
Abstract
Background:
Although anterior apophyseal abnormalities of the vertebrae and spondylolytic spondylolisthesis (SS) are prevalent in gymnasts during growth spurts, no studies have examined the relationship between apophyseal abnormalities and SS.
Hypothesis:
A significant relationship will exist between anterior apophyseal abnormalities and SS in young gymnasts.
Study Design:
Cohort study; Level of evidence, 2.
Methods:
A total of 306 gymnasts (123 male, 183 female; age range, 6-28 years) with >2 weeks of back pain were enrolled in this study. Apophyseal abnormalities were evaluated using radiography. In the primary analysis, multiple logistic regression analysis was performed to assess the odds ratio (OR) for multivariate factors (age, body mass index, sex, skeletal maturity, competitive level, and presence of spondylolysis or SS) influencing the incidence of apophyseal abnormalities. In the secondary analysis, 90 of the 306 gymnasts were followed up radiographically for a minimum of 2 years, and factors contributing to the worsening of apophyseal abnormalities were identified.
Results:
In the primary analysis, the chi-square test revealed a relationship between anterior ring apophyseal abnormalities and SS at the L5-S1 segment (OR, 7.6). Multiple logistic regression analysis demonstrated that the presence of SS at L5-S1 (OR, 9.5) and competitive level (international: OR, 6.7; national: OR, 4.5) correlated with the incidence of apophyseal abnormalities. The secondary analysis identified the presence of SS at L5-S1 (OR, 5.9) as a significant factor contributing to the worsening of apophyseal abnormalities.
Conclusion:
The presence of SS was a factor affecting the incidence and prognosis of anterior apophyseal abnormalities.
The vertebral ring apophysis, which is separated from the vertebral body by a cartilaginous layer, calcifies at approximately 6 years of age, begins to ossify at approximately 13 years, and begins to fuse with its vertebral body at approximately 17 years. 4 Before complete ossification of the ring apophysis, this osteocartilaginous junction is a relatively weak point, 1 and repetitive trauma or overloading of the spine may cause ring apophyseal abnormalities. 11,17
Apophyseal abnormalities of the vertebrae include marginal Schmorl nodes or sequelae from these nodes, 2,19 and abnormalities affecting the anterior part of the thoracolumbar spine during growth spurts are more prevalent in gymnasts, wrestlers, and skiers. 11,17,20 Anterior apophyseal abnormalities are more common from the thoracolumbar junction to the lumbosacral vertebrae. At the thoracolumbar junction of the spine, forward flexion theoretically increases the risk of injuries to anterior parts of the vertebrae because of compression. 17,21 In the lumbar spine, the opposite conditions are encountered; dorsal extension increases the risk of traction injuries in the anterior parts of the vertebrae. 4,21 Anterior apophyseal abnormalities also have negative effects on the growing athlete, such as back pain, disc degeneration, and poor spinal alignment. 16,19,20 In gymnasts, the level of competition, training periods, and training hours per week have been shown to contribute to the occurrence of these abnormalities. 9,16,22 Each gymnastics event consists of a combination of a number of several techniques. Athletes spend a lot of time practicing to master them, but once they develop back problems, they may not be able to fully perform their daily exercises. As a result, the acquisition of skills can be severely affected. Therefore, there is an urgent need to control the occurrence and progression of anterior apophyseal abnormalities.
Spondylolysis is generally considered to result from repetitive stress to the pars interarticularis. 7 In gymnasts, spondylolysis most likely results from repetitive flexion and extension of the spine at extreme ranges of motion, in addition to twisting maneuvers. The vast majority of lesions, up to 95%, occur at the L5 vertebra. 10 Spondylolysis sometimes progresses to spondylolytic spondylolisthesis (SS) in young athletes. A previous study suggested a relationship between apophyseal abnormalities and SS. 13 However, longitudinal cohort studies that focus on a single sport have not yet been conducted.
The purpose of the present study was to investigate the factors influencing the incidence and prognosis of anterior apophyseal abnormalities in young gymnasts. We hypothesized that SS would be associated with the incidence and prognosis of anterior apophyseal abnormalities in young gymnasts.
