
Abstract
Purpose:
We aimed to examine the functional outcome in different walking conditions in elderly adults who underwent surgical repair after a non-contact hamstring injury. Our objective was to compare lower limb kinematics and kinetics over the entire gait cycle between the injured and contralateral leg in overground and level and uphill treadmill walking.
Methods:
12 patients (mean ± SD, age: 65 ± 9 years; body mass index: 30 ± 6 kg/m2) walked at self-selected speed in overground (0% slope) and treadmill conditions (0% and 10% slope). We measured spatiotemporal parameters, joint angles (normalised to gait cycle) and joint moments (normalised to stance phase) of the hip, knee and ankle. Data between sides were compared using paired sample t-tests (p < 0.05) and continuous 95% confidence intervals of the paired difference between trajectories.
Results:
Patients walked at an average speed of 1.31 ± 0.26 m/second overground and 0.92 ± 0.31 m/second on the treadmill. Spatiotemporal parameters were comparable between the injured and contralateral leg (p > 0.05). Joint kinematic and joint kinetic trajectories were comparable between sides for all walking conditions.
Conclusions:
Refixation of the proximal hamstring tendons resulted in comparable ambulatory mechanics at least 1 year after surgery in the injured leg and the contralateral leg, which were all within the range of normative values reported in the literature. These results complement our previous findings on hamstring repair in terms of clinical outcomes and muscle strength and support that surgical repair achieves good functional outcomes in terms of ambulation in an elderly population.
Trial registration:
clinicaltrials.gov (NCT04867746).
Introduction
Although hamstring injuries are most common during athletic activities – with an incidence of 1.2–4 injuries per 1000 hours of athletic exposure1,2 – their prevalence is also increasing in older adults during daily activities because of the increasingly active elderly population. 3 Moreover, older adults are at higher risk of injury due to tendon degeneration or chronic tendinopathy, in which tendons often become the weakest part of the muscle-tendon-bone unit, 4 making the tendon vulnerable to injury. 3
Proximal hamstring injuries are often caused by rapid hip flexion with simultaneous knee extension. 2 The degree of injury can vary, ranging from a muscle strain to an avulsion of 1, 2, or all 3 tendinous insertions on the ischial tuberosity. 5 Anatomically, the proximal hamstring originates on the lateral aspect of the ischial tuberosity and consists of the semimembranosus (SM), semitendinosus (ST), and the long head of the biceps femoris (BF) muscles. 6 The SM has a more proximal and lateral origin than the ST and long head of the BF, and together they constitute the conjoint tendon. 6 Current evidence suggests that outcomes are better after surgical treatment than conservative treatment when all 3 tendons (i.e., SM, ST and BF) are a completely avulsed or at least 2 tendons are retracted (i.e., shortened) by >2 cm.7 –9 In surgical refixation, the injured tendon is usually reinserted at the anatomic origin of the ischial tuberosity,10,11 or more proximally and laterally to the original origin in a modified technique to avoid postoperative discomfort during sitting.12,13 While clinical and patient-reported outcomes of surgical hamstring repair have been described in the literature for the conventional and also for the modified technique,7,10,12,14 there is limited evidence of the functional outcomes of surgical repair for human locomotion.
