
Abstract
Background:
Ramp lesions of the medial meniscus have an impact on joint stability in anterior cruciate ligament (ACL)–deficient knees, but the impact of lesion length and repair is unclear.
Purpose/Hypothesis:
The purpose of this cadaveric study was to evaluate the effect of medial meniscal ramp lesion repair on the biomechanics of ACL-deficient knee joints. It was hypothesized that (1) ramp lesions will increase the anterior tibial translation (ATT), internal rotation (IR), and external rotation (ER) in ACL-deficient knee joints; (2) increasing the length of the ramp lesion will further increase the ATT, IR, and ER; and (3) repairing the ramp lesion will reduce the ATT, IR, and ER after ACL reconstruction.
Study Design:
Controlled laboratory study.
Methods:
Included were 9 fresh-frozen cadaveric specimens (4 left knees, 5 right knees; 6 males and 3 females; mean age, 60 years [range, 40-73 years]). The specimens were tested on a biomechanical rig. Two external loading conditions were applied: a 134-N anterior tibial load and 5-N·m internal/external tibial torque with the knee at full extension and at 15°, 30°, 60°, and 90° of flexion. ATT was tracked via a high-speed video camera. The following knee states were tested: intact; ACL-deficient; ACL-deficient combined with a 5-, 10-, 15-, or 20 mm–long ramp lesion of the medial meniscus; ACL reconstruction; and ACL reconstruction combined with ramp lesion repair. The ATT, IR, and ER at all knee angles were analyzed by 1-way analysis of variance.
Results:
The ATT, IR, and ER were significantly increased after cutting of the ACL (P < .05). The ATT, IR, and ER continued to increase when ACL deficiency was combined with ramp lesions of 5 to 20 mm in length (P < .05). The ATT, IR, and ER significantly decreased after ACL reconstruction and ACL reconstruction combined with ramp lesion repair (P < .05).
Conclusion:
The laxity of knees with ACL deficiency combined with a ramp lesion of the medial meniscus increased more obviously as the ramp lesion increased in length. In a cadaveric model, ACL reconstruction combined with ramp repair improved knee joint stability.
Concomitant meniscal lesions are commonly seen in patients with anterior cruciate ligament (ACL) rupture, especially in the posterior horn of the meniscus and in the posteromedial meniscocapsular attachments. 9 In 1988, Strobel 13 described a particular type of meniscal lesion associated with ACL rupture and termed it a ramp lesion of the medial meniscus. Ramp lesions have historically been underrecognized because they are commonly located within a posteromedial blind spot when using standard anterolateral and anteromedial arthroscopic portals. 14 In recent years, however, medial meniscal ramp lesions have received extensive attention. Recent studies have shown a high prevalence of ramp lesions (16%-17%) in ACL-deficient knees, 7,11 which was associated with a mild anteromedial rotatory subluxation. 3 Ramp lesions are caused by anterior translation of the tibia in ACL-deficient knees, leading to posterior meniscocapsular traction. 1,12 If the tibia is subjected to a greater anterior load, a tear may occur in the posteromedial meniscocapsular junction. 6
Studies have confirmed that ramp injury has an impact on stability of the knee joint, but no biomechanical research on the impact of ramp injury length on knee joint stability, or whether repair of ramp injury can improve stability of the knee joint, has been reported.
In this study, we evaluated the effect of medial meniscal ramp lesion length and repair on the biomechanics of ACL-deficient knees in fresh cadavers. We hypothesized that in a cadaveric model (1) medial meniscal ramp lesions can increase the anterior tibial translation (ATT), internal rotation (IR), and external rotation (ER) in ACL-deficient knee joints; (2) increasing the length of the medial meniscal ramp lesion will continue to increase the ATT, IR, and ER; and (3) repairing the ramp lesion will reduce the ATT, IR, and ER after ACL reconstruction.