Methods
Participants
Between 2005 and 2019, a consecutive series of 380 gymnasts with >2 weeks of back pain were enrolled in the present study. Among the cohort, 306 gymnasts (123 male, 183 female; age range, 6-28 years) met the inclusion criteria for the primary analysis, which were as follows: (1) complete radiographic examination of the lumbar spine at the first visit and (2) complete demographic data. We excluded athletes who (1) were recreational gymnasts or (2) had undergone any type of lumbar surgery (3) with incomplete data.
A secondary longitudinal analysis was conducted in 90 of the 306 gymnasts who met the following inclusion criteria: (1) minimum 2-year radiographic follow-up and (2) demographic data essential to perform secondary analysis. We excluded athletes who (1) were retired from gymnastics competitions or (2) had undergone any type of lumbar surgery within 2 years of the first visit (3) with incomplete data. A study flowchart is shown in Figure 1. All patients provided informed consent for study participation. The present study was approved by the institutional review board of our hospital.

Flowchart of gymnasts who met inclusion and exclusion criteria for the present study.
Collection and Processing of Data
The following information was obtained from medical records and imaging: age, body mass index (BMI), training hours per week, level of competition, skeletal maturity, and lateral view of lumbar vertebrae on plane radiography; all data were recorded at the time of the first visit. The competitive level of each athlete was categorized as one of the following: international, national, and district. 23
Skeletal maturity was assessed using lateral radiographs and divided into 3 stages based on the appearance of the ring apophyses of the L3 vertebra: (1) cartilaginous stage (absence of ring apophyses), (2) apophyseal stage (appearance of ring apophyses), and (3) epiphyseal stage (ossification of ring apophyses). 13 Participant demographics are summarized in Table 1. Radiographs at the final evaluation point were collected and used in the secondary longitudinal analysis.
Participant Characteristics at First Visit (N = 306) a

a Data are shown as mean (95% CI) or No. BMI, body mass index.
Radiographic Examination
Apophyseal abnormalities were defined as follows: (1) excavation of the apophyseal region, (2) excavation of the apophyseal region with a persistent apophysis, (3) a persistent apophysis, and (4) enlargement of the apophyseal region. 21 In the present study, we investigated abnormalities affecting the anterior part of the vertebrae that may be clinically problematic. 16,19,20 Regarding morphological changes to lesions during the follow-up period, we focused on the shape of the vertebral body at the involved site. To adjust for individual vertebral sizes and magnification effects, the relative depth (or severity) of the lesion was calculated as a percentage of the vertebral body height (ratio between the depth of the lesion and vertebral height × 100) in the lateral view. 17 An increase in this ratio at the final evaluation was defined as worsening, while a decrease was defined as an improvement; therefore, changes in the ratio were classified into 2 groups: (1) worsening and (2) improvement or no changes.
Spondylolytic defects were diagnosed using standard anteroposterior and lateral radiographs of the lumbar spine. The percentage of the slip was measured on lateral radiographs using the methods of Wiltse and Winter. 25 SS was defined as vertebral slippage of >5%. 13
All radiographs were evaluated by 2 spine surgeons (M.U. and A.K.). Any discrepancies in the evaluation of radiographic findings between the surgeons were reviewed between them, and a final decision was reached.
Statistical Analysis
Our primary analysis was cross-sectional, and our secondary analysis was longitudinal. Before statistical analysis, quantitative data, such as age, BMI, and practice volume at the first visit, were categorized to acquire an equal distribution.
In the primary analysis (N = 306), the spinal segment below the spondylolytic defect was defined as the involved segment, and we investigated the relationship between spondylolysis or SS and apophyseal abnormalities at the involved segment using the chi-square test. Multiple logistic regression analysis was used to assess the odds ratio (OR) for multivariate factors affecting the incidence of apophyseal abnormalities at the L5-S1 segment. Independent variables were as follows: age, BMI, sex, practice volume, skeletal maturity, competitive level, and presence of spondylolysis or SS.
In the secondary analysis (n = 90), multiple logistic regression analysis was conducted to identify the factors influencing the worsening of apophyseal abnormalities at the L5-S1 segment. Independent variables were as follows: age, BMI, sex, skeletal maturity, competitive level, and presence of spondylolysis or SS. Data on practice volume could not be followed over time in many participants, so it was excluded from the independent variables.