The biomechanical function of the hamstring muscle complex is to extend the hip and flex the knee. Walking is a basic and the most common activity in daily life. The hamstring muscles are active throughout the gait cycle, but especially during terminal swing to slow knee extension and initiate hip extension. 14 They are also active during early stance to assist in hip extension. Because the hamstring muscles span both the hip and knee, they are at a greater risk of injury due to the potential for rapid muscle lengthening during the combined hip flexion and knee extension that occurs during the swing phase in walking.7,14
Although it is not necessary for a healthy person to consciously focus on alternating stepping during habitual walking, it is a complex and demanding movement that is exacerbated on a treadmill or when walking uphill. Walking uphill places greater demands on the leg muscles, 15 which may exacerbate injury- or age-related changes in lower leg kinetics and gait patterns.16,17 Consequently, the improvement of walking ability with therapeutic interventions is 1 of the most important clinical criteria and serves as an indicator of the functional outcome. 18
For patients after hamstring injury and/or surgical repair of the hamstring complex, there is no evidence on gait patterns. This is especially true for elderly patients, who often require a longer rehabilitation period and for whom surgical treatments often fail to restore full tendon function due to reduced regenerative capacity. 19 Therefore, we aimed to investigate the functional outcomes of activities of daily living under different walking conditions in older adults treated surgically after non-contact proximal hamstring injury. Specifically, our objective was to compare gait parameters and lower limb kinematics and kinetics over the entire gait cycle during walking between the injured and contralateral leg. We hypothesised that a surgical technique involving functional anatomic reconstruction of the tendon would restore walking biomechanics, both on a level surface and during more challenging treadmill or uphill walking.
Material and methods
Study design and participants
In this retrospective study, 17 patients were identified who were treated surgically for proximal hamstring rupture by a single senior surgeon at a single hospital between 2014 and 2019, all of whom received the extra-anatomic anchor positioning procedure. 12 All patients were retrospectively contacted at least 1 year after surgery at the time of the study (November 2020–June 2021) and asked to participate in the follow-up examination. Inclusion criteria were age > 18 years and surgical repair with modified anchor placement for proximal hamstring ruptures between 2014 and 2019. Exclusion criteria were revision surgery within 6 months before the study on the ipsilateral knee or hip, injury or surgical procedures of the contralateral knee or hip within the last year, and inability to provide informed consent. The study was approved by the regional ethics committee (EKNZ-2020-02276) and registered at clinicaltrials.gov (NCT04867746). All participants signed an informed consent prior to participation.
Surgical technique
The surgery was performed according to the procedure described by Chocholáč et al. 12 First, the origin of the proximal hamstring tendons at the ischial tuberosity and the modified reinsertion point on the lateral and proximal side were localised. At the latter sites, 3 Arthrex BioComposite Corkscrews (FT 5.5 mm × 14.7 mm anchors, Arthrex, FA, USA) were introduced into the bone: 2 were placed proximally and 1 distally. The hamstring tendons were fixed at these sites with non-resorbable FibreWire anchor threads (FibreWire, Arthrex, FA, USA). A detailed description of the surgical method can be found in Chocholáč et al. 12
Experimental protocol
All functional tests were conducted at the Functional Biomechanics Laboratory at the Department of Orthopaedics and Traumatology at the University Hospital Basel (Switzerland). Patients were equipped with retroreflective markers as described in detail below. Kinematic and kinetic data were collected for two types of walking, namely overground and treadmill walking. For overground walking, patients completed walking trials at their self-selected walking speed on a 10-metre walkway with 2 embedded force plates (Kistler force plate 9260AA6, Kistler AG, Winterthur, Switzerland: sampling rate 2400 Hz) until data for 6 valid trials per side were recorded. Participants then walked on a treadmill (h/p/ cosmos, mercury, Traunstein, Germany). After a 5-minute familiarisation period, data were collected for the last 30 seconds of a 2-minute walk at 0% slope and at 10% slope, respectively. Participants chose a self-selected speed for level walking, which was reduced to 85% of self-selected speed for uphill walking.
Spatiotemporal parameters
Walking speed and cadence for all walking conditions, as well as step time, step length, stance phase, and single support phase were determined using kinematic measures as described below. 18
Kinematics and kinetics
Kinematic data were collected using a 3-dimensional motion analysis system with 10-cameras (Vicon, Oxford, UK; sampling rate 240 Hz). Joint angles and external joint moments for the hip, knee (sagittal and frontal), and ankle (sagittal) were determined using reflective markers placed on predefined anatomic landmarks on the pelvis and lower legs using the CGM 2.3 model.20,21 Joint moments were normalised to body mass and only measured for the overground condition.
