
Abstract
Background:
To improve clinical management, the International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine (ISAKOS) developed a specific subclassification of Rockwood type III acromioclavicular (AC) injuries: IIIA (no overriding distal clavicle) and IIIB (overriding distal clavicle).
Purpose/Hypothesis:
The study aimed to determine the inter- and intraobserver reliability of the radiographic classification proposed by ISAKOS for AC injuries. It was hypothesized that the strength of agreement for the ISAKOS modification will be substantial to almost perfect.
Study Design:
Cohort study (diagnosis); Level of evidence, 3.
Methods:
We evaluated 40 radiographs of all types of AC joint injuries from patients at a single institution. The images were distributed to 6 shoulder and elbow fellowship–trained orthopaedic surgeons, along with standardized assessment questionnaires. The evaluators measured the bilateral coracoclavicular distance and the coracoclavicular ratio and classified the severity of the injuries according to the modified ISAKOS Rockwood classification. Four of the surgeons repeated the evaluation 6 weeks later to calculate intraobserver agreement. The kappa (κ) statistic was calculated for categorical inter- and intraobserver reliability. Intraclass correlation coefficient (ICC) estimates were calculated for the reliability of the coracoclavicular distance measurement. A 2-tailed test was performed to assess statistical significance.
Results:
Overall interobserver agreement was substantial (κ = 0.637; 95% CI, 0.595-0.680) among the 6 evaluators, and intraobserver agreement was also substantial among the 4 evaluators (κ = 0.616; 95% CI, 0.549-0.638). The interobserver agreement for evaluating types IIIA and IIIB was fair (κ = 0.215; 95% CI, 0.135-0.295) and moderate (κ = 0.473; 95% CI, 0.393-0.553), respectively. The agreement on the coracoclavicular distance measurements was excellent among the 6 evaluators on both the affected side (ICC, 0.982; 95% CI, 0.970-0.990) and the unaffected side (ICC, 0.930; 95% CI, 0.894-0.958).
Conclusion:
Substantial agreement was found when categorizing AC joint injuries using the ISAKOS modification of the Rockwood classification, with excellent reliability demonstrated for the quantitative assessment of vertical displacement of the clavicle. Visual examination was unreliable in differentiating type IIIA injuries from type IIIB injuries.
Keywords
Acromioclavicular (AC) joint injuries are common among athletes, especially in contact sports. 6,15 Despite extensive research in the recent literature, the treatment of acute and chronic AC joint injuries remains a challenge for orthopaedic surgeons. 33 Furthermore, there is still substantial debate about recommendations for treating unstable AC joint injuries (Rockwood types III-VI), particularly for Rockwood type III. 4,19,24,43 Although several publications have recommended nonoperative management of type III injuries, 6,8,44 there are insufficient data to conclude that surgical treatment does not provide additional benefits in terms of function, return to previous activities, postoperative osteoarthritis, or quality of life compared with conservative treatment. 19,24,43
Although surgical treatment appears to be beneficial in young and active patients, 29,44 nonoperative management prevailed in cost-effectiveness for the treatment of Rockwood type III AC joint injuries. 14 Therefore, the surgical indication should ideally be based on a comprehensive, verified, reliable classification and ideally based on clinical and diagnostic imaging. 9,20 Introduced in 1984, 39 the Rockwood classification is the classification used most widely by surgeons to diagnose and assist in clinical decision-making. 13,41
Six categories are included in the Rockwood classification for grading the severity of AC joint injuries. Type I and II injuries are treated conservatively, whereas type IV to VI lesions are generally treated surgically. 4,5,7,22 However, the treatment of type III injuries based on the original Rockwood system is often challenging. 4,24,42,43 Several variables have been proposed to be the origin of this disagreement, including the lack of high-quality evidence that shows the advantages of conservative treatment over immediate or delayed surgery. 11,34 Furthermore, recent studies have associated the Rockwood classification with limited reliability. 9,20,32,35,38 As a result, it is difficult to agree on a criterion and assess homogeneous and well-defined type III injuries during investigations. 22
Beyond the highly diverse methodology used among these studies, poor-to-moderate inter- and intraobserver agreement has been reported when evaluating AC joint injuries using the Rockwood classification. 9,20,32,35,38 To improve the clinical approach, the Upper Extremity Scientific Committee of the International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine (ISAKOS) has suggested modifying Rockwood type III into IIIA (stable AC joint without an overriding clavicle on cross-body adduction view) and IIIB (overriding clavicle) to differentiate stable from unstable injuries, respectively. 5 As a result, the distinction between these lesions is based on the clinical presentation and radiographic evaluation of the cross-body adduction view. 5 Table 1 shows the Rockwood classification as modified by the ISAKOS committee. 5,39
Rockwood Classification as Modified by the Consensus of the ISAKOS Committee a

a AC, acromioclavicular; AP, anteroposterior; CC, coracoclavicular; CCD, coracoclavicular distance; ISAKOS, International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine; N/A, not applicable.
