
Abstract
Study Design:
Case series.
Objectives:
To report the clinical outcomes of the decompression procedure using the microendoscopic discectomy system for the treatment of a separation of lumbar posterior ring apophysis in young active athletes.
Methods:
We retrospectively reviewed 17 cases that underwent the microendoscopic surgery to treat a symptomatic separated lumbar ring apophysis between 2001 and 2014 at our institute or our associated hospital. The cases consisted of 15 males and 2 females, with their ages ranging from 12 to 19 years. The surgeries were performed at total of 18 lumbar levels, including 15 L4/5 and 3 L5/S1 levels. All patients were young athletes. We evaluated the following: (1) the Japanese Orthopaedic Association (JOA) score for low back pain, (2) recovery rates using Hirabayashi’s method, (3) operating time, (4) intraoperative blood loss, (5) perioperative complications, (6) the status of comeback to sports, and (7) the period taken to return to sports.
Results:
The JOA score was improved after the surgery in all cases. Recovery rate was 92.0% ± 8.1%. The mean operating time per level was 89.2 ± 33.3 minutes. The mean intraoperative blood loss per level was 95.3 ± 93.1 mL. A pinhole size dural tear occurred in one case as a perioperative complication. All cases returned to sports. The mean period taken to return to sports was 10.9 ± 3.5 weeks.
Conclusion:
Microendoscopic decompression surgery is useful for treating a separation of lumbar posterior ring apophysis.
Introduction
Separation of the lumbar posterior ring apophysis can be a cause of low back pain and leg pain, as could be experienced with like a lumbar disc herniation. 1 It is an uncommon lesion, which is typically found in young active athletes. It requires careful diagnosis and the selection of the most appropriate surgical option since it can be a formidable barrier to the activities of daily living (ADL). The lesion is generally caused by trauma; the actual condition is a bony fragment at the posterior rim of lumbar vertebral endplate. 2,3 When a conservative treatment is ineffective and surgery is selected, it is considered best to avoid the major surgery such as wide laminectomy and fusion surgery. 3 -13
Microendoscopic discectomy (MED) was developed by Smith and Foley 14 in 1997 and the decompression technique has been one of the useful minimally invasive spine surgeries used in Japan. Using the technique, the authors have carried out more than 3000 cases of lumbar disc herniation and lumbar spinal canal stenosis, 15,16 as well as more than 20 cases of separation of lumbar posterior ring apophysis. Using the technique, the facet joints and posterior stabilizers such as musculatures and ligaments are preserved. This can reduce the risk of the postoperative spinal instability and the future need for fusion surgery. Furthermore, this surgery can allow the young active athletes to start rehabilitation early.
The purposes of this study were (1) to describe the decompression procedure when using the MED system in a case of a separation of lumbar posterior ring apophysis and (2) to report the clinical outcomes in young athletes.
Patients and Methods
Surgical Technique
The patient was placed in the prone position on a laminectomy frame after general anesthesia was induced. The fluoroscopic C-arm was brought into the surgical site and the targeting level was marked under fluoroscopic anterior-posterior guidance. First, the operator stood on the symptomatic side and video monitor was placed on the opposite side of the patient (Figure 1a). An approximately 17-mm median skin incision was created above a spinous process. After the paramedian fasciotomy and finger navigation on the symptomatic side, the paravertebral muscles were split using serial dilators of the METRx endoscopic system (Medtronic Sofamor Danek). The 16-mm tubular retractor was then passed over the dilators and secured to the flexible arm mounted to the table side rail. The oblique-viewing endoscope was attached to the tubular retractor (Figure 1b). The position of the tubular retractor was reconfirmed fluoroscopically after the resection of residual musculatures and soft tissues overlying the lamina and facet joint. All of the following procedures were performed microendoscopically (Figure 1c). With the lamina and facet joint well visualized, a high-speed drill with a long curved endoscopic bar (eg, Midas-Rex: Figure 2b) was used to cut the lamina until exposing the superior and inferior attachments of ligamentum flavum. After the laminotomy, ligamentum flavum was firstly split using ball-tipped probe at the midline to decompress the dural sac; the probe was then removed. The lateral recess on the ipsilateral side was decompressed by using a long curved endoscopic bar and curved Kerrison rongeurs (Figure 2a); this allowed the facet joint to be kept as intact as possible. The outer edge of the nerve root was identified and then gently retracted medially to expose the separated ring apophysis. We used a chisel (usually curved chisel: Figure 2c) to cut the separated ring apophysis (while keeping the nerve root retracted) and removed it piecemeal using a herniotomy rongeur. After the hemostasis and irrigation, the fascia was closed with 2-0 Vicryl (Johnson & Johnson). Next, if a bilateral approach is needed, the operator moved to the opposite side and video monitor was also moved so that the operator can watch it. The residual mass of the separated ring apophysis was removed by the same procedure through the opposite-side approach using a median skin incision. After the hemostasis and irrigation, a drain was placed, and the fascia and the skin were closed in layers with 2-0 Vicryl and Steristrips (3M Company). It is possible to resect the separated ring apophysis completely and safely through this bilateral approach, even if it is a huge mass.