Data processing
Data were analysed offline using a custom-written Matlab program (Mathworks, Natick, MA, USA). Heel-strike and toe-off for overground walking were identified using the force plates embedded in the walkway. For treadmill walking, heel-strike and toe-off were identified using the velocity zero crossing (in walking direction) of the heel and toe markers, respectively, according to a previously described method. 22 Kinematic trajectories were time normalised to gait cycle (101 data points per gait cycle) and kinetic trajectories were time normalised to stance phase (51 data points per stance phase). The average trajectories of the 6 trials were computed for each parameter, side and patient. Comparisons were made between the injured and contralateral side.
Statistical analysis
Paired t-tests were used to test for differences in spatiotemporal parameters between the injured and the contralateral side (p < 0.05). Comparability of gait trajectories between the injured and contralateral legs was assessed using the confidence interval approach and minimum clinically relevant differences. 23 The 95% confidence interval (CI) around the mean paired difference between the injured and contralateral limb was calculated for each time point of the kinematic and kinetic trajectories and visually presented. 24 Because the difference between sides could be in either a positive or negative direction, both positive and negative values were used to define clinical relevance, forming a relevance interval defined as ±3° for kinematic trajectories and ±0.1 Nm/kg for kinetic trajectories.25,26 Comparable results in trajectories between sides were concluded if the confidence interval contained zero and if the mean differences was contained within the relevance interval. All analyses were conducted in Matlab.
Results
Patient characteristics
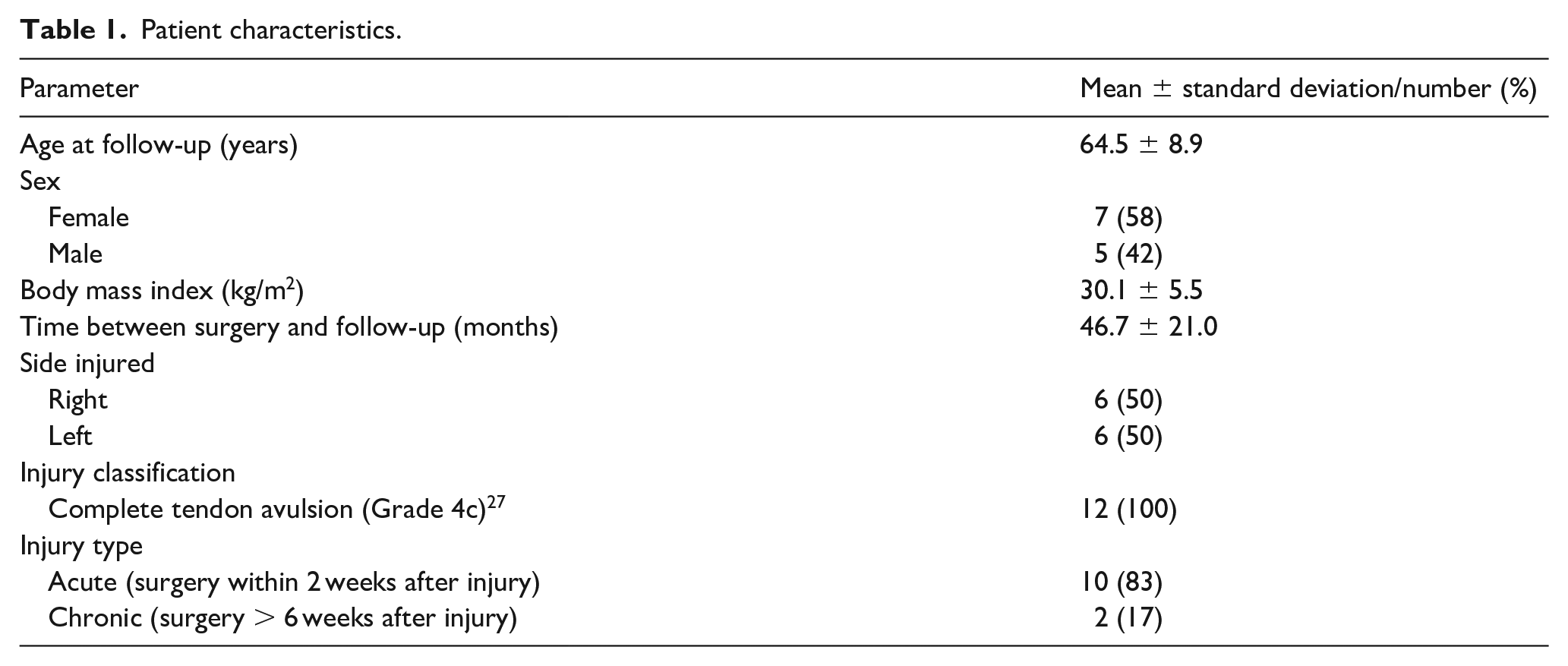
Overall, 12 patients completed gait analysis at follow-up. All patient characteristics are listed in Table 1. 1 subject was not able to perform gait analysis due to pain not related to hamstring injury (Figure 1).
Patient characteristics.
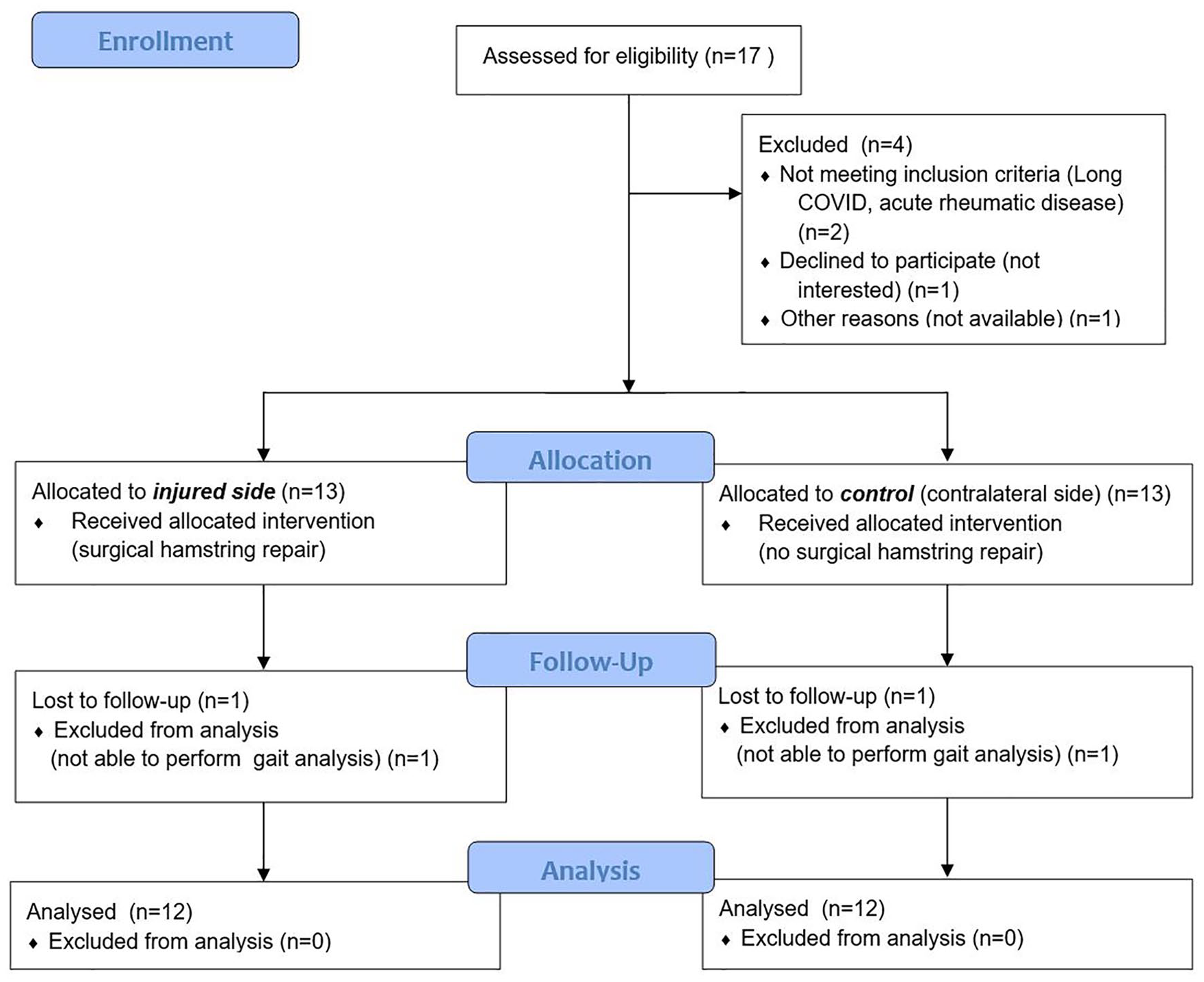
CONSORT flow chart.
Spatiotemporal parameters
Self-selected walking speed and cadence were slower for treadmill than for overground walking conditions (Table 2). Spatiotemporal parameters did not differ between sides (p > 0.05) for all walking conditions (Table 3).
