
Abstract
Background:
Chronic ankle instability (CAI) alters sensorimotor function and joint coordination, but ankle coordination during walking in copers (patients with a history of ankle sprain without any residual symptoms of CAI) remains unknown.
Purpose:
To identify foot and shank coordination patterns that discriminate among individuals with CAI, copers, and healthy controls and to investigate whether copers display a different strategy to overcome altered sensorimotor function after a lateral ankle sprain compared with individuals with CAI and healthy controls.
Study Design:
Controlled laboratory study.
Methods:
A total of 51 participants (17 participants with CAI, 17 copers, 17 healthy controls) walked on an instrumented treadmill at a fixed speed of 1.20 m/s for a 10-second trial, from which 8 consecutive gait cycles were extracted for analysis. Heel strike and toe-off were identified for each stance phase, and each stance phase was normalized to 100 time frames. A curve analysis was performed to detect group mean differences in vector coding coupling angles and coordination variabilities for sagittal plane ankle motion/transverse plane tibial plane motion (SAK/TT) and frontal plane ankle motion/transverse plane tibial motion (FAK/TT) with 90% CIs.
Results:
During the terminal stance, CAI and coper groups demonstrated an inversion–tibial external rotation coupling, while controls displayed a dorsiflexion–tibial internal rotation strategy. During midstance, there were no differences between the coper, CAI, or control groups. At 0% to 20% of stance, the CAI group showed the most variability, while copers showed the least. During midstance, both copers and controls displayed an increase in variability earlier than the CAI group. The CAI group displayed a peak in variability from 39% to 43% of stance, which was greater than copers. During the propulsive phase (from heel-off to toe-off), the CAI group showed greater SAK/TT variability than both copers and controls. Similar to SAK/TT variability, the CAI group showed an earlier peak in FAK/TT variability compared with controls.
Conclusion:
The CAI, coper, and control groups displayed different ankle joint coupling patterns and coordination variability during a walking gait cycle.
Clinical Relevance:
Copers may have the ability to alter their coordination during walking, which may help us understand the underlying mechanism of CAI.
One of the most common sport-related injuries is a lateral ankle sprain. 23 About 33% to 53% of individuals with a history of ankle sprain develop chronic ankle instability (CAI). 39 Individuals with CAI demonstrate mechanical instability, functional instability, and/or recurrent ankle sprains and report a feeling of the ankle “giving way.” 21
CAI has been associated with altered proprioception, excessive joint laxity, limited dorsiflexion range of motion, and neuromuscular function deficits. 8,22,24,33,42,43 Deficits in sensorimotor function resulting from injury could be one of the contributing factors to altered kinematics of the ankle joint during gait in individuals with CAI. 1,29 For example, individuals with CAI demonstrated a more inverted rearfoot at initial contact and at heel strike during walking and jogging. 10 Further, individuals with CAI also kept the outer side of the foot in contact with the ground for a longer period than those without CAI during the stance phase of walking. 30 Drewes et al 9 also reported that individuals with CAI demonstrated less dorsiflexion range of motion than those without CAI during the stance phase of jogging. Delahunt et al 4 have suggested that altered kinematics of the ankle joint may contribute to the risk of repeated episodes of ankle sprains during walking. Therefore, these studies have focused on differences in ankle kinematics between individuals with and without CAI during gait. However, some studies have focused on the coordination of segments or joints at lower extremity in individuals with CAI. 10,19
Coordination based on dynamic system theory has been considered a sensitive measure of joint mechanics, capable of detecting differences between injured and noninjured individuals. 17 Given that sagittal plane talocrural motion and frontal plane subtalar motion are implicated in ankle sprain, understanding the coupling of these motions in CAI, coper, and healthy populations may offer insights into injury risk factors and potential coping strategies that may be targeted in clinical practice. 32
Modified vector coding identifies the coupling relationship between 2 segments. The coupling angle is determined by the vector orientation between two data points on an angle-angle diagram adjacent in time. 31 It has been suggested that alteration of joint coupling may play a role in ankle injuries during gait. 17,37 Thus, previous studies have focused on coordination of the subtalar frontal plane motion with shank transverse plane motion, where a lateral ankle sprain is most likely to occur. 5,37 For example, Herb et al 19 found that individuals with CAI demonstrated a greater ratio of rearfoot frontal plane to shank transverse plane motion during the early and late swing phases of walking. These findings may describe how individuals with CAI have a high risk of exposure to recurrent ankle sprains. Because individuals with CAI demonstrated limited dorsiflexion that does not allow the ankle to be placed in a closed-pack position, altered dorsiflexion could be also associated with CAI. 9,10 However, to the best of our knowledge, no one has investigated the coupling relationship between talocrural joint motion (plantarflexion/dorsiflexion) and transverse plane motion of the ankle during walking in individuals with CAI.