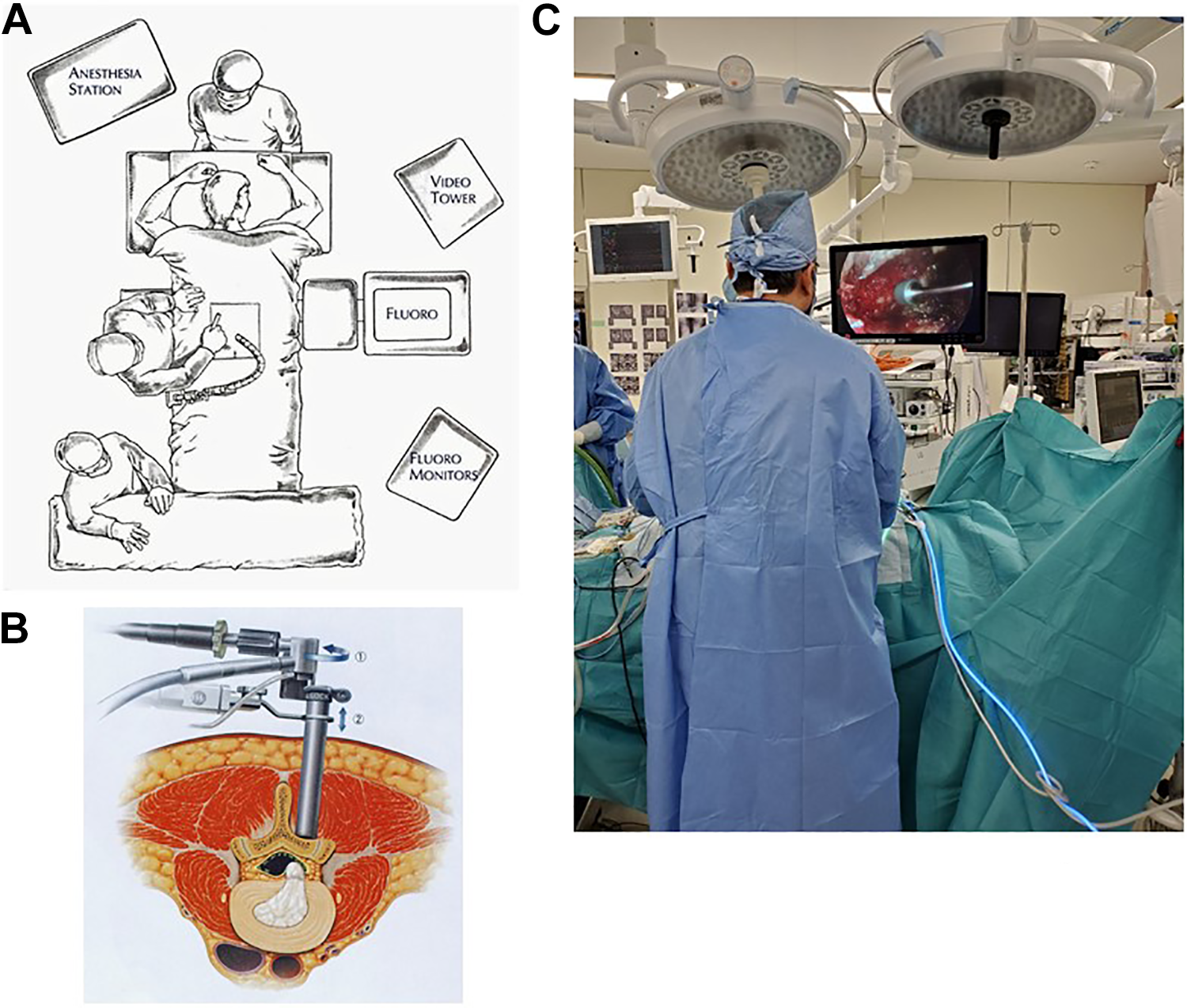
(a) The layout of equipment. (b) METRx endoscopic system with the 16-mm tubular retractor and the oblique-viewing endoscope. (c) Intraoperative landscape.
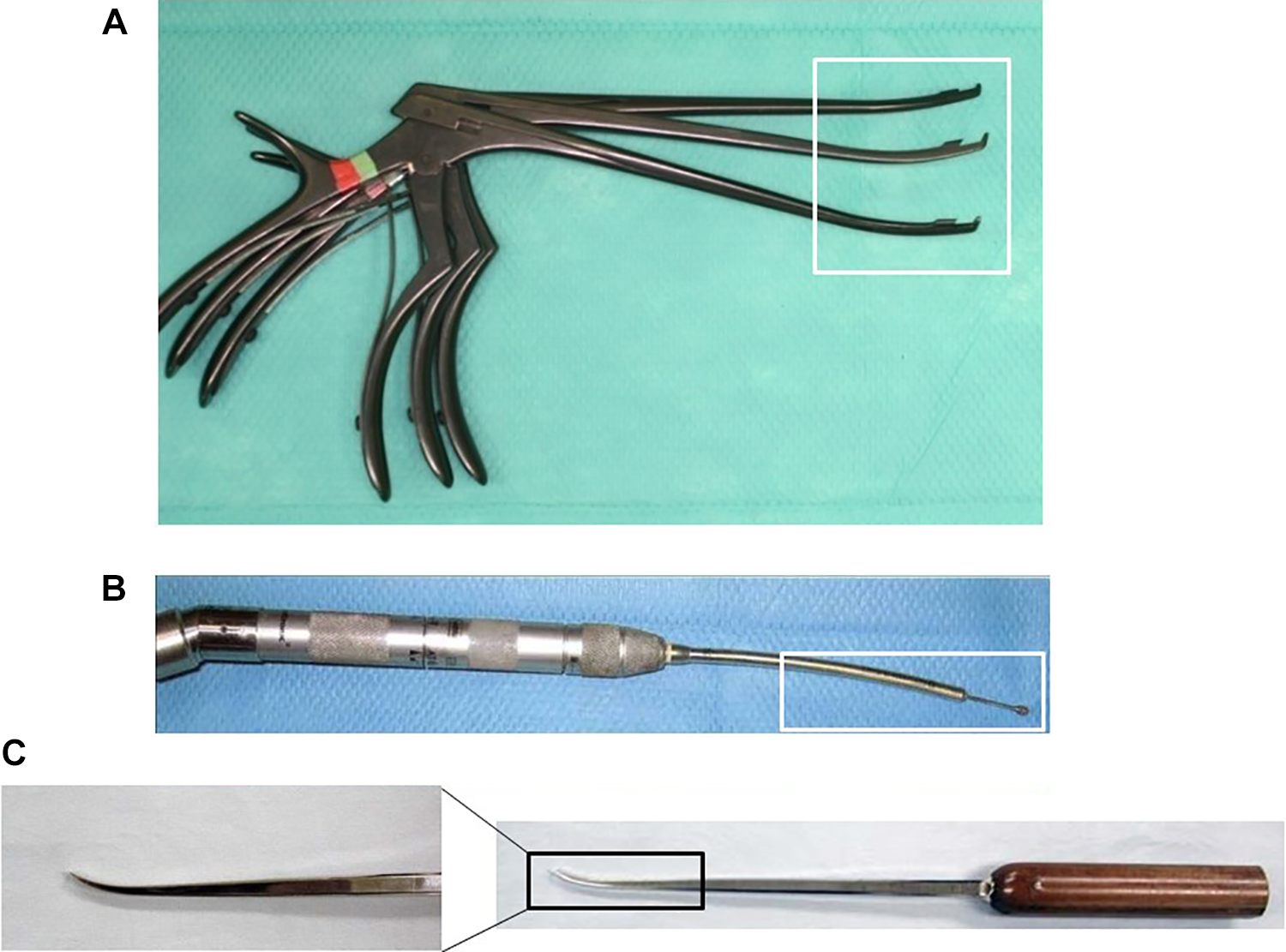
(a) Curved Kerrison rongeurs. (b) A long curved endoscopic bar. (c) A curved chisel.
Patients and Evaluations
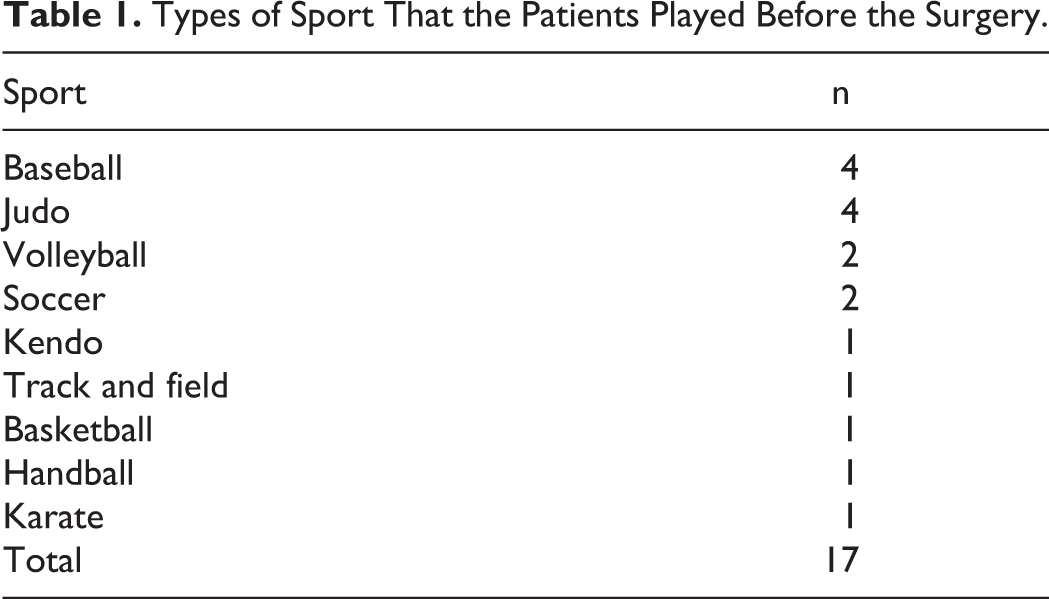
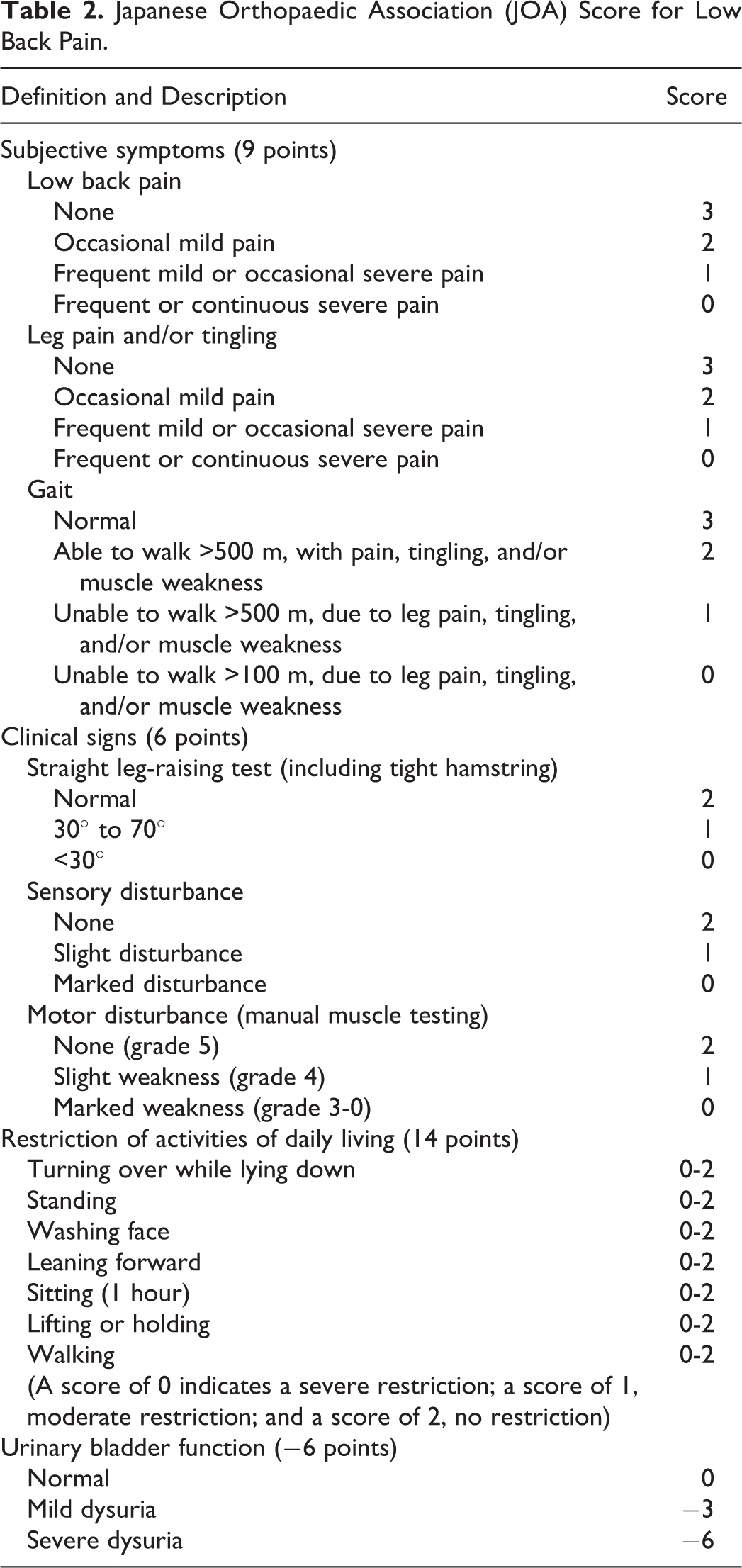
We reviewed retrospectively consecutive 17 cases (between 2001 and 2014) that had undergone the microendoscopic surgery to treat a symptomatic separated lumbar ring apophysis at our institute or our associated hospital. All participants provided informed