Numerous studies have adopted this new approach in their clinical practice, 3,17,18,27,30,31,34 and it has been accepted as a comprehensive classification system. 40 However, the reliability of the modified classification has not been demonstrated. Therefore, this study aimed to determine the inter- and intraobserver reliability between surgeons categorizing AC joint injuries using the Rockwood classification modified by ISAKOS. 5 We hypothesized that inter- and intraobserver agreement for the radiographic assessment between shoulder and elbow surgeons is substantial to almost perfect.
Methods
Patient Selection
The institutional review board of the Clinica Universidad de los Andes authorized this retrospective analysis. The requirement for informed consent from participants was waived. Patients with acute AC joint injury from a single hospital for 18 months (July 1, 2018, to December 31, 2020), who had undergone the radiographic protocol within 3 weeks of the original trauma and were between 18 and 40 years of age, were eligible for inclusion. Exclusion criteria included a history of os acromiale shoulder pathology, distal clavicle degenerative pathology, a radiographic method that did not meet the radiographic protocol, open physis, and fracture sequelae that had not been noted previously in the medical history. A complete set of bilateral radiographs was collected retrospectively from 46 consecutive patients with an AC joint injury.
Radiographic Protocol
At the time of the initial injury, each patient had 4 sets of bilateral radiographic projections taken: (1) a true bilateral anteroposterior (AP), (2) a bilateral panoramic Zanca, (3) a bilateral axillary, and (4) a bilateral cross-body adduction view (Alexander 1 /Basamania).
A well-defined approach was used for the bilateral cross-body adduction view. The patient stood 45° from the detector (as for the Y-view of the shoulder). The cross-adducted arm was placed in front of the chest, and the hand rested on the contralateral shoulder (Figure 1). 28 Furthermore, collimation, exposure, and central point were consistent throughout the study, maintaining a source-to-image distance of 100 cm. The radiograph settings were established according to the size of the patients from 58 kV and 8 mA to 60 kV and 10 mA, as previously reported. 23
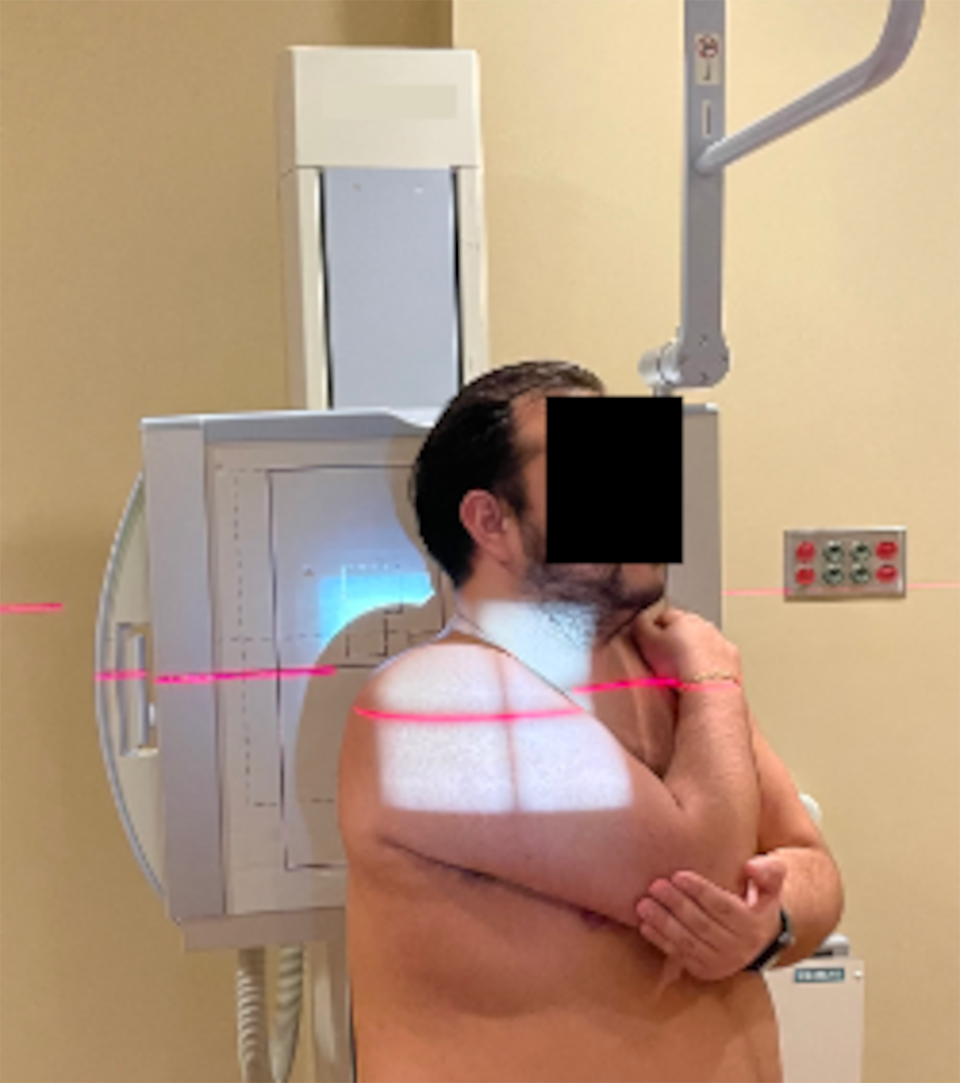
Radiographic positioning of the patient for the cross-body adduction view.
Data Collection
Six shoulder and elbow surgeons from 3 different institutions watched a short instructional video on how to (1) measure the coracoclavicular distance (CCD) in the AP view and (2) calculate the CCD ratio. Shoulder and elbows specialists were defined as fellowship-trained shoulder and elbow orthopaedic surgeons with ≥5 years' experience whose practice included surgical management of AC joint injuries. In addition, the assessors received a copy of the original publication by the ISAKOS Upper Extremity Committee 5 outlining the radiographic definition of the Rockwood subclassification to distinguish between type IIIA and IIIB (Figure 2).