Gait speed and cadence for the different walking conditions.

Spatiotemporal parameters for the injured and contralateral side.

paired t-test.
Joint kinematics
Overall, the joint kinematics for the injured leg were comparable to those of the contralateral leg for all walking conditions (Figure 2). The mean paired differences in the trajectories of hip flexion and adduction, knee flexion and adduction, and ankle dorsiflexion angle between the injured and contralateral leg were largely within the relevance interval for all walking conditions. The trajectories for knee adduction showed a systematic shift towards more abduction/less adduction (negative difference) throughout the gait cycle for all walking conditions, but the 95% CI did not contain zero, except for a very brief moment around toe-off for the overground walking condition, but the mean difference remained within the relevance interval.
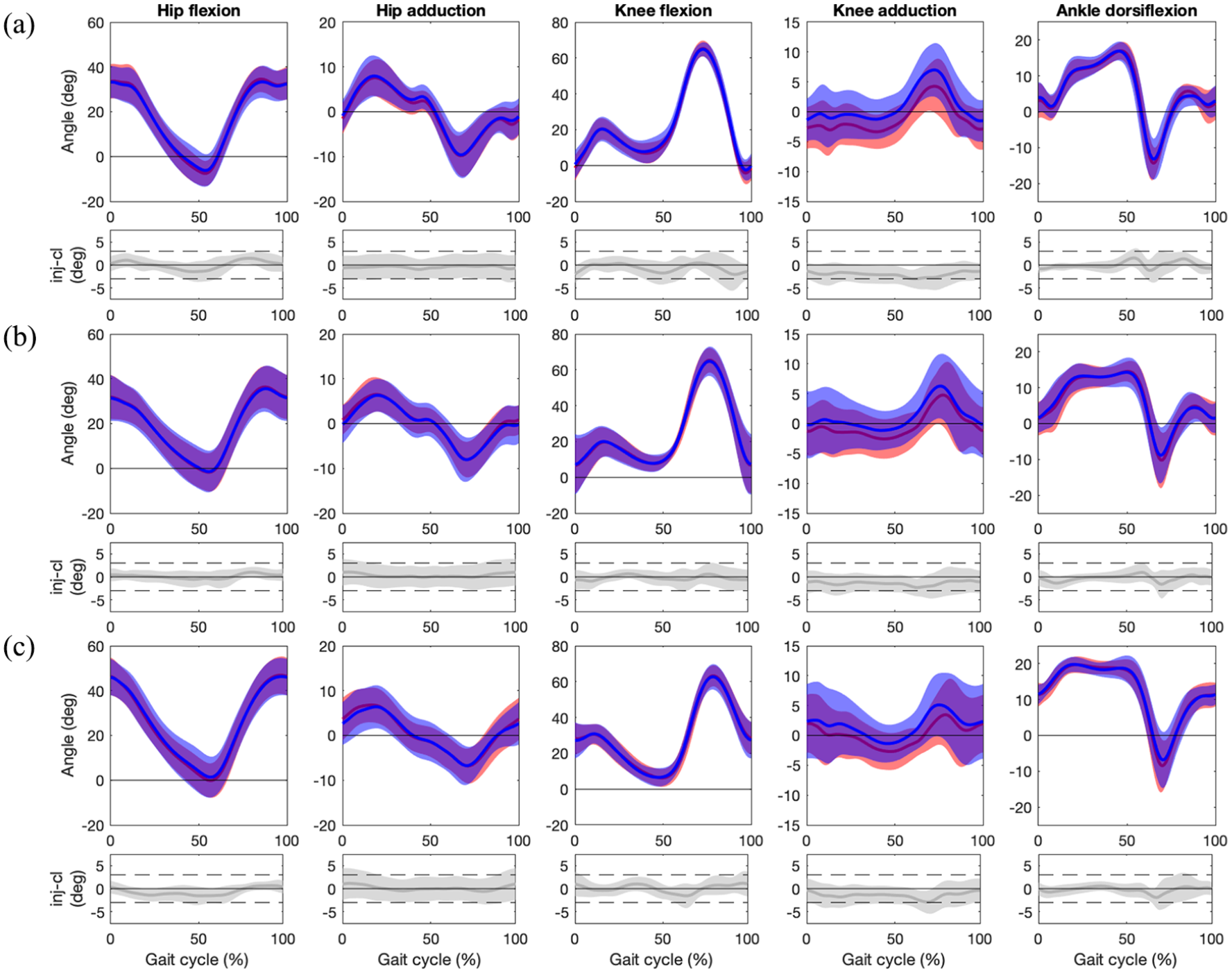
Mean (standard deviation) hip flexion, hip adduction, knee flexion, knee abduction, and ankle dorsiflexion angles for (a) overground walking (0% slope), (b) treadmill walking (0% slope), (c) treadmill walking (10% slope) for the injured (red [lighter]) and contralateral (blue [darker]) side (top graphs). Bottom graphs show mean and 95% confidence interval of the paired differences for each kinematic parameter throughout the gait cycle and the limits of the relevance interval (±3°, dashed lines).
Joint kinetics
Similarly, the joint kinetics for the injured leg were comparable to those of the contralateral leg (Figure 3). The mean paired differences in the trajectories of hip flexion and adduction, knee flexion and adduction, and ankle dorsiflexion moments between the injured and contralateral leg were largely within the relevance interval. The trajectories of knee adduction moment showed a systematic shift towards greater abduction moment (positive difference) but the mean difference remained within the relevance interval throughout the whole stance phase. The ankle dorsiflexion moment was smaller on the injured side for approximately 20% of stance in terminal stance (95% CI not containing zero), but the mean difference remained within the relevance interval.