In addition to the average coordination, it has been suggested that measurement of the variability of coordination patterns within an individual may help to better understand sensorimotor system function in gait. 2 Lower variability could represent either poorly controlled motion or constrained motion, which may cause injury or lower quality of human movement. 16 Two studies have reported that individuals with CAI demonstrated lower variability in coordination of the rearfoot frontal plane with shank transverse plane motion, and in coordination of hip and ankle frontal plane motion, than individuals without CAI. 4,19 According to these results, lower variability indicating constrained motion at the ankle joint could be related to recurrent ankle sprains in individuals with CAI and a compensatory adaptation to instability. However, there is no study investigating coordination variability of ankle frontal or transverse plane motion with ankle sagittal plane motion.
Copers are a group who have a history of ankle sprain and do not have any residual symptoms of CAI. 10,19 Therefore, those with CAI might more appropriately be compared with copers than a control group with no history of ankle sprain because this comparison could provide clinically important insights into successful sensorimotor coping mechanisms after an ankle sprain during walking. 10,19,41 Understanding these sensorimotor adaptations by copers may be useful clinically, providing more realistic target movement patterns for athletes and patients after an ankle sprain. It may not be realistic to expect patients to return to the typical motor control strategies of healthy controls with no history of ankle sprain, given the likelihood of lasting changes to ligament function. However, to date, there is no study investigating the coordination relationship between the foot and shank in copers.
The purpose of this study was to identify differences in the joint coupling and coordination variability of sagittal and frontal plane motion of the ankle and transverse plane motion of the shank among individuals with CAI, those with no history of ankle sprain, and copers throughout the gait cycle during walking. It was hypothesized that individuals with CAI and copers would demonstrate different coupling angles and coordination variability compared with individuals with no history of ankle sprain.
Methods
Participants
The study protocol received institutional review board approval, and written informed consent was provided by all participants. The participants were enrolled from January 1, 2015, to December 31, 2021.
Participants were divided into 3 groups (CAI, coper, and stable ankle [control]) according to number of ankle sprains in the past year, ankle function in the past 6 months, and scores on the Cumberland Ankle Instability Tool (CAIT) and Foot and Ankle Ability Measure–Activities of Daily Living (FAAM-ADL). The inclusion and exclusion criteria for the 3 groups are presented in Table 1. 14,27
Inclusion and Exclusion Criteria for the CAI, Coper, and Control Groups a

a CAI, chronic ankle instability; CAIT, Cumberland Ankle Instability Tool; FAAM-ADL, Foot and Ankle Ability Measure–Activities of Daily Living subscale.
Instruments
Kinematics were collected at 120 Hz and filtered with a fourth-order recursive Butterworth filter at 12 Hz using a 5-camera motion analysis system and associated QTM software (Qualisys). The foot and shank kinetic movements were established by an x-y-z Cartesian coordination system. Vertical ground-reaction force data were collected with a threshold of 20 N by a force plate instrumented treadmill (Treadmetrix) to identify initial contact (heel strike) and final contact (toe-off) on the ground during walking. Force data were sampled at 1200 Hz. Triplanar ankle joint angles for dorsiflexion/plantarflexion, eversion (EV)/inversion (IV), and tibial internal rotation (TIR)/tibial external rotation (TER) were calculated by using Visual 3D software (C-Motion).