Radiographic subclassification of the Rockwood system proposed by ISAKOS Upper Extremity Scientific Committee. Using the digital caliper in the panoramic AP view, we measured CCD through vertical lines (yellow arrows). The CCD ratio was calculated and expressed as a percentage. The images here consist of 2 cases. In type IIIA injury, the CCD ratio is 66%, and the cross-body view (Alexander) on the affected side shows no overriding clavicle on the acromion. In contrast, for type IIIB, the CCD ratio is 75%, and the radiographic image in the cross-body view shows an overriding clavicle on the acromion. AP, anteroposterior; CCD, coracoclavicular distance; ISAKOS, International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine.
Radiographic sets were acquired from a single institution and recorded as Digital Imaging and Communications in Medicine (DICOM) files. Before distribution, they were anonymized by removing demographic information. Furthermore, additional clinical data were hidden from observers, and a single number was assigned to identify each patient. The evaluation instructions and the research questions were distributed by email. Qualitative and quantitative data were recorded using an electronic database program (Excel Version 16; Microsoft Corporation). Subsequently, a URL link was generated and distributed to all observers to download the DICOM files. Each investigator performed the radiographic evaluation independently using the open-source Horos picture archiving and communication systems software (Version 3.3.6; https://horosproject.org).
For each set of images, the evaluators were asked to perform 3 tasks and register the result in the spreadsheet: (1) the CCD on the AP view radiograph, using vertical lines to measure the distance between the uppermost border of the coracoid process and the lower border of the clavicle on the injured and healthy sides (Figure 2); (2) the coracoclavicular (CC) ratio, which was calculated as follows: (CCD injured − CCD healthy)/CCD healthy × 100; and (3) classification of the injury according to the ISAKOS modification of the Rockwood classification system, after visual evaluation of Zanca, axillary, and cross-body stress radiographs. The second evaluation included randomly altering the number and sequence of the images collected; 6 weeks later, 4 assessors repeated the process following the same technique.
Statistical Analysis
Data were analyzed using SPSS statistical software (Version 28; IBM). The inter- and intraobserver reliability were determined by calculation of the kappa (κ) statistic based on the works of Cohen 10 and Fleiss et al. 12 Interobserver analysis was used exclusively to examine each subcategory in further detail, as it can evaluate all observations simultaneously and provides a larger view of the agreement. The κ statistic was interpreted according to the Landis and Koch 21 taxonomy, in which <0 represents no agreement, 0 to 0.2 is slight agreement, 0.21 to 0.40 is fair agreement, 0.41 to 0.60 is moderate agreement, 0.61 to 0.80 is substantial agreement, and 0.81 to 1.0 is almost perfect agreement. Statistical differences between individual κ values were considered significant when the upper and lower limits of the 95% CIs did not overlap.