Confounders were selected as appropriate, and the multicollinearity of each independent variable was assessed by calculating each correlation before analysis. The goodness of fit for each final estimate was assessed using the Hosmer-Lemeshow test. 12 All analyses were performed using SPSS for Macintosh (Version 21; IBM). Differences were considered to be significant at P < .05.
Results
Primary Analysis
Anterior apophyseal abnormalities were observed in 92 vertebrae of 84 patients (27%) at the following segments: L1-2 (n = 20), L2-3 (n = 11), L3-4 (n = 10), L4-5 (n = 24), and L5-S1 (n = 27), with the L5-S1 segment being the most commonly affected. Spondylolysis was detected at L1-2 (n = 1), L2-3 (n = 6), L3-4 (n = 18), L4-5 (n = 33), and L5-6 (n = 46), while SS was identified at L1-2 (n = 0), L2-3 (n = 0), L3-4 (n = 2), L4-5 (n = 1), and L5-6 (n = 26).
The chi-square test revealed a relationship between anterior ring apophyseal abnormalities and SS at the L5-S1 segment (OR, 7.6; P < .001). On the other hand, the chi-square test did not reveal a relationship between anterior ring apophyseal abnormalities and spondylolysis at any vertebral segments. Among the 27 cases with apophyseal abnormalities occurring at the L5-S1 segment, 8 were at the same vertebral segment as SS. The remaining 19 cases did not have SS. In contrast, among the 26 cases of SS occurring at the L5-S1 segment, 8 were at the same vertebral segment as apophyseal abnormalities. The remaining 18 cases did not have apophyseal abnormalities (Table 2).
Relationship Between Apophyseal Abnormalities and Spondylolysis and SS a

a Boldface P value indicates statistical significance (P < .05). NE, not estimated; OR, odds ratio; SS, spondylolytic spondylolisthesis.
b Except 8 cases with SS.
c Except 6 cases with Spondylolysis.
Multiple logistic regression analysis demonstrated that the presence of SS at L5-S1 (OR, 9.5; P < .001) and competitive level (international: OR, 6.7; P = .04) (national: OR, 4.5; P = .02) correlated with the incidence of apophyseal abnormalities (Table 3).
Factors Influencing the Incidence of Apophyseal Abnormalities a

a Boldface P values indicate statistical significance (P < .05). BMI, body mass index; NA, not applicable; OR, odds ratio; SS, spondylolytic spondylolisthesis.
b Adjusted by age and BMI.
Secondary Analysis
The 90 patients included in the secondary analysis had a mean follow-up of 39.9 months (range, 24-132 months). In 8 patients, apophyseal abnormalities were not observed at the L5-S1 segment at the initial visit but were detected in the final evaluation. Also, 3 patients had apophyseal abnormalities at the first visit that had worsened by the final evaluation (Figure 2). These 11 cases were included in the worsening group, and factors affecting the worsening group were examined using logistic analysis. The results obtained identified the presence of SS at L5-S1 as a significant factor (OR, 5.9; P = .03) (Table 4).
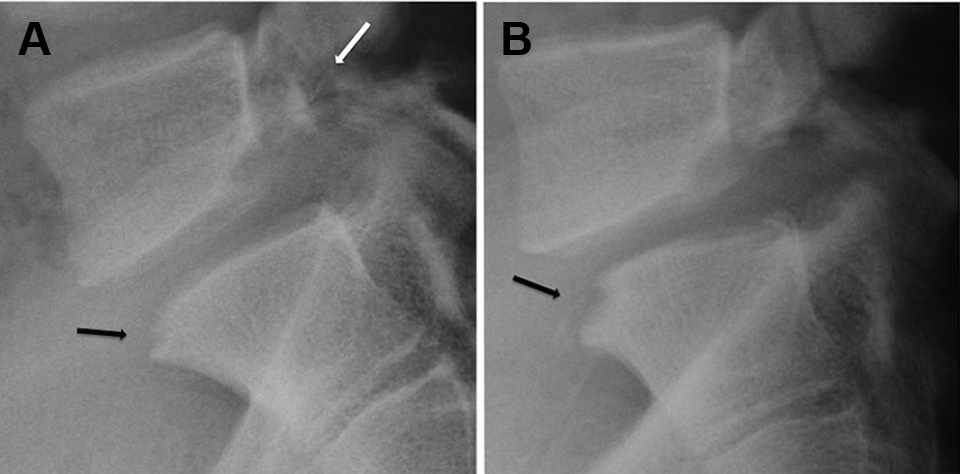
Lateral radiographs from a 15-year-old male gymnast. (A) Radiograph obtained at the initial visit shows spondylolytic spondylolisthesis at L5 (white arrow) and excavation of the apophyseal region at the upper anterior corner of S1 (black arrow). (B) Follow-up radiograph obtained in the final evaluation at 26 months after the initial visit shows an increase in the size of excavation at S1 (black arrow).