consent. This study was reviewed and approved by the Ethical Committee for clinical trials at our institute. The cases consisted of 15 males and 2 females, with their ages ranging from 12 to 19 years (mean age: 15.2 years) at the time of the surgery. The surgeries were performed at a total of 18 lumbar levels: 15 L4/5 and 3 L5/S1 levels. One case had the surgery at both of L4/5 and L5/S. Five, 9, and 4 cases were classified into type 1, 2, and 3, respectively, according to Takata’s classification 3 (Figure 3). The follow-up period ranged from 12 to 67 months (average: 23 months). All patients were young athletes as shown in Table 1. The clinical records were analyzed. We evaluated the following: (1) the Japanese Orthopaedic Association (JOA) score for low back pain (Table 2) before surgery and at final follow-up. The scoring system is commonly used in Japan to indicate the severity in lumbar spinal disorders. The total score for a healthy individual is 29. (2) Recovery rates that were calculated at final follow-up using the Hirabayashi’s method: (postoperative JOA score – preoperative JOA score) × 100 / (29 − preoperative JOA score). (3) Operating time. (4) Intraoperative blood loss. (5) Perioperative complications. (6) the status of comeback to sports. (7) The period taken to return to sports.
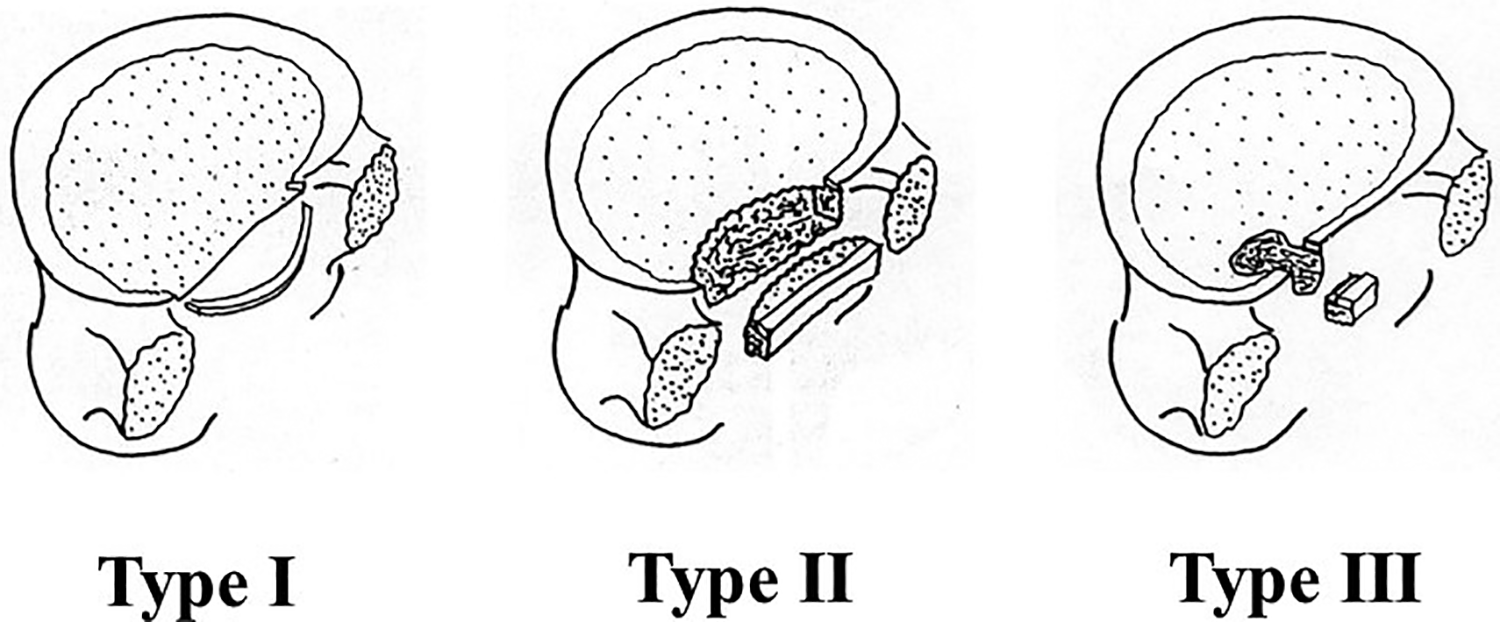
Takata’s classification.
