity of the Japanese version of the HSS Pedi-FABS is likely applicable to conditions outside of those experienced during coronavirus disease 2019. Further surveillance is needed to confirm our results after the situation has normalized.
Conclusion
In the current study, the Japanese version of the HSS Pedi-FABS demonstrated good reliability and validity, thus making it a valuable assessment tool for physical activity among Japanese children.
Footnotes
Acknowledgement
The authors appreciate the assistance from the teachers and school nurses of the Chiba University Elementary and Secondary Schools, the physical therapists for their support in data collection, and Yumi Akagi for data management.
Final revision submitted February 16, 2022; accepted May 11, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by Pfizer Global Medical Grants (grant 43802135). AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Chiba University (approval No. 3959).