Procedures
All participants wore neutral running shoes (New Balance model 690) during walking. Retro-reflective markers were placed over the base of the first and fifth metatarsals, the lateral and medial malleoli, and the lateral and medial epicondyles of the femur. 11 Clusters of tracking markers were placed on the heel counter of the shoe and the lateral shank. All participants walked on the treadmill at their preferred gait speed for 3 minutes as a warm-up. They then walked on the treadmill at a fixed speed of 1.20 m/s for a 10-second trial, from which 8 consecutive gait cycles were extracted for analysis. Analysis of 8 trials has been suggested as a minimum stride for variability using vector coding during walking. 15 Heel strike and toe-off were identified for each stance phase. Each stance phase was normalized to 100 time frames, where frame 0 stands for heel strike and frame 100 stands for toe-off.
Vector Coding Analysis
The vector coding analysis for this study is based on the work of Sparrow et al 36 and is intended to identify the relative motion patterns between 2 segments: (1) frontal plane ankle motion for IV and EV/transverse plane tibial motion for TER and TIR (FAK/TT) and (2) sagittal plane ankle motion for dorsiflexion and plantarflexion/transverse plane tibial motion for TER and TIR (SAK/TT). We used Microsoft Excel 2016 (Microsoft Corp) and MATLAB 2019a (MathWorks) to implement the vector coding procedures.
The mean coupling angle that was obtained by the vector coding analysis was partitioned into 8 coordination patterns according to 3 criteria regarding the ankle and tibia. These 8 coordination patterns stem from the partitioning of the polar distribution into 45° sections. For SAK/TT, the value of the mean coupling angle can be interpreted as (1) antiphase or in-phase ankle/tibial dominancy, (2) ankle dorsiflexion or plantarflexion, or (3) tibial internal or external rotation (Figure 1A). Similarly, for the FAK/TT, the value of the mean coupling angle can be interpreted as (1) antiphase or in-phase ankle/tibial dominancy, (2) ankle IV or EV, or (3) tibial internal or external rotation (Figure 1B). The only difference between SAK/TT and FAK/TT is that ankle dorsiflexion or plantarflexion