In addition, for the CCD measurements, we calculated the interobserver reliability using the 2-way random mixed-effects model of the intraclass correlation coefficient (ICC), assuming a single measurement and absolute agreement (ICC [2,1]). 25 The 95% CI of the estimated ICC was also calculated on the affected and unaffected sides. ICC values were interpreted as follows: <0.5, poor; 0.5 to 0.75, moderate; >0.75 to 0.9, good; and >0.90, excellent. 25 A 2-tailed test was performed to determine significant differences (α = .05).
The notation of Walter et al 45 for sample size calculation was used to calculate the power of the study. Using n = 4 for the 4 surgeons who participated in intraobserver reliability, along with an alpha value of .05 and beta of 0.20, it was estimated that the sample size required for this study was 40.38. Radiographic images of 40 patients met the selection criteria and were chosen for the intrarater reliability analysis.
Results
Patient Characteristics and Raters
Of the 46 patients who met our study inclusion criteria, 2 were excluded due to AC joint osteoarthritis, 2 were excluded due to an incomplete set of radiographs, 1 due to distal clavicle fracture, and 1 due to os acromiale. As a result, the study cohort included images from 40 patients. There were 30 men and 10 women, with a mean ± standard deviation age of 27 ± 9 years. The mean interval between initial presentation and radiographs was 3 ± 6 days; 26 had injured their right side, while 14 had injured their left side. The 6 shoulder and elbow surgeons returned the first evaluation forms, while 4 returned the second round.
Inter- and Intraobserver Reliability of Radiographic Diagnosis
The κ value for interobserver reliability, including all Rockwood subtypes, was 0.637 (95% CI, 0.595-0.680) among the 6 assessors, indicating that agreement of diagnosis using the Rockwood classification modified by the ISAKOS committee was substantial according to the conventional Landis and Koch 21 taxonomy. The Cohen κ agreement for intraobserver reliability was also substantial (κ = 0.616; 95% CI, 0.549-0.638) (Table 2).
Inter- and Intraobserver Reliability of the Rockwood Classification Modified by the ISAKOS a

a ISAKOS, International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine.
Since each type of AC joint injury depends on calculating the CCD ratio in the AP view and the visual assessment on several radiographic projections, κ values distributed by types and subtypes reflect the agreement for these combinations. There was almost-perfect interobserver agreement when diagnosing type I injuries (κ = 0.883; 95% CI, 0.753-0.913) and substantial agreement when classifying type V injuries (κ = 0.787; 95% CI, 0.707-0.867); however, there were no significant differences. In comparison, no agreement was found for type IV injuries (κ = −0.004).
Regarding subclassification type III, the interobserver agreement was fair (κ = 0.215; 95% CI, 0.135-0.295) to moderate (κ = 0.473; 95% CI, 0.393-0.553) for types IIIA and IIIB, respectively (Table 3).
Interobserver Reliability by Type of the Rockwood Classification Modified by the ISAKOS a

a ISAKOS, International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine; N/A, not applicable.
Inter- and Intraobserver Reliability of Radiographic Measurements
The ICC for interobserver reliability of the radiographic parameter measured on the AP views (CCD) indicated excellent agreement among the 6 evaluators. However, there were significant differences in the agreement between the measurements performed on the affected side (ICC = 0.982; 95% CI, 0.970-0.990) compared with the unaffected side (ICC = 0.930; 95% CI, 0.894-0.958) (Table 4).
Interobserver Reliability for CCD Measurements a
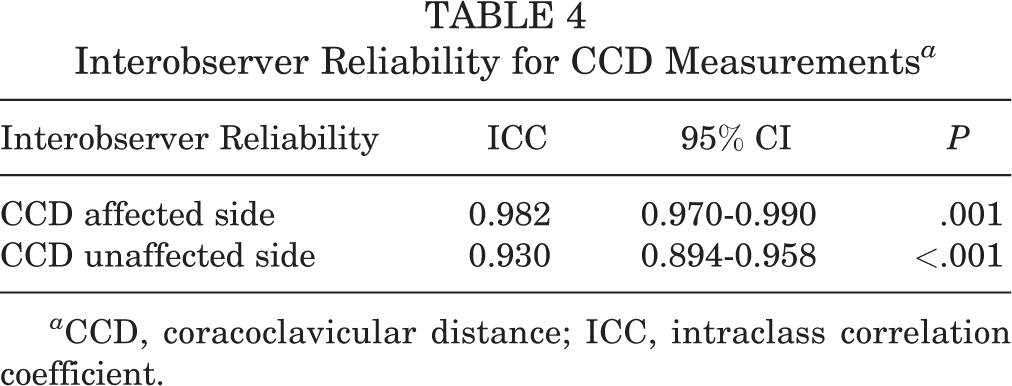
a CCD, coracoclavicular distance; ICC, intraclass correlation coefficient.