Factors Influencing the Prognosis of Apophyseal Abnormalities a
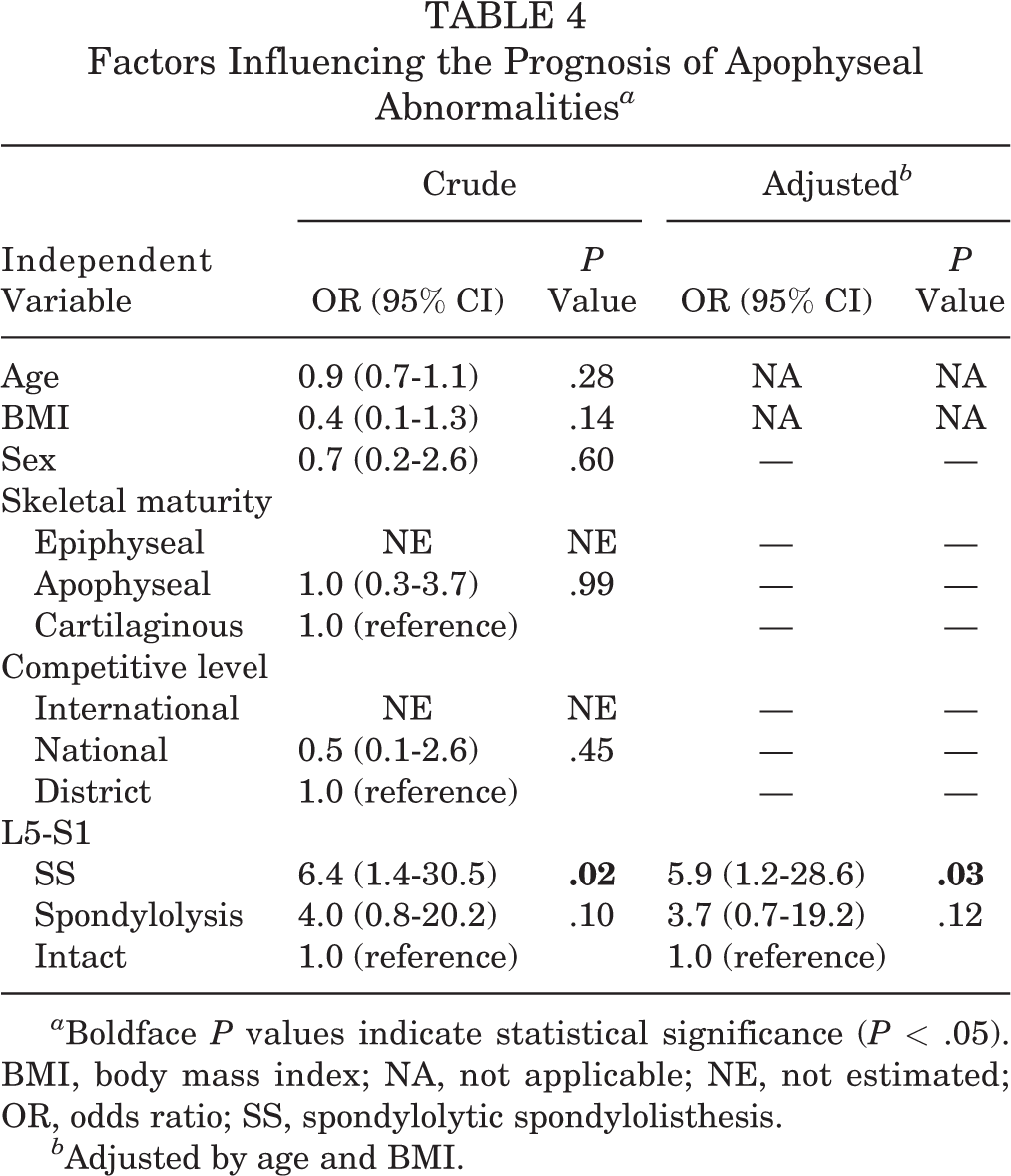
a Boldface P values indicate statistical significance (P < .05). BMI, body mass index; NA, not applicable; NE, not estimated; OR, odds ratio; SS, spondylolytic spondylolisthesis.