Methods
Specimen Selection
Our research was reviewed by 7 members of the review committee of our institution and subsequently approved by the committee. Eleven fresh-frozen human cadaveric knee joints (Weijiao Biotechnology) were evaluated for inclusion in this study. Arthroscopic inspection showed that 2 knees had gouty tophi, and these knees were excluded. Thus, 9 human cadaveric specimens were included in this study; arthroscopic inspection showed that the meniscus was intact without degeneration and ACL was intact. The knees were obtained from 6 male and 3 female cadavers with an average age of 60 years (range, 40-73 years), and they comprised 4 left knees and 5 right knees. The specimens were stored in a freezer at –20°C and thawed to room temperature for 24 hours before testing. The distal tibia and proximal femur were cut 30 cm from the knee joint line. They were then cleaned of soft tissues to enable placement of the femur and tibia into the biomechanical instrument.
Specimen Fixation
The proximal femur was placed on a cylinder above the biomechanical rig and fixed with a 6-mm hexagon socket wrench (Figure 1A). The rear of the cylinder was fixed on the tailstock. The flexion angle of the knee joint was adjusted as necessary (0°-90°). The tibia was placed on the lower sleeve and fixed with a 6-mm hexagon socket wrench. The lower part of the cylinder was connected with a 40 cm–diameter disk through a 50 cm–long rod, which was fixed at the bottom of the frame. Two wires were fixed through the chuck of the disk, the rear of the wire was fixed with a 50 mm–diameter load-bearing disk, the wire was placed at both ends through pulleys, and a load was placed on the load-bearing disk to apply stress to the IR and ER. The lower cylinder was composed of sleeve rings and wires, and the wire was connected with the pull sensor. The front screw handle applied anterior force, and the force value was obtained through the pull sensor (Figure 1A).
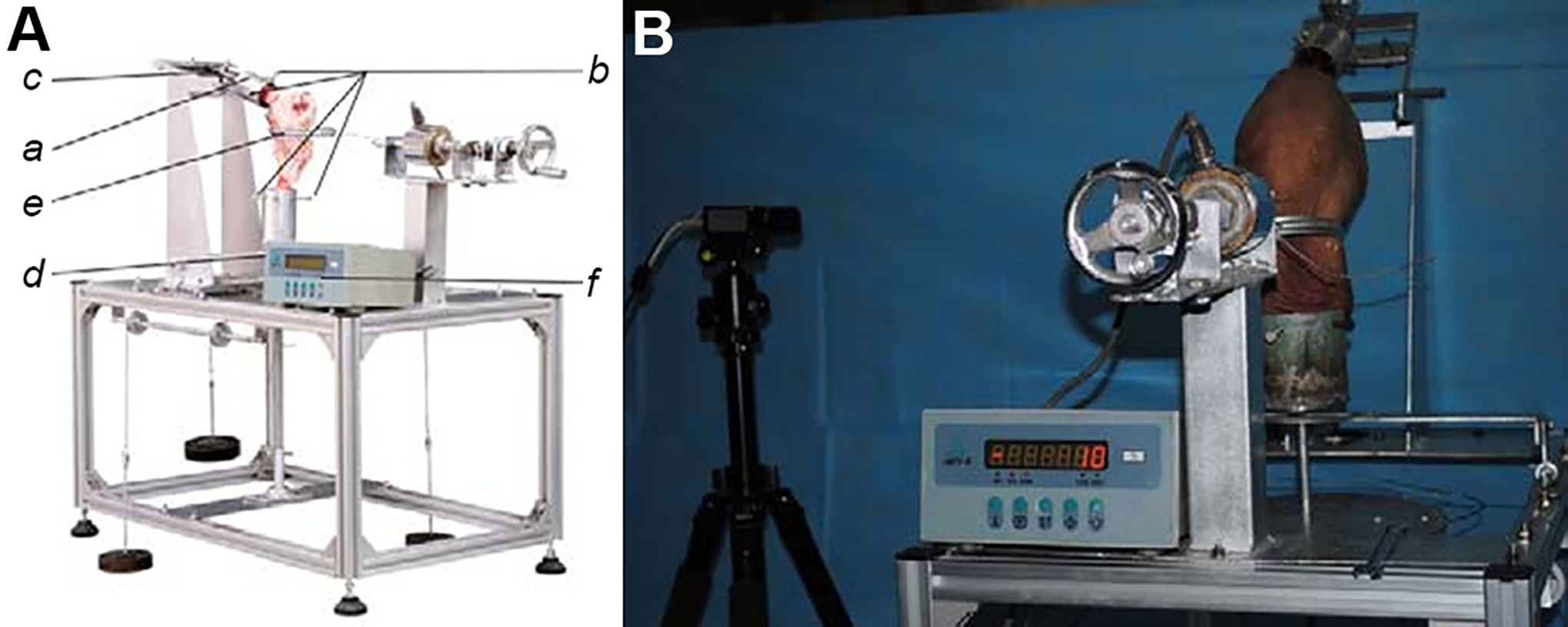
(A) Fixation of cadaveric specimens with biomechanical rig: cylinder to connect the femoral end/tibial end (a); hexagon to fix the femoral end/tibial end (b); tailstock to fix the sleeve of the femoral end (c); disc to apply stress to the internal rotation and external rotation (d); sleeve rings to connect with the front screw handle applied anterior force (e); and pull sensor that displays the anterior force reading (f). (B) Use of high-speed camera to track changes of the knee.