is evaluated for SAK/TT and ankle IV or EV is evaluated for FAK/TT. 26 This is due to the difference between SAK/TT and FAK/TT: SAK/TT evaluates the relative motion patterns between the sagittal plane ankle motion for dorsiflexion and plantarflexion and transverse plane tibial motion for TER and TIR, while FAK/TT evaluates the relative motion patterns between frontal plane ankle motion for IV and EV and transverse plane tibial motion for TER and TIR.
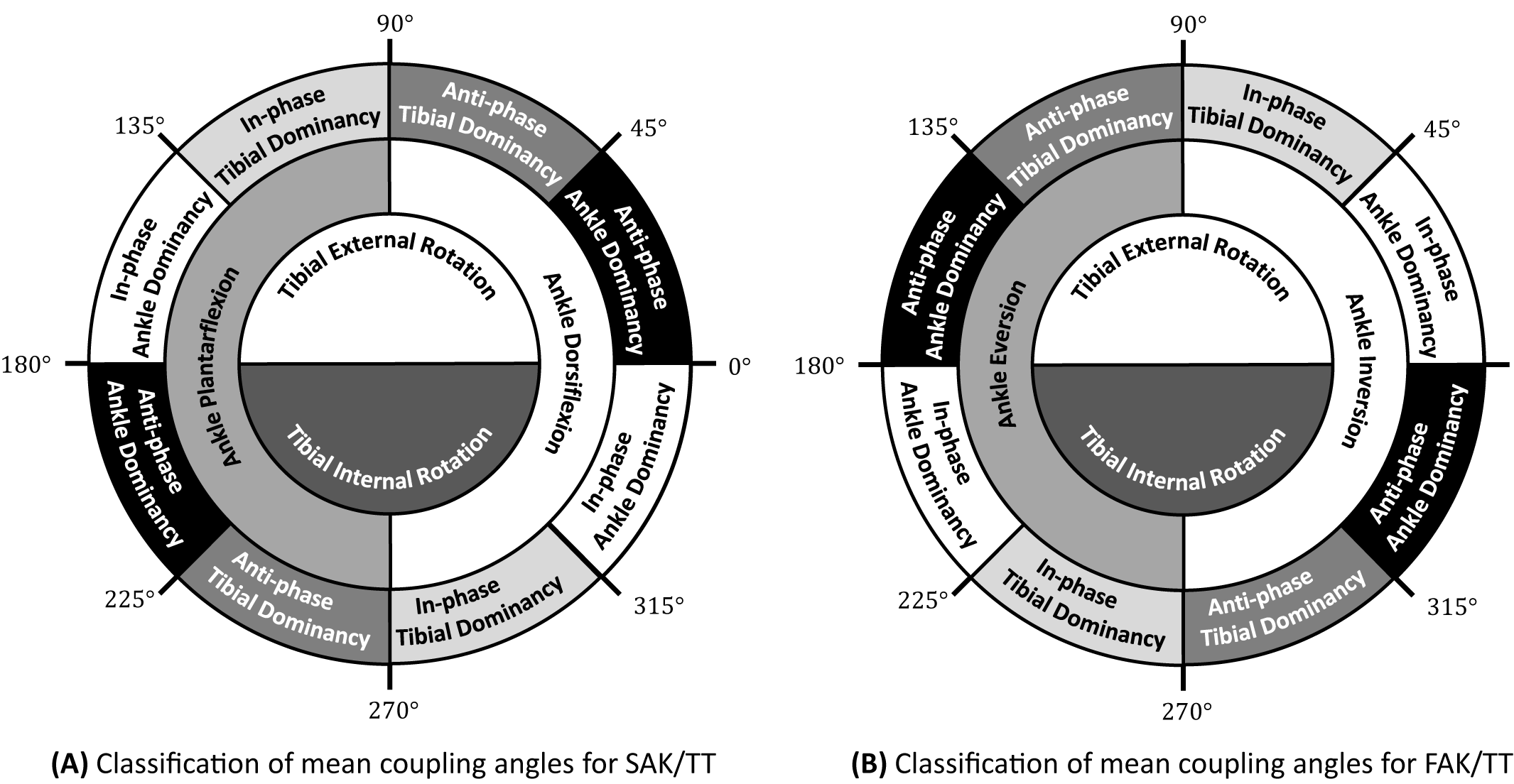
Classification of coordination patterns for ankle-tibial mean coupling angle. FAK/TT, frontal plane ankle motion/transverse plane tibial motion; SAK/TT, sagittal plane ankle motion/transverse plane tibial plane motion.
The coupling angle variability was also obtained from the vector coding analysis. If the variability value was close to 1, this indicated that the coupling angle values were stable across the multiple gait cycles; if it was close to 0, the values of the coupling angle were unstable across the multiple gait cycles. In other words, the lower the variability across the multiple gait cycles, the closer to 1 the value of the coupling angle variability.
Statistical Analysis
The vector coding coupling angles and coordination variabilities of SAK/TT and FAK/TT were recorded as means with 90% CIs and were analyzed during the stance phase of walking for all 3 study groups. A curve analysis (alpha level of P < .05) was performed to detect group mean differences, indicated by more than three consecutive increments in which the 90% CI for each group did not intersect. 19,29 Microsoft Excel 2016 was used for group mean differences and associated standard deviations. 19,29
An a priori power analysis (α = .05; β = 0.08) performed on similar kinematic variables during gait determined that 17 participants per group (range, 7-29 participants) was necessary for adequate power. 3,10,19
Results
A total of 51 participants, 17 participants (9 men, 8 women) per group, were included. There were no significant differences in height, mass, or age among the groups, as summarized in Table 2. 26 The CAIT and FAAM-ADL scores in the CAI group were significantly lower than those in the coper and control groups (P < .05 for both).