Discussion
Overall, this research indicated substantial interobserver (κ = 0.637; 95% CI, 0.595-0.680) and intraobserver (κ = 0.616; 95% CI, 0.549-0.638) reliability for categorizing AC joint injuries using the ISAKOS modification to the Rockwood classification system under a standardized radiological protocol. Although the radiographic measurements were consistent between fellowship-trained shoulder and elbow surgeons, our results indicated a lack of agreement on subclassifying type III injuries. The interobserver agreement was fair (κ = 0.215; 95% CI, 0.135-0.295) to moderate (κ = 0.473; 95% CI, 0.393-0.553) for types IIIA and IIIB, respectively.
Rockwood classification is the approach used most widely to assess AC joint injuries. 39,40 Current practice suggests that Rockwood types I and II should be handled conservatively, while types IV and V should be treated surgically; however, the management of Rockwood type III remains controversial. 2,4,6,9,19,20,24,42,43 There is insufficient evidence to establish significant differences in surgical or conservative treatment effects on functional outcomes in patients with type III AC joint injuries. 11,24,34
Several variables could influence these discrepancies. Type III injuries can result in a wide variety of lesions, ranging from stable asymptomatic lesions to unstable symptomatic lesions. 5 In acute AC joint injuries, the Rockwood types may not be correlated with clinical symptoms. 16 An optimal classification system would be reliable, reproducible, clinically relevant, a clear guide to treatment, and a good predictor of clinical prognosis. 9 Therefore, the key to optimal treatment may lie in identifying the underlying pathology. 5
However, the Rockwood classification system has been linked to a lack of reliability, and its use to classify AC joint injuries has been questioned. 9,20,32,35,38 Kraeutler et al 20 demonstrated a fair interobserver agreement (κ = 0.366) between 8 evaluators who rated a set of AP and axillary radiographs by visual assessment.
Pifer et al 35 examined the κ value between physicians of various disciplines in 25 cases. The moderate agreement in the evaluation of AC injuries (κ = 0.515) shown by orthopaedic surgeons was higher than between radiologists (κ = 0.363) or emergency medicine physicians (κ = 0.189). However, Pifer et al were unclear whether the low inter-departmental agreement reflects classification or training weaknesses.
Cho et al 9 observed poor agreement between experienced shoulder surgeons. Based on bilateral AP and axillary radiographs, inter- and intraobserver reliability of the classification was fair (κ = 0.214) and moderate (κ = 0.474), respectively. Furthermore, they found no significant improvement after adding additional 3-dimensional computed tomography scans. 9 However, it appears that a lack of consensus on radiography methodology is an essential factor in the lower agreement. 22,41 In addition, the use of unilateral AP or isolated Zanca projections has been associated with lower agreement between observers when grading AC joint injuries. 32,35
Our radiographic protocol aimed to eliminate a substantial amount of variability and increase the reliability of the classification of AC joint injury using bilateral projections as reported. 22 Lau et al 22 found substantial interobserver (κ = 0.624) and intraobserver (κ = 0.696) reliability of the Rockwood classification system based on bilateral rather than unilateral evaluation of AC joints. Similarly, the current study found substantial agreement between shoulder and elbow surgeons (κ = 0.637; 95% CI, 0.595-0.680).