Experimental Process
The knee joints of 9 fresh cadavers were successively subjected to model establishment and mechanical testing, with the following treatment sequence: (1) intact control (no surgical treatment), (2) ACL cutting and ramp injury, (3) ACL reconstruction and ramp injury, and (4) ACL reconstruction and ramp injury repair.
For the ACL cutting and ramp injury model, a No. 10 blade was inserted through the anterolateral approach to cut off the ACL (Figure 2). After establishing the posteromedial and posterolateral approach, a No. 10 blade was inserted into the posteromedial approach, and the ramp area of the medial meniscus was cut by 5, 10, 15, and 20 mm (Figure 3).

(A) Intact anterior cruciate ligament (ACL). (B) The ACL was cut by inserting a No. 10 blade through the anteromedial approach.
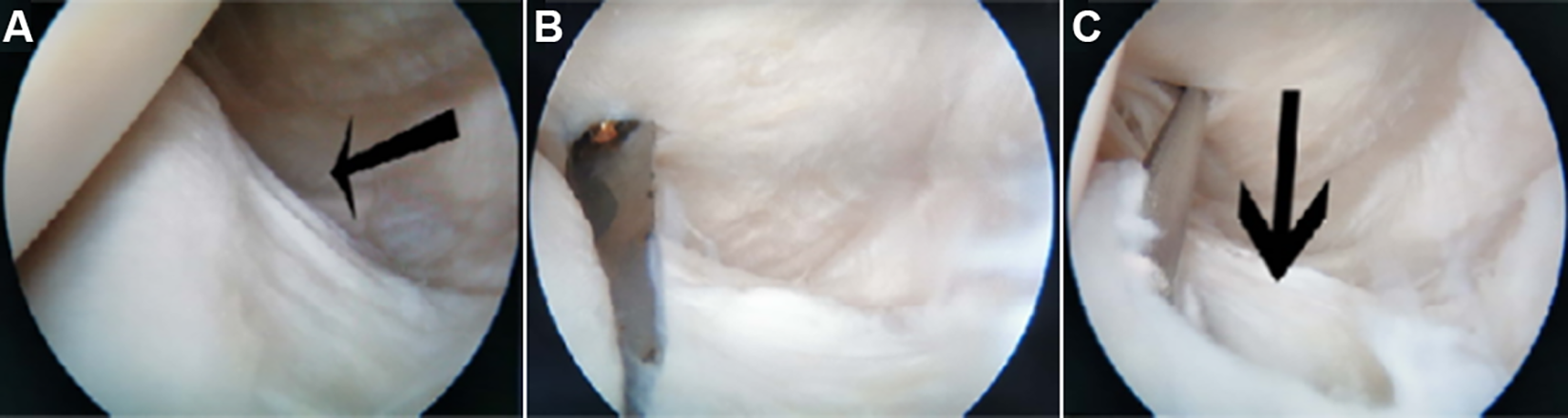
(A) Ramp area of the medial meniscus of an intact knee (black arrow). (B) The ramp area of the medial meniscus was cut. (C) Ramp lesion of the medial meniscus after modeling (black arrow).