Characteristics of the Study Groups a
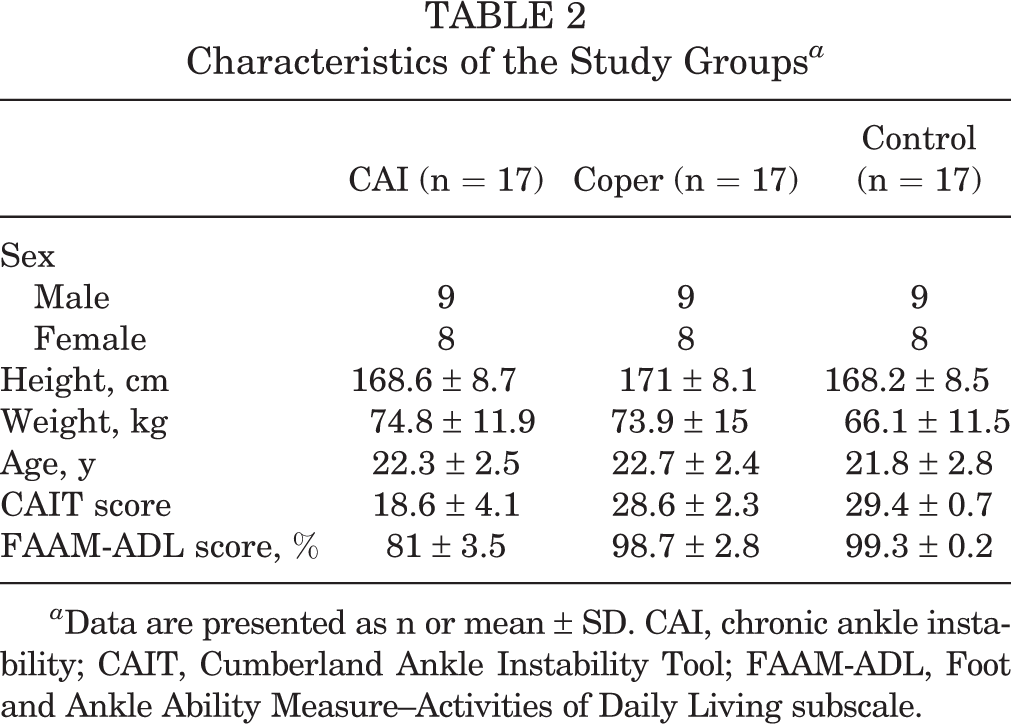
a Data are presented as n or mean ± SD. CAI, chronic ankle instability; CAIT, Cumberland Ankle Instability Tool; FAAM-ADL, Foot and Ankle Ability Measure–Activities of Daily Living subscale.
Variability in SAK/TT Between Groups
Controls demonstrated greater ankle dorsiflexion movement than individuals with CAI while the tibia was externally rotated between 33% and 36% of the stance phase. However, there were no significant differences in the SAK/TT angles between the CAI and coper groups or between the copers and controls (Figure 2, A-C).
The CAI group had significantly higher variability in SAK/TT between 54% and 76% of the stance phase than copers, and between 17% and 21%, 40% and 46%, and 54% and 83% of the stance phase than controls (P < .05 for all). However, the CAI group had lower variability in SAK/TT between 84% and 100% of the stance phase than copers and between 85% and 91% of the stance phase than controls (P < .05 for all). Copers had higher variability in SAK/TT between 43% and 50%, 55% and 58%, 66% and 74%, 79% and 85%, and 90% and 100% of the stance phase than controls (P < .05 for all) (Figure 2, A-C).

Comparison between the study groups of the 90% CIs (reported as mean ± SD) for the coupling angle and variability values for (A-C) SAK/TT (sagittal plane ankle motion/transverse plane tibial plane motion) and (D-F) frontal plane ankle motion/transverse plane tibial motion (FAK/TT) during walking. Boxed areas indicate significant differences between groups. Data in the corners of the box indicate the starting and ending points. CAI, chronic ankle instability.
Variability in FAK/TT Between Groups
Controls demonstrated an ankle IV–TIR strategy, while the CAI and coper groups demonstrated an ankle IV–TER strategy between 80% and 86% of the stance phase. However, there were no significant differences in the FAK/TT angles between the CAI and coper groups (Figure 2, D-F).