Types of Sport That the Patients Played Before the Surgery.
Japanese Orthopaedic Association (JOA) Score for Low Back Pain.
Results
JOA Score and Recovery Rate
The JOA score was improved after the surgery in all cases. The mean score was 16.2 ± 4.7 points before surgery and 28.1 ± 0.9 points at final follow-up. Recovery rate was 92.0% ± 8.1%.
Operating Time, Intraoperative Blood Loss, and Perioperative Complications
The mean operating time per level was 89.2 ± 33.3 minutes. The operating time was longer in some cases in types 1 and 2 in Takata’s classification because the bilateral approach was required in those cases (2 of 5 cases in type 1, and 7 of 9 cases in type 2). The mean intraoperative blood loss per level was 95.3 ± 93.1 mL. A pinhole size dural tear occurred in one case as a perioperative complication. No neurological deterioration was observed postoperatively.
The Status of Comeback to Sports and the Period Taken to Return to Sports
All cases returned to sports. The mean period taken to return to sports was 10.9 ± 3.5 weeks after the surgery.
Case Presentation
A 15-year-old male Judo wrestler consulted our institute with left-side leg pain after the Judo lessons. Physical examination revealed positive tension sign such as “straight leg raising” test, motor weakness at his muscles of tibialis anterior and extensor hallucis longus, and hypesthesia at his left-side L5 distribution. The JOA score was 20 out of 29 points.
Plain radiograph and computed tomography showed the separated ring apophysis at L4-5. Magnetic resonance imaging revealed that the left L5 nerve root and dural sac were being compressed (Figure 4).
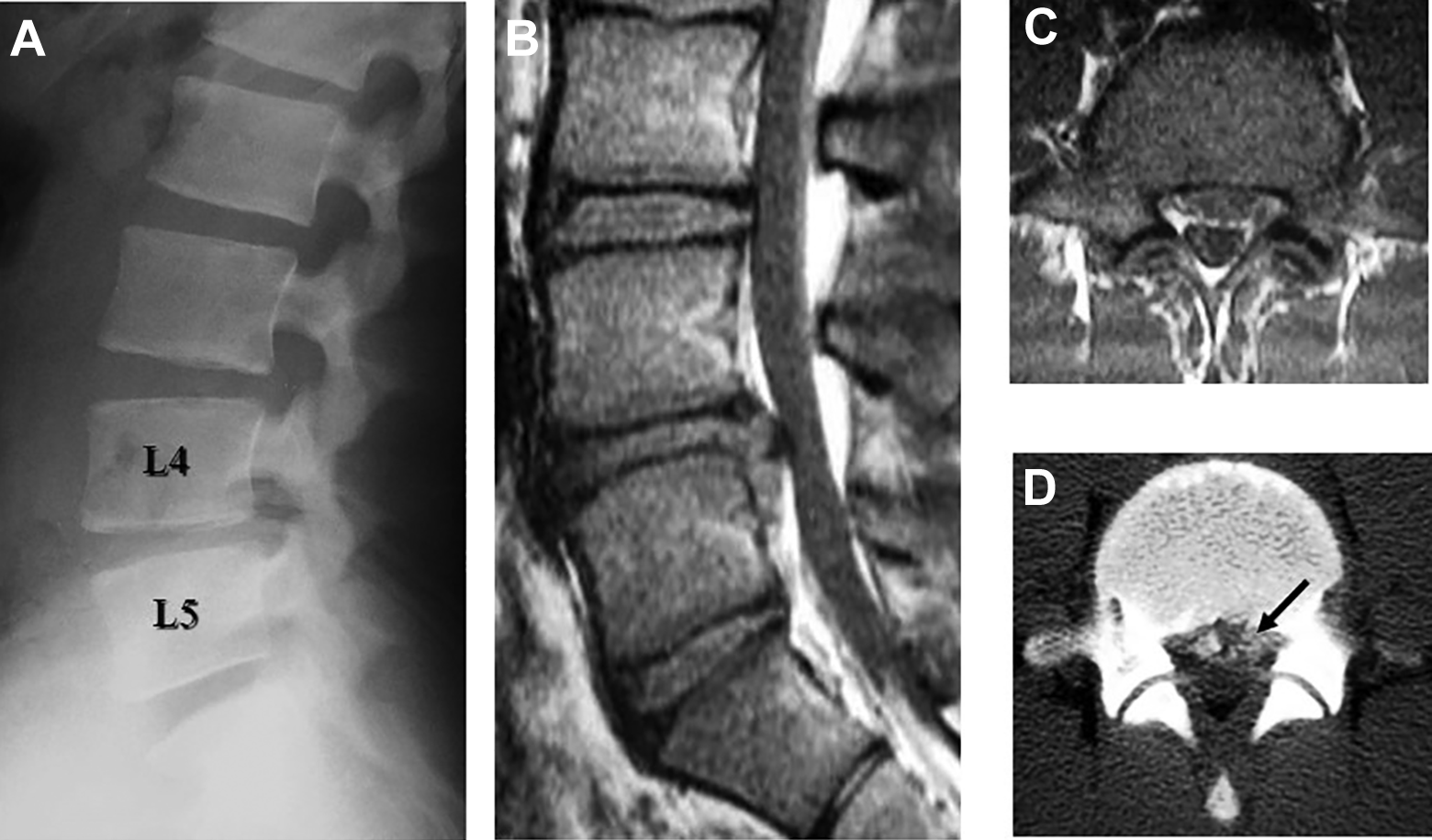
Preoperative imaging studies for case. Plain radiograph and computed tomography (CT) scan show the separated ring apophysis at L4-5. Magnetic resonance imaging (MRI) reveals that the left L5 nerve root and dural sac are compressed. (a) Lateral view of plain radiograph. (b) Sagittal MRI. (c) Axial MRI at L4-5. (d) CT image at L4-5.