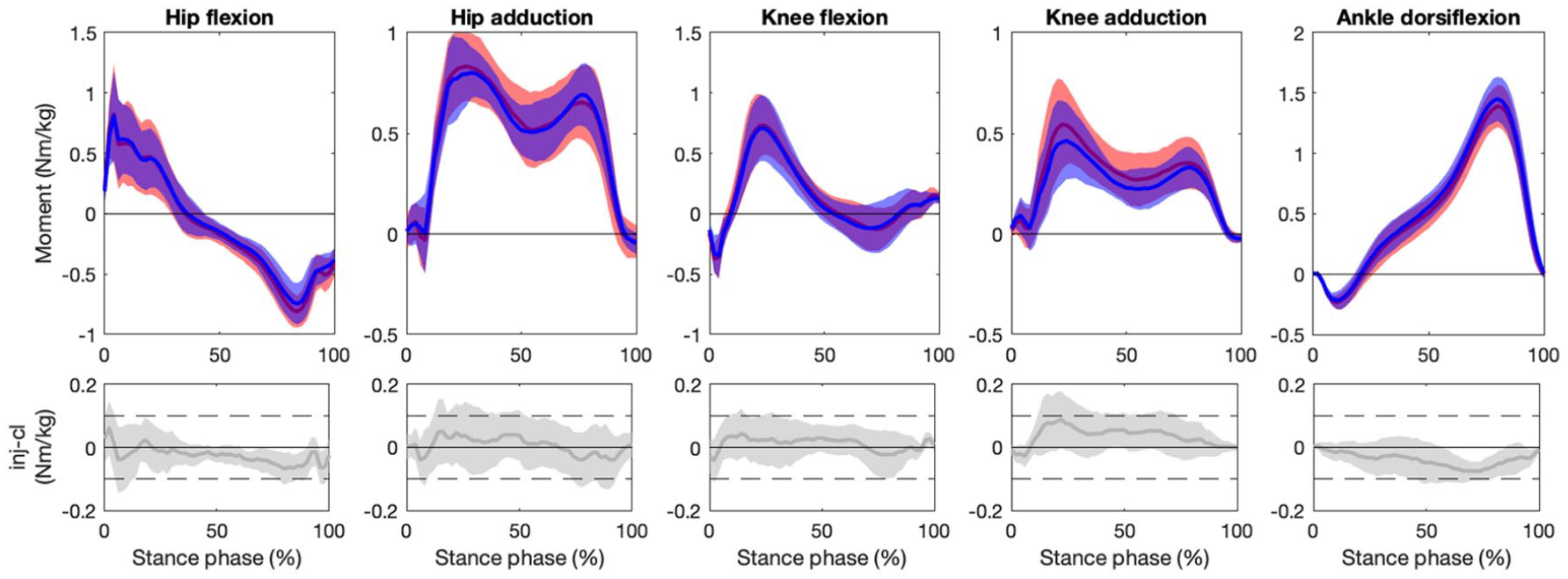
Mean (standard deviation) external hip flexion, hip adduction, knee flexion, knee abduction, and ankle dorsiflexion moments for the injured (red [lighter]) and contralateral (blue [darker]) side (top graphs). Bottom graphs show mean and 95% confidence interval of the paired differences for each kinetic parameter throughout the stance phase and the limits of the relevance interval (±0.1 Nm/kg, dashed lines).
Discussion
This study aimed to investigate the functional outcomes of activities of daily living for various walking conditions in older adults who received surgical repair of proximally ruptured hamstring tendons. Our results demonstrate that gait parameters, joint kinematics and kinetics were largely comparable between the injured and contralateral side, suggesting that reconstruction of the tendon restores joint biomechanics in gait on the injured side. This confirms and complements the previously reported good to excellent clinical results of the surgical technique used, 12 with remarkable functional results in 1 of the most common daily activities: in walking.
Specifically, we found no asymmetries in spatiotemporal gait parameters between the injured and contralateral sides in all walking conditions. Spatiotemporal parameters are most commonly used to assess functional impairment and gait symmetry in all types of populations.18,28 Most forms of walking impairments are associated with a reduction in walking speed. 29 In addition to walking speed, asymmetry describes functional differences between lower limbs and is often increased after injury.30,31 Our outcomes in gait speed, cadence and side-specific functional spatiotemporal parameters were within the normal range of healthy population reported in the literature.32,33 Studies comparing gait parameters between treadmill and overground walking reported equivocal findings.28,34 –36 Patients in our study had slightly lower self-selected walking speeds for level treadmill walking compared to overground walking, accompanied by a lower cadence, a smaller step length and a longer stance phase, which is consistent with the findings of Alton et al. 36 The differences between level and overground walking could be attributed to an uncertainty in treadmill walking in our study population, which is presumably primarily due of their lack of experience.