The CAI group had higher variability in FAK/TT between 6% and 9%, 39% and 43%, 59% and 67%, and 69% and 79% of the stance phase than copers, and between 13% and 17%, 62% and 67%, and 69% and 74% of the stance phase than controls (P < .05 for all). However, individuals with CAI had lower variability in FAK/TT between 21% and 36% of the stance phase than copers, and between 27% and 39%, 55% and 58%, and 75% and 81% of the stance phase than controls (P < .05 for all). Copers had lower variability in FAK/TT between 6% and 12%, 57% and 61%, and 70% and 81% of the stance phase, and higher variability in FAK/TT between 21% and 36% of the stance phase than controls (P < .05 for all) (Figure 2, D-F).
Discussion
To our knowledge, this is the first study to report on differences in coupling and coordination variability of the ankle in copers as well as individuals with CAI and healthy controls during walking. Differences between the groups were noted in both coupling relationships and variability.
Coupling Angles
During the terminal stance, both the CAI and the coper groups displayed an IV-TER coupling, while control participants displayed a dorsiflexion–TIR strategy. This indicates that control participants reverse to TIR before individuals with a history of ankle sprain. The combination of dorsiflexion and TIR may be an attempt by individuals with previous ankle sprain to gain passive support and proprioceptive feedback from the posterior talofibular ligament, which is the least likely to be involved in ankle sprain. 20,25 Our results are in contrast to previous studies finding no differences in frontal and transverse plane coupling within the ankle joint in individuals with CAI during the stance phase of walking. 10,19 These discrepancies likely arise from differences in methods of calculating coupling. Drewes et al 10 found no differences in ankle coordination using a continuous relative phase to examine this coupling relationship, which takes into account joint velocity, which may mask differences in relative changes in joint position. Herb et al 19 also found no differences in ankle coordination using a vector coding technique to compare individuals with CAI with healthy controls; however, their vector coding angles were collapsed to 90°. Silvernail et al 35 have since shown that collapsing vector coding angles can allow for incorrect interpretation. For example, using a 360° scale, equal degrees of TER and EV would be considered antiphase motion or uncoupled motion, while using a 90° scale, this same coordination pattern would be classified as “equal segmental motion,” which may be incorrectly interpreted as highly coupled motion.
During midstance, all groups displayed a dorsiflexion–TER coupling pattern. However, dorsiflexion was more dominant in the control group than the CAI group. This strategy may allow individuals with healthy ankles to maintain a more stable ankle joint loading. Since the coper group was not different from individuals with CAI or controls, it appears that they use a strategy that falls somewhere in the middle of healthy and high-risk movement patterns.
Variability
Variability differed between groups for a greater proportion of the stance phase, indicating that sensorimotor constraints arising from injury may have a more pronounced effect on motor flexibility as opposed to joint motion. From about 0% to 20% stance, during which the transition from single- to double-limb support takes place, individuals with CAI showed the most variability, while copers showed the least. This was counter to our expectation that copers would demonstrate sensorimotor characteristics somewhere between those of CAI and control participants. This suggests that copers and individuals with CAI use different strategies to accomplish the coordinating transition from single- to double-limb support. Individuals with CAI may employ a more flexible strategy to distribute load. Copers may have found a narrow range of “safe” coordination strategies and stay within this range to avoid potentially injurious ankle motion at impact. In agreement with our results observed in copers, reduction in variability measured using a continuous relative phase has been previously reported in asymptomatic athletes with a history of injury. 17,28,34
In examining variability during midstance, it appears that both copers and controls display an increase in variability earlier than individuals with CAI. This increase in variability may reduce the first peak of the vertical ground-reaction force, as the increase in variability could reduce repetitive damage to the same ankle. 17 CAI may be constrained by sensorimotor deficits after injury, and thus have fewer available coupling strategies as load increases. Individuals with CAI do display a peak in variability from 39% to 43% stance, which is greater than the variability displayed by copers during that period. It could be that as loads fall after the first peak of the vertical ground-reaction force, flexibility is restored in the CAI group.