Furthermore, visual assessment of the vertical plane, specifically between type III and type V injuries, has been identified as one of the leading causes of classification disagreement. 22 Our results agreed that adding a standardized technique to measure CCD significantly influences the agreement, as shown in a previous study. 22 Our overall result differs substantially from studies based on isolated visual assessment. 20,32,35 Bilateral measurement of CCD is a crucial strategy to improve the strength of agreement to classify AC joint injuries using the Rockwood system. 22,41
Schneider et al 41 proposed comparing the CCD with the contralateral side (through a CC index) and using the original system by Rockwood to assess acute AC joint injuries by evaluators with different levels of training. They found a disagreement between visual and measured diagnoses ranging from 6.9% to 27.6%. Inter- and intraobserver reliability were excellent for the digitally measured Rockwood grades (Pearson correlation coefficient, 0.85-0.93 and 0.90-0.97, respectively) 41 . In the current study, the ICC of the CCD measurements was excellent, although significantly higher on the affected side than on the unaffected side. Similar to our results, the CCD measurement was reproducible and has shown strong concordance for inter- and intraobserver reliability in previous reports. 23,36
On the other hand, a correct and reliable diagnosis of horizontal plane instability is critical to distinguish stable from unstable injuries and establish rational treatment recommendations. Unfortunately, this differentiation is difficult to make in most cases, as the diagnosis of a predominantly 3-dimensional dynamic injury is made using a static imaging modality. 4,36
The ISAKOS consensus group has described a more specific classification by adding the IIIA (stable) and IIIB (unstable) subgroups to the Rockwood type III categorization to provide adequate guidance in the management of this category of injury. 5 Although the rationale for this subclassification is primarily functional, specialized radiographic images should be used to offer objective information about horizontal translation. 5 The axillary view has been proposed to determine the horizontal static displacement. Nevertheless, the lack of agreement on the precise amount of posterior displacement necessary to be classified as type IV may be unreliable to classify injuries accurately. 9,20 Furthermore, the usefulness of the axillary projection appears to be inconsistent. 37 We found no agreement (κ = −0.004) between observers classifying Rockwood type IV injuries.
In addition, type III injuries are characterized by a 100% superior displacement of the distal clavicle, 5 and the ISAKOS consensus advises that this category be further subdivided by evaluating the dynamic horizontal instability. The lateral cross-body adduction view is used to evaluate how the clavicle overlaps the acromion due to the anteromedial translation of the scapula. 1 In this radiographic projection, the distal clavicle overrides the acromion in unstable subtype IIIB. 5 Thus, horizontal displacement may be underappreciated when relying simply on AP views.