He underwent the decompression surgery as mentioned in the Patients and Methods section. The intraoperative findings are shown in Figure 5. The blood loss was 100 mL. The operation time was 84 minutes. Computed tomography and magnetic resonance imaging taken after the surgery showed (1) complete resection of the separated ring apophysis (Figure 6), (2) decompression of the nerve root and dural sac (Figure 7), and (3) preservation of the facet joints (Figure 6). His leg pain disappeared immediately after the surgery. His JOA score was improved to full score within 3 weeks. He returned to judo 3 months after the surgery (Figure 8).
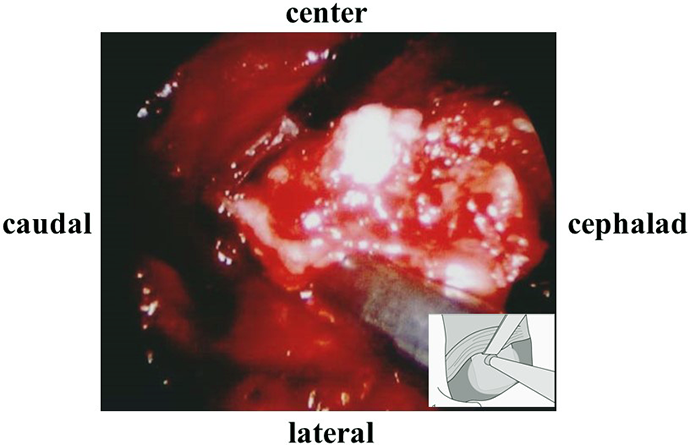
Intraoperative photograph. The nerve root and dural sac are gently retracted toward the center. The separated ring apophysis is resected through the lateral side of the nerve root.
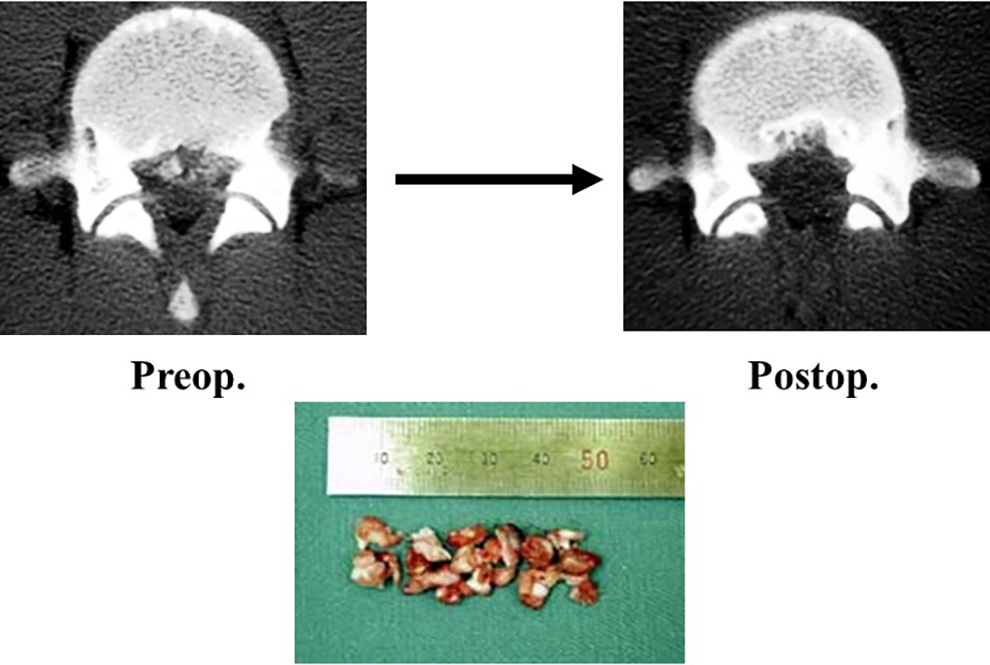
Postoperative computed tomography image and the resected fragments of separated ring apophysis.