After midstance, during the propulsive phase (ie, from heel-off to toe-off), individuals with CAI showed greater SAK-TT variability than both copers and controls. Visual inspection of the variability plots suggest that this is due to the rise in variability typically associated with transition points occurring earlier in the CAI group. An important transition during late stance is from single- to double-limb support. Previous research has reported that CAI demonstrates a shorter period of single-limb support, perhaps as a strategy to maintain stability. 12 Thus, it could be that the differing periods of high and low variability between individuals with CAI, copers, and healthy controls are partly related to different timings of transition events during gait.
Similar to SAK-TT variability, CAI showed an earlier peak in FAK-TT variability compared with control participants, which again suggests an earlier occurrence of a transition event. This period of increased variability of FAK-TT coordination was absent in the coper group. Similar to early stance, it is possible that copers have identified a narrow range of coordination patterns that allow them to safely transition from single- to double-limb support. This lack of variability may have consequences in terms of adaptability and cumulative overuse.
There are a limited number of studies investigating the variability of lower extremity motion of copers compared with CAI and control groups. 10,18,19,26 However, the previous studies have demonstrated conflicting results. For example, Herb et al 18 found that copers demonstrated less variability of ankle frontal motion than individuals with CAI during a jumping task, and control participants demonstrated greater knee and hip variability than copers and individuals with CAI during a jump landing task. Thus, similar to our results, it appears that movement variability, as well as differences in variability between the CAI, coper, and control groups, depends on the task. This could be due to the different demands of sensorimotor function in each gait phase. Copers may use a coping strategy to prevent reinjury by using either more or less variability than individuals with CAI and/or healthy controls, depending on the task to be accomplished.
Limitations
Several limitations should be considered when interpreting the results of this study. Since the relationship between variability, function, and injury is still largely theoretical, the exact benefits and consequences of lower or higher variability in clinical populations is unclear. Further, both male and female participants were included in this analysis. Since men and women are known to display different coordination patterns in the foot and ankle, this may have confounded our results. 38 Also, the characterizations of the groups that have influenced our observations can be further analyzed using magnetic resonance imaging evidence and subtalar joint anatomy, which can be used to investigate the injuries to tissues in copers and individuals with CAI anatomically. Last, taking pes cavus versus pes planus, forefoot adduction versus abduction, and other subtalar configurations into account can help us to better analyze their effects on the forces and motions seen at the ankle.
Conclusion
Dorsiflexion was more dominant in the healthy control group than the CAI group, which indicates a more stable ankle joint during loading. Copers used a gait strategy falling in the middle of healthy and CAI movement patterns. Since limited dorsiflexion range of motion may result in recurrent ankle sprains, clinicians should treat these deficits appropriately. These deficits can be recovered by gliding the talus posteriorly on the tibia. 6,13,40
With regard to variability, during midstance to propulsive phases, copers were more likely to employ a narrow range of coordination strategies compared with individuals with CAI. Variability is thought to be beneficial to injury prevention, as it may allow for load to be distributed across tissues. However, variability using unsound coordinating patterns, as seen in the CAI group, is not beneficial. The limited variability of copers may reflect their ability to maintain sound coordinating patterns despite sensorimotor deficits. 7 Copers may display a different coping strategy of ankle joint coupling patterns and coordination variability during walking compared with individuals with CAI or healthy ankles to prevent resprain. In addition, copers may have a natural gait pattern that simply relies less on the injured ankle.
Clinicians should be aware of the intersegmental and multiplanar alterations and consider these changes when they plan and implement rehabilitation programs. Such rehabilitation may lead to better central reorganization of movement patterns and improved function during gait for individuals with a history of ankle sprain. 19
Footnotes
Final revision submitted August 16, 2022; accepted September 8, 2022.
One or more of the authors has declared the following potential conflict of interest or source of funding: This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) (No. 2020R1G1A1008736). This research was also supported by a 2021 Chung-Ang University Research Grant. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Chung-Ang University (reference No. 1041078-202111-HR-335-01).