For the ACL reconstruction and ramp injury model, the semitendinosus and gracilis tendons of the specimens were woven into grafts with a diameter of 8 mm and a length of 10 cm. ACL reconstruction was performed through the medial approach, and an 8-mm femoral canal and a tibial bone canal were established. The femoral end was fixed by Endobutton suspension (Smith & Nephew), and the tibial end was fixed by interference screw (Smith & Nephew).
For the ACL reconstruction and ramp injury repair model, the posterolateral approach was used to insert a meniscal suture hook. The knee joint was flexed at 90°, and the ramp lesion was sutured by the all-inside technique using a suture hook (Smith & Nephew) with No. 1 polydioxanone suture (Johnson & Johnson Medical GmbH, Germany) (Figure 4). The ramp lesion was measured with a special ruler under arthroscopy, and the biomechanical tests were repeated.

Suture ramp lesion via the posteromedial approach.
For each of the 4 experiment models, 2 external loading conditions were applied: a 134-N anterior tibial load and a rotatory load of 5 N·m internal/external tibial torque at full extension(FE) and 15°, 30°, 60°, and 90° of flexion. The reason for using 134 N and 5 N·m as stress loads was that Stephen et al 12 found through their experimental research that these 2 loads accorded with the mechanical environment of the knee joint under the physiological state. The ATT was tracked by a high-speed video camera (Figure 1B), and the rotation angle was read by the cylinder dial.
Statistical Analysis
Data are expressed as mean ± SD. The ATT, IR, and ER were analyzed by 1-way analysis of variance. To estimate the sample size necessary for the study, we ran an a priori power analysis using G*power Version 3.1.9.2. Assuming a statistical power of β = 0.80 and α = .05, we obtained a sample size of 8. Statistical evaluation of the data was performed using the Student t test, and statistical significance was set at P < .05. SPSS (Version 20.0; IBM Corp) was used for the statistical analysis.
Results
Internal Rotation
Compared with the intact knee, the IR increased significantly at all flexion angles in the ACL-cut state (P < .05). Compared with the ACL-deficient knee, the IR continued to increase significantly at all flexion angles when the ACL was cut with a 5-mm ramp lesion of the medial meniscus (P < .05). When the length of the ramp lesion was extended to 10 mm, the IR continued to increase again at FE and 30° of flexion compared with the 5-mm ramp lesion of the medial meniscus (P < .05). The changes of IR at 60° and 90° of flexion were not statistically significant. When the length of the ramp lesion was extended to 15 mm, the IR continued to increase significantly at all flexion angles (P < .05). When the length of the ramp lesion was extended to 20 mm, the IR continued to increase again at FE and 30°, 60°, and 90° of flexion compared with the 10-mm ramp lesion of the medial meniscus (P < .05). When the ACL was reconstructed, the IR at different flexion angles decreased significantly (P < .05) except for 90° of flexion. When ACL reconstruction was performed and the ramp lesion was repaired, the IR decreased significantly only at 60° (P < .05) (Table 1).
Comparison of Tibial Internal Rotation Angle at Each Flexion Angle a

a Data are reported in degrees as mean ± SD. ACL, anterior cruciate ligament; ACLR, anterior cruciate ligament reconstruction.
External Rotation
Compared with the intact knee, the ER increased significantly at all flexion angles when the ACL was cut (P < .05). When the ramp lesion was 5 mm long, the ER increased significantly compared with the ACL-deficient knee at FE and 30° and 90° of flexion (P < .05). The ER of the 10 mm–long ramp lesion continued to increase significantly compared with the 5 mm–long ramp lesion except at FE (P < .05). When the ramp lesion was 15 mm long, the ER increased significantly compared with the 10-mm ramp lesion at FE and 30°, 60°, and 90° of flexion (P < .05). The ER of the meniscus with a 20 mm–long ramp lesion continued to increase significantly compared with the 10 mm–long ramp lesion except at FE (P < .05). The ER decreased significantly at all flexion angles when the ACL was reconstructed (P < .05). When ACL reconstruction was performed and the ramp lesion was repaired, the ER decreased significantly at all flexion angles (P < .05) (Table 2).