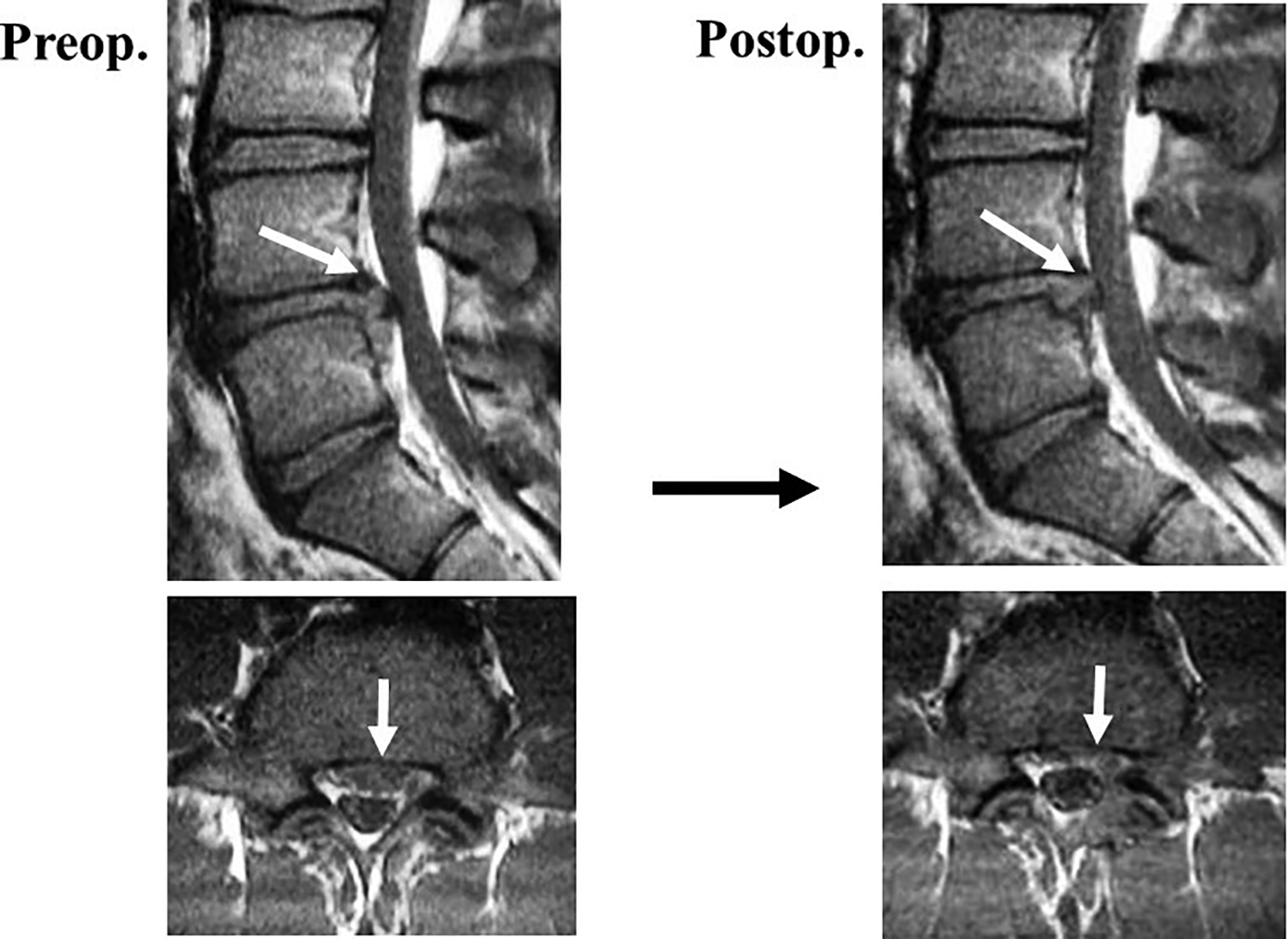
Postoperative magnetic resonance images. The nerve root and dural sac are decompressed.