Several recent studies have recommended using the ISAKOS subdivision for imaging evaluation throughout the decision-making process for evaluating AC joint injuries. 3,17,18,27,30,31,34 Recently, the panel members of the European Society of Sports Traumatology, Knee Surgery & Arthroscopy agreed that the Rockwood classification, modified by the ISAKOS statement, is the most appropriate and comprehensive classification to date to guide treatment choice. 40 However, to our knowledge, no study has shown the reliability of categorizing AC joint injuries using the ISAKOS proposal. This study demonstrated that, using a standardized radiographic protocol, with bilateral static projections and stress cross-body adduction views, the inter- and intraobserver reliability was substantial. These results align with those previously performed under a similar radiographic approach but using the original Rockwood classification system without including the cross-body adduction view. 22,41
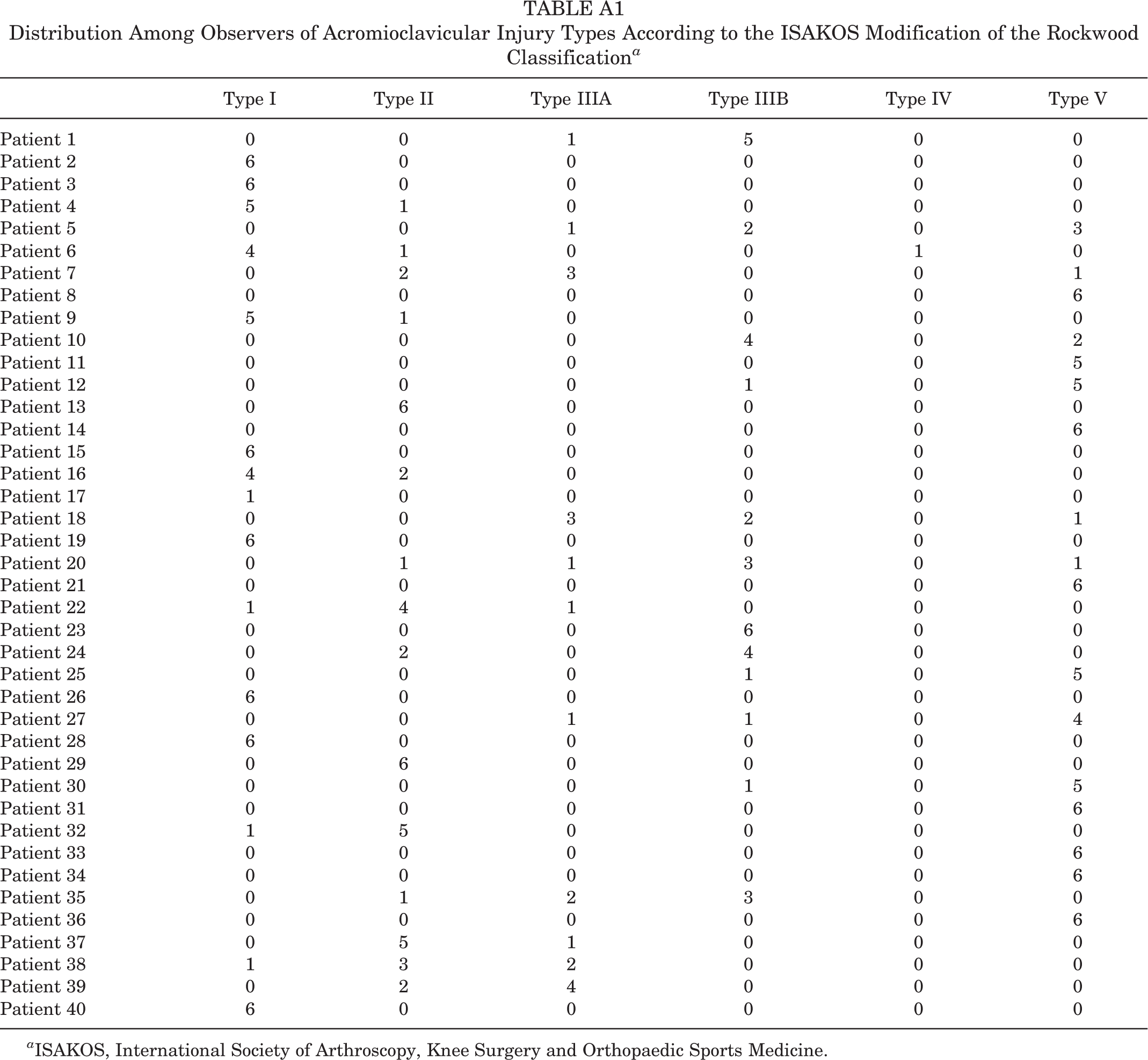
Furthermore, in this study, 16 patients were classified as type IIIA or IIIB by ≥1 surgeon, reaching unanimous agreement in just 1 patient (Appendix Table A1 and Figure A1). Since the distinction between types IIIA and IIIB is critical for decision-making and constitutes the rationale for the ISAKOS modification, the κ values in each type of injury allow us to distinguish those with better or poorer results in the interobserver analysis. Interestingly, the interobserver agreement exhibited in our study was fair and moderate for type IIIA and IIIB, respectively. This outcome can be attributed to the radiographic distinction used in type III subclassification that is based on a subjective radiographic assessment rather than an objective measurement.
Interpreting Cohen κ values ranging from 0.41 to 0.60 as moderate implies that a κ of 0.41 represents sufficient agreement. 21 McHugh 26 has proposed a more analytical interpretation, suggesting that any κ value <0.60 indicates insufficient agreement among the raters. Contrary to our hypothesis, the interobserver reliability to distinguish between type IIIA and type IIIB was limited using the ISAKOS subclassification in the context of this study. Furthermore, the strength of agreement was lower than that of the other types except for type IV (see Table 3). These findings suggest that Rockwood type III injuries will most likely require additional subclassification due to significant discrepancies and high variability in the radiographic classification method.
Other methodologies can be investigated to improve classification agreement and accuracy as a diagnostic tool. Several researchers have developed quantitative approaches to distinguish between IIIA and IIIB types objectively. 17,28,46 However, none of these quantitative evaluation methodologies has been adopted widely, and a validation procedure has not been carried out for most of them.
Limitations
The first limitation of this study was the lack of clinical data on the patients, which is critical in the decision-making process. However, we believe that clinical presentation should not influence radiographic reliability analysis alone, as the purpose of the study was to determine the consistency of radiographic classification rather than to assess validity. As a result, the impact of the lack of clinical data on imaging assessment appears negligible in this particular case. Moreover, studies that measure agreement based on a comprehensive functional approach might be more relevant. Therefore, prospective designs including associated clinical features combined with radiographic presentations are suggested for future research. Second, because this was a retrospective study conducted in a single center, the image sets were preselected, potentially adding selection bias and compromising external validity. Third, although the radiographs were obtained using a defined protocol, they were taken by several technicians, which may have increased variability.