Comparison of Tibial External Rotation Angle at Each Flexion Angle a
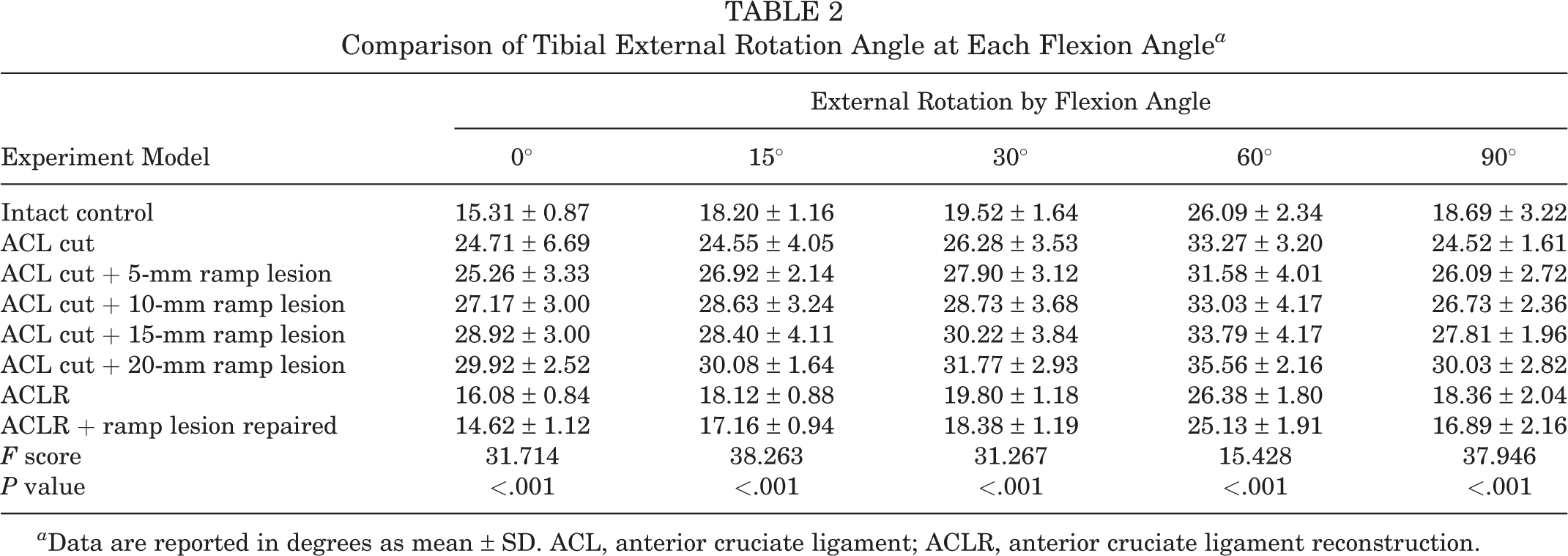
a Data are reported in degrees as mean ± SD. ACL, anterior cruciate ligament; ACLR, anterior cruciate ligament reconstruction.
Anterior Tibial Translation
Compared with the intact knee, the ATT at all flexion angles increased significantly when the ACL was cut (P < .05). After creation of the 5-mm ramp lesion, the ATT at all flexion angles continued to increase significantly compared with the ACL-deficient knee (P < .05). When the length of the ramp lesion was extended to 10 mm, the ATT at all flexion angles continued to increase significantly compared with the ACL-deficient knee with a 5-mm ramp lesion (P < .05). When the length of the ramp lesion was extended to 15 mm, the ATT at all flexion angles increased significantly compared with the ACL-deficient knee with a 10-mm ramp lesion (P < .05). When the length of the ramp lesion was extended to 20 mm, the ATT at all flexion angles increased significantly compared with the ACL-deficient knee with a 15-mm ramp lesion (P < .05). When the ACL was reconstructed, the ATT decreased significantly at all flexion angles (P < .05). When ACL reconstruction was performed and the ramp lesion was repaired, the ATT continued to decrease significantly at all flexion angles (P < .05) (Table 3).