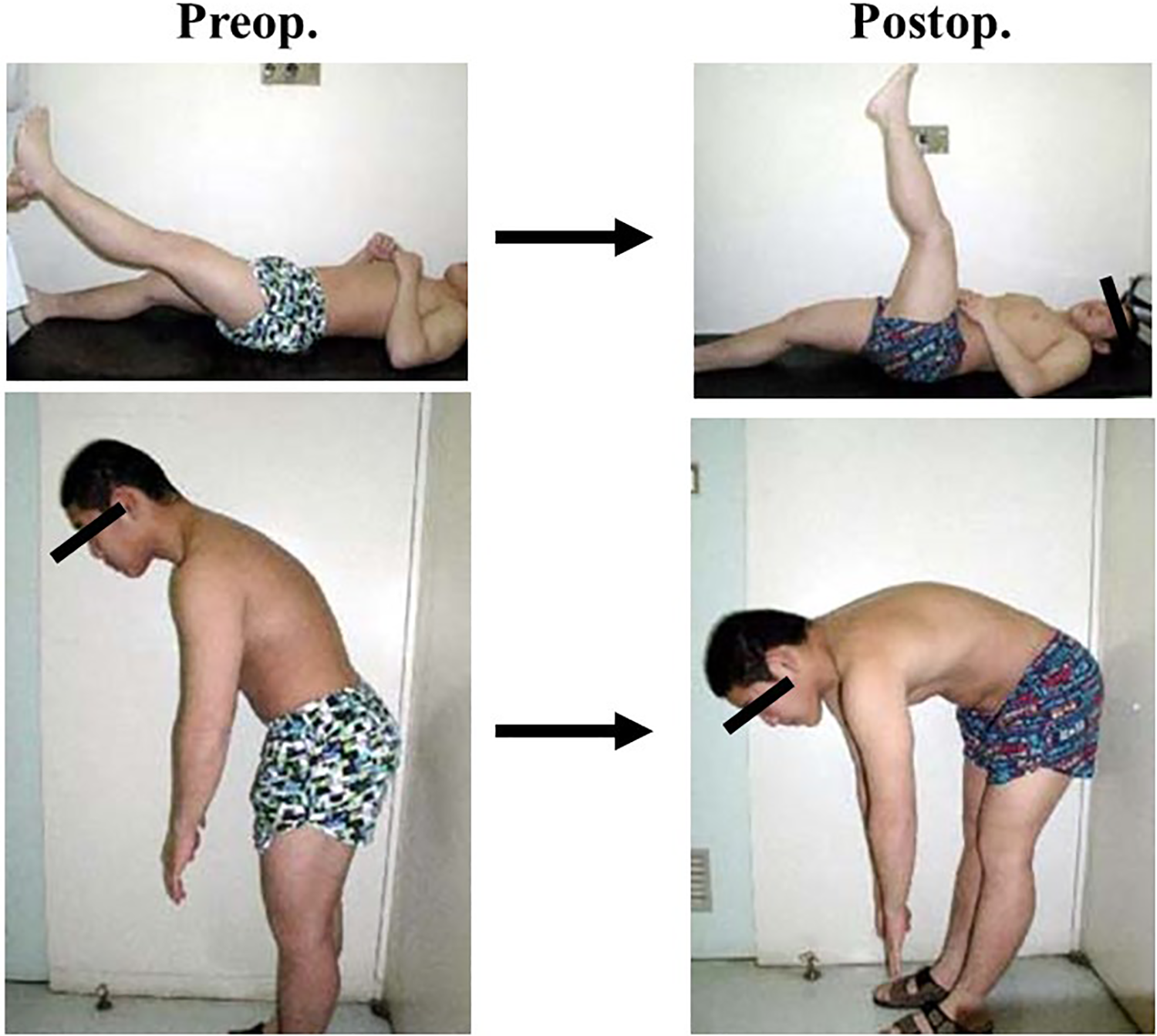
Pre- and postoperative physical examinations. Tension sign became negative and stiffness of body trunk improved postoperatively.
Discussion
All patients in our study provided satisfactory results and all returned to sports.
Akhaddar et al 4 reported the efficacy of hemi- or full laminectomy in 87 patients with their ages ranging from 18 to 54 years (mean age: 36.2 years). Shirado et al 12 reported the efficacy of laminectomy in 32 patients with their ages ranging from 16 to 39 years (mean age: 25.4 years). Bony fragment was removed simultaneously in both reports. The follow-up period was 5.6 and 4.7 months, respectively. The risk of postoperative spinal instability remains unclear in young active athletes because the long-term result was not shown in those reports. The paravertebral muscles and facet joints are likely to be largely damaged in conventional open surgery, especially in separation of lumbar posterior ring apophysis, because wide decompression is often required. Asazuma et al 5 reported the efficacy of posterior umbar interbody fusion in 5 patients with their ages ranging from 14 to 28 years (mean age: 17.4 years). Conventional surgeries can cause barrier in the return to sports in young athletes because of its invasiveness and prolonged limitation of the exercise. Fusion surgery can result in an adjacent segment disease in the future. Takata et al 3 and Savini et al 11 reported the cases in which bony fragment was removed through an anterior approach. However, anterior approach should be avoided because of its difficulty, more invasiveness, and some complications. Furthermore, as we mentioned earlier, the MED system can reduce the risk of the postoperative spinal instability and the future need for fusion surgery as well as can start rehabilitation early after the surgery.
We reported the usefulness and minimal invasiveness of decompression surgery using MED system to the spinal structures for the treatment of lumbar disc herniation and lumbar spinal canal stenosis. 15,16 The technique was applied to a separation of lumbar posterior ring apophysis in young athletes in this study. Operating time was comparable to the conventional open surgery and blood loss was thought to be less than it, with only minor intraoperative complication. The surgical outcome evaluated with JOA scoring system and recovery rate was satisfactory. Furthermore, the surgery using the MED system provided early return to sports. Therefore, this microendoscopic surgery can be a very useful technique for a separation of lumbar posterior ring apophysis in young athletes.
There are some pitfalls in this surgery. First, the procedure is limited within the 16-mm tubular retractor, although surgical field is clearly and widely visualized by using oblique-viewing endoscope. Therefore, this surgery has a somewhat steep learning curve. We recommend gaining some experience of this microendoscopic surgery in the cases of lumbar disc herniation and lumbar spinal canal stenosis before applying it to a separation of lumbar posterior ring apophysis. Second, because resection of the bony fragment is required, intra- and postoperative bleeding can be more of a problem in separation of lumbar posterior ring apophysis as compared with bleeding in lumbar disc herniation or lumbar spinal canal stenosis. The symptoms of epidural hematoma are more likely to occur in microendoscopic surgery than conventional open surgery because of the limited surgical field. Therefore, it is necessary to make sure that hemostasis is firmly achieved (eg, by using bone wax). Third, a separation of lumbar posterior ring apophysis is often huge. In that case, the decompression of the dural sac and contralateral nerve root could require a bilateral approach; that would lead to a longer operating time.
In conclusion, microendoscopic decompression surgery is useful for treating a separation of lumbar posterior ring apophysis especially in young active athletes.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.