b Adjusted by age and BMI.
Overall, 7 participants showed worsening of apophyseal abnormalities in the final evaluation, even though SS was not present at the first visit or final evaluation. In contrast, even with the presence of SS, 9 cases showed no changes or improvements in the final evaluation, including 1 case in which abnormalities had been repaired. Among the 4 cases with apophyseal abnormalities and no SS at the first visit, none had SS in the final evaluation.
Discussion
Our results showed that the presence of SS and the competitive level of gymnasts were significant factors influencing the incidence of apophyseal abnormalities, while SS was identified as a factor contributing to the progression of these abnormalities. With regard to the competitive level, the results support those of Swärd et al. 21
Mechanisms That May Cause Apophyseal Abnormalities
In the present study, among the 27 cases with apophyseal abnormalities at the L5-S1 segment, 8 had SS at the same vertebral segment, and the chi-square test revealed a relationship between apophyseal abnormalities and SS. The pathogenetic mechanism proposed by Ikata et al 13 may be involved in this result. On the other hand, there were 19 cases in which apophyseal abnormalities occurred without SS, which means that there may be another injury mechanism that does not involve SS. Therefore, we focused on movements unique to gymnastics, which are rare in other sports. Brüggemann 5 reported that during a giant swing on uneven bars or the high bar before a Tkatchev release, shear force at L5-S1 is approximately 4-fold the body weight of a gymnast. Average compressive landing forces at the L5-S1 segment in a gymnast’s spine have been calculated as 11.6- and 14.8-fold their body weight for forward and backward saltos, respectively. Average landing shear forces at the L5-S1 segment have also been calculated as 1.4- and 2.2-fold the body weight of a gymnast for forward and backward saltos, respectively. 5 In other words, L5-S1 of the spine in gymnasts is constantly subjected to large shear and compressive forces, and these biomechanical properties may be associated with apophyseal abnormalities.
Factors Influencing the Incidence and Prognosis of Apophyseal Abnormalities
The results of the chi-square test demonstrated a relationship between apophyseal abnormalities and SS. Logistic regression analysis in cross-sectional studies identified the presence of SS as a significant factor associated with the incidence of anterior ring apophyseal abnormalities (Table 3). These findings suggest that the presence of SS is associated with the incidence of apophyseal abnormalities. However, their causal relationship remains unknown. In the longitudinal analysis, of the 4 cases in which apophyseal abnormalities were observed without SS at the first visit, none had SS in the final evaluation. Therefore, this result was negative for the possibility that apophyseal abnormalities influenced the incidence of SS.
The incidence and severity of injuries increase in high-level gymnastics. 8,24 The rate of overuse injuries is higher than that of acute injuries as gymnasts progress to higher levels of competition because of the increased hours, intensity, and repetition of movements needed to perfect more complex skills. 6,14,15 Low back and wrist injuries occur more frequently from overuse than ankle injuries, which are generally acute. 6 Previous studies on anterior ring apophyseal abnormalities mainly focused on elite gymnasts who participated in international competitions or belonged to national teams. 3,11,19,20 The present study targeted a wide range of levels from international to district, and a high level of competition appeared to be a significant factor contributing to the incidence of apophyseal abnormalities.
On the other hand, competitive level was not associated with the progression of apophyseal abnormalities. In the secondary analysis, only 2 patients at the international level were included, and the observation period was ≥2 years; the small number of participants and the short observation period may have affected the results.