Comparison of Anterior Tibial Translation Distance at Each Flexion Angle a

a Data are reported in degrees as mean ± SD. ACL, anterior cruciate ligament; ACLR, anterior cruciate ligament reconstruction.
Discussion
Through this cadaveric biomechanical study, we found that both ACL deficiency and ACL deficiency combined with a ramp lesion affected knee ATT, IR, and ER. ACL reconstruction decreased the ATT, IR, and ER, but not to the levels seen in the intact state. After repairing the ramp lesion, the instability of IR and ER was alleviated. We also found that the length of the ramp lesion had different effects on stability of the knee. In the evaluation of knee flexion angles and knee lesion status, we found that the ER decreased at a flexion angle of 60°, and we considered this to be a synergistic effect of the collateral ligament and the ACL. Further biomechanical study is required to elucidate the mechanism underlying this phenomenon. Although some previous studies have shown a length of either 15 or 25 mm to be the cutoff for stable versus unstable ramp lesions, we believe that this stability refers to the stability of the meniscus, not the stability of the knee joint.
Ramp lesions are common in ACL-deficient knees. Liu et al 7 found that the probability of a ramp lesion was approximately 17% in ACL-deficient knees. In patients with chronic ACL injuries, the probability of a ramp lesion continues to increase. Papastergiou et al 8 found that after 3 months, ACL deficiency increased the risk of a meniscal lesion. They recommended that ACL reconstruction be carried out within 3 months to minimize the risk of developing secondary meniscal tears. Zoller et al 15 confirmed that ACL reconstruction after >6 months of ACL deficiency increased the risk of medial meniscal lesions.
In a biomechanical study of ramp lesions, DePhillipo et al 4 found that cutting the meniscocapsular and meniscotibial attachments of the posterior horn of the medial meniscus significantly increased the ATT in ACL-deficient knees at 30° and 90° of flexion. After ACL reconstruction, the IR and ER increased at all flexion angles after attachment of the posterior horn of the medial meniscus to the articular capsule and cutting of the meniscotibial ligament. Although ACL reconstruction improves knee stability in ACL-deficient knees, it does not restore normal knee kinematics. DePhillipo et al found that when the flexion angle was greater than 30° after repair of the ramp lesion of the medial meniscus, the IR and ER could not be corrected. Their study result contradicts ours. Our study showed that when the ramp lesion was repaired, the IR and ER could be corrected at any flexion angle. In the biomechanical study by Stephen et al, 12 the ATT, IR, and ER were significantly increased in ACL-deficient knees with ramp lesions. After repair of the ramp lesions, the ATT and IR were decreased; however, there was no significant change in the ER. Ahn et al 2 obtained the same results in their study. Our experimental results showed that repair of ramp lesions can restore the ATT, ER, and IR at any flexion angle. In ACL-deficient knees with ramp lesions, the ramp lesions may be repaired to improve stability. However, the failure rate of ramp lesion repair is high, and the requirements for surgeons are also high. 5,10
Limitations
This study has 3 main limitations. First, the cadaver specimen was very old, which may have led to data errors because of the poor state of the soft tissues in the biomechanical tests. Second, the sample size was small (N = 9), making the data prone to errors. Third, the stress state of the specimens was incomplete. For example, there were only 4 knee flexion angles, which does not represent all flexion states of normal human bodies.
Conclusion
ACL deficiency and ramp lesions of the medial meniscus should be treated simultaneously. ACL reconstruction alone cannot completely restore the stability of the knee.
Footnotes
Final revision submitted August 8, 2022; accepted August 30, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: The study received a grant from the Guangxi Natural Science Foundation from the Department of Science and Technology of Guangxi Zhuang Autonomous Region. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from The People’s Hospital of Guangxi Zhuang Autonomous Region.