Kinematic measures are commonly used to assess mechanisms of injuries or to evaluate the outcome of a treatment based on gait asymmetries.2,37,38 We found comparable values for both sides, when walking on level as well as uphill. Daly et al. 38 examined the running kinematics of athletes with a history of acute hamstring injuries and conservative treatment on a treadmill with no incline. They found an increase in anterior pelvic tilt, hip flexion, and medial knee rotation on the injured side compared with the control side, resulting in statistically significant asymmetries. The combined increases in hip flexion and anterior pelvic tilt on the previously injured side may increase hamstring strain, which may be associated with an increased risk of (re)injury. 38 Therefore, it is reasonable to expect that after injury patients may benefit from surgical treatment by achieving better functional outcomes; however, this needs to be confirmed by comparison with a similar population of surgically treated patients. In addition, one must keep in mind that walking is less demanding than running, so we cannot exclude the possibility that asymmetries may occur in more dynamic tasks also in our population. However, in an older population such as ours, fast movements such as running are becoming less relevant. Overall, the joint kinematics of our patients were comparable between the injured and contralateral sides and within the normative values reported in the literature for a healthy population during both level walking and uphill walking.16,39,40
Similarly, all joint moments were within the normal range of a healthy population and comparable between sides. 16 A redistribution of mechanical power from distal to proximal has been observed in the elderly. 16 Decreased ankle joint kinetics are often associated with increased hip extensor moments during early stance and/or increased hip flexor moments during push-off. 41 Neural changes or propulsive deficits of the ankle muscles have been suggested to explain this redistribution of joint kinetics. 16 Although our patients had reduced ankle moments on the injured side during terminal stance, they had comparable hip flexion moments between the sides, which does not support this redistribution described in the literature.
Strength and limitations
We have presented the first findings on gait biomechanics after hamstring refixation in an older study population and after this specific modified surgical technique. Previous studies were largely limited to functional outcomes assessed by strength capabilities, clinical outcomes, and patient-reported outcome measures.12,13 Our estimates of clinical relevance of ±3° for kinematic trajectories and ±0.1 Nm/kg for kinetic trajectories were based on standard errors reported for kinematic and kinetic gait data and were rather conservative. The fact that differences in patterns were within these limits further support ±3° for kinematic trajectories and ±0.1 Nm/kg for kinetic trajectories to assess the comparability of kinematics and kinetics between sides.25,26 Limitations of our study are the small sample size, the heterogeneity in follow-up, and comparison of the injured limb to the contralateral side rather than to non-injured controls. We addressed the latter limitation by comparing our data with data from a similar population of healthy subjects in the same age group. However, the results of our study are to be confirmed in a larger population when compared to a control intervention.
Conclusion
Surgical refixation of the tendon appears to result in ambulatory mechanics comparable to those of the contralateral leg and within the range of normative values reported in the literature, suggesting that patients do not adopt compensatory gait patterns. Minor functional limitations should be addressed early with therapeutic interventions such as coordinative exercises and strength training to maintain or improve gait mechanics. Finally, our results complement previous findings on surgical hamstring repair with good functional outcomes in terms of ambulation and suggest that elderly active patients may benefit from surgical treatment.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was funded by the Department of Orthopaedics and Traumatology of the University Hospital Basel, Switzerland. Linda Bühl’s salary was partially funded by a research fellowship by Zimmer Biomet Deutschland GmbH. The sponsor did not have a role in any aspect of this study.