Conclusion
The study findings indicated overall substantial agreement of shoulder and elbow surgeons when categorizing AC joint injuries using the ISAKOS modification of the Rockwood classification. Furthermore, the reliability exhibited in assessing the vertical displacement of the clavicle was excellent using a standardized protocol to measure CCD on AP radiographs. However, visual assessment of the cross-body adduction view lacks reliability in differentiating type IIIA and type IIIB when subclassifying type III injuries. More research with adequate methodology is needed to provide alternative approaches to accurately identify stable and unstable injuries that, along with thorough clinical evaluation, can help minimize the number of cases where horizontal instability of the AC joint is underestimated.
Footnotes
Final revision submitted May 14, 2022; accepted August 10, 2022.
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Ethical approval for this study was obtained from Hospital Militar de Santiago (IRB ID# CEC/120-60).
APPENDIX
Distribution Among Observers of Acromioclavicular Injury Types According to the ISAKOS Modification of the Rockwood Classification a
| Type I | Type II | Type IIIA | Type IIIB | Type IV | Type V | |
|---|---|---|---|---|---|---|
| Patient 1 | 0 | 0 | 1 | 5 | 0 | 0 |
| Patient 2 | 6 | 0 | 0 | 0 | 0 | 0 |
| Patient 3 | 6 | 0 | 0 | 0 | 0 | 0 |
| Patient 4 | 5 | 1 | 0 | 0 | 0 | 0 |
| Patient 5 | 0 | 0 | 1 | 2 | 0 | 3 |
| Patient 6 | 4 | 1 | 0 | 0 | 1 | 0 |
| Patient 7 | 0 | 2 | 3 | 0 | 0 | 1 |
| Patient 8 | 0 | 0 | 0 | 0 | 0 | 6 |
| Patient 9 | 5 | 1 | 0 | 0 | 0 | 0 |
| Patient 10 | 0 | 0 | 0 | 4 | 0 | 2 |
| Patient 11 | 0 | 0 | 0 | 0 | 0 | 5 |
| Patient 12 | 0 | 0 | 0 | 1 | 0 | 5 |
| Patient 13 | 0 | 6 | 0 | 0 | 0 | 0 |
| Patient 14 | 0 | 0 | 0 | 0 | 0 | 6 |
| Patient 15 | 6 | 0 | 0 | 0 | 0 | 0 |
| Patient 16 | 4 | 2 | 0 | 0 | 0 | 0 |
| Patient 17 | 1 | 0 | 0 | 0 | 0 | 0 |
| Patient 18 | 0 | 0 | 3 | 2 | 0 | 1 |
| Patient 19 | 6 | 0 | 0 | 0 | 0 | 0 |
| Patient 20 | 0 | 1 | 1 | 3 | 0 | 1 |
| Patient 21 | 0 | 0 | 0 | 0 | 0 | 6 |
| Patient 22 | 1 | 4 | 1 | 0 | 0 | 0 |
| Patient 23 | 0 | 0 | 0 | 6 | 0 | 0 |
| Patient 24 | 0 | 2 | 0 | 4 | 0 | 0 |
| Patient 25 | 0 | 0 | 0 | 1 | 0 | 5 |
| Patient 26 | 6 | 0 | 0 | 0 | 0 | 0 |
| Patient 27 | 0 | 0 | 1 | 1 | 0 | 4 |
| Patient 28 | 6 | 0 | 0 | 0 | 0 | 0 |
| Patient 29 | 0 | 6 | 0 | 0 | 0 | 0 |
| Patient 30 | 0 | 0 | 0 | 1 | 0 | 5 |
| Patient 31 | 0 | 0 | 0 | 0 | 0 | 6 |
| Patient 32 | 1 | 5 | 0 | 0 | 0 | 0 |
| Patient 33 | 0 | 0 | 0 | 0 | 0 | 6 |
| Patient 34 | 0 | 0 | 0 | 0 | 0 | 6 |
| Patient 35 | 0 | 1 | 2 | 3 | 0 | 0 |
| Patient 36 | 0 | 0 | 0 | 0 | 0 | 6 |
| Patient 37 | 0 | 5 | 1 | 0 | 0 | 0 |
| Patient 38 | 1 | 3 | 2 | 0 | 0 | 0 |
| Patient 39 | 0 | 2 | 4 | 0 | 0 | 0 |
| Patient 40 | 6 | 0 | 0 | 0 | 0 | 0 |
a ISAKOS, International Society of Arthroscopy, Knee Surgery and Orthopaedic Sports Medicine.