In the longitudinal arm of the study, the results of multiple logistic regression analysis suggested that SS affected the progression of apophyseal abnormalities. On the other hand, 7 of 90 gymnasts had worsening of apophyseal abnormalities at L5-S1 in the final evaluation, even though SS was not present at the first visit or final evaluation. In contrast, even with the presence of SS, 9 cases showed no changes or improvements in the final evaluation. These results suggest that factors other than those examined in the present study are influencing the prognosis of these abnormalities. Various factors such as longer training periods, 22 intensive training, and competition 17 may be involved in the prognosis of apophyseal abnormalities.
In this study, there was no association between apophyseal abnormalities and age. The study population consisted of a wide age range, from 6 to 28 years, and the incidence of apophyseal abnormalities was found in the age range of 11 to 22 years. Older gymnasts may be more likely to sustain injuries because of more complex and difficult movements and greater accumulated exposure to training. 6 However, in our study, the incidence of apophyseal abnormalities did not increase with age. This study suggests the need to check for these abnormalities when examining growing gymnasts, regardless of age.
BMI was not a risk factor in our study. Richmond et al 18 reported that obese adolescents had a higher risk of sport-related injuries compared with healthy-weight adolescents. Our study population consisted of young gymnasts, and obese athletes were rare. It was possible that this may have affected the results. In addition, the present study indicated that participant sex was not associated with the incidence or progression of apophyseal abnormalities. A previous study found that these abnormalities occurred only in athletes and were most commonly found in female elite gymnasts. 21 The difference is that their participants were all elite athletes, while our study included nonelite athletes, and this may have influenced the results.
There was no relationship between skeletal maturity and the incidence and prognosis of apophyseal abnormalities. Baranto et al 2 reported in their 15-year follow-up magnetic resonance imaging (MRI) study that most of the spinal abnormalities in athletes seem to occur during growth spurts, as the majority of the abnormalities demonstrated at follow-up MRI after their sports career were present at baseline. In the present study, the incidence of apophyseal abnormalities in the epiphyseal stage, in which skeletal maturation has been completed, was similar to that in the apophyseal stage (see Table 3), but considering the previous report, it is suggested that this may have been a remnant of abnormalities that occurred during the growth spurt. A long-term radiographic follow-up of the study participants from the cartilage stage to the epiphyseal stage is needed to clarify the relationship between the incidence and progression of apophyseal abnormalities and skeletal maturity.
Limitations
The present study had 3 main limitations. First, although all of the participants in this study presented with low back pain as their primary complaint, we did not address whether the apophyseal abnormalities detected in the patients were symptomatic. While apophyseal abnormalities have been reported as a possible cause of pain, 20 there are no reports on specific physical or imaging findings that can prove abnormalities to be symptomatic. Hence, further studies on the relationship between apophyseal abnormalities and pain are required. Second, difficulties were encountered in assessing small deformations and slight changes in apophyseal regions using plain radiography, and thus, a detailed evaluation was not possible. Furthermore, in cases of spondylolysis, instability may differ depending on the stage, and the effects on the apophysis may also differ; therefore, an evaluation by computed tomography, MRI, or dynamic radiography is required where appropriate. Third, the number of cases that met the criteria in the longitudinal analysis was small, and the follow-up period to evaluate the final morphology of apophyseal abnormalities was too short in some cases. Nevertheless, to the best of our knowledge, the present study is the first to demonstrate a relationship between apophyseal abnormalities and SS in gymnasts, and additional studies are needed to resolve these limitations.
Conclusion
Anterior ring apophyseal abnormalities were observed in 27% of gymnasts who were treated for back pain. A relationship between anterior apophyseal abnormalities and SS was found at the L5-S1 segment. The presence of SS and the competitive level of gymnasts were significant factors influencing the incidence of apophyseal abnormalities, while SS was identified as a factor contributing to the prognosis of these abnormalities. Understanding the risk factors associated with apophyseal morphological changes is important in preventing the occurrence of these changes and in maintaining athlete performance. To accomplish this, a close collaboration between athletes, coaches, athletic trainers, and physicians is essential.
Footnotes
Acknowledgment
The authors thank Yusuke Ueda, Takahiro Sekiguchi, and Takahiro Fujihara for their valuable help with this study.
Final revision submitted August 17, 2022; accepted September 16, 2022.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Funabashi Orthopaedic Hospital (IRB/ERC #2021018).