
Abstract
Purpose:
Our aim was to conduct this survey among consultant shoulder surgeons in the United Kingdom to document the current management of Rockwood type III acromioclavicular joint (ACJ) injuries.
Methods:
British Elbow and Shoulder Society Research Committee-approved online survey was used and 137 responses were collected within 3 months.
Results:
One hundred percent of responders would treat type III injuries conservatively initially. Routine physiotherapy would be offered by 86% of surgeons. The patient’s factors that influence the decision to consider surgery are pre-injury functional demand, current functional deficit, pain and patient request for surgery. Across all groups the mean time to surgical intervention from injury was 3.8 months. About 45% of all consultants would use the same technique for all cases and there were differences between the varieties of techniques used by surgeons, depending on their degree of experience. LockDown was the most widely used technique in all groups of patients. This was followed by Ligament Augmentation & Reconstruction System (LARS), hook plate and Arthroscopic TightRope/DogBone technique for acute injuries. LARS, modified Weaver–Dunn and ACJ resection were used most commonly after LockDown for delayed cases.
Conclusion:
Our survey revealed the current trends in clinical practice to treat symptomatic Rockwood type III ACJ injuries, but it also confirmed the controversial and complex management differences, which vary among shoulder surgeons in the United Kingdom.
Introduction
Acromioclavicular joint (ACJ) dislocation is a common injury seen in orthopaedic practice and accounts for up to 12% of shoulder injuries. 1 It is most commonly seen in younger male patients who participate in contact sports, and the spectrum of injury encompasses from minor sprains and subluxations to complete dislocations with rupture of the surrounding soft tissue structures. The ACJ injuries were classified by Rockwood into six separate types, according to the severity of the injury. 2 Although this is still the commonly used classification system, recent studies have suggested an overall lack of reliability of the Rockwood classification of ACJ dislocations and of decisions regarding their treatment. 3,4
Less severe (types I, II and III) ACJ injuries are more common, 2 with recent studies suggesting that of those who present to hospital, the most common are type III injuries. 5
The treatment of ACJ injuries can be broadly stratified by the severity of the injury, with type I and II injuries almost universally treated conservatively with expected return to painless full range of motion few weeks after the injury. 6 There is also consensus that type IV, V and VI injuries should be treated surgically. 7 The treatment of type III injuries is less clear, with current evidence suggesting that both conservative and surgical treatment have similar outcomes. 8,9 There is no clear consensus on the management of these injuries and no randomized controlled trials to support clinical decisions. Most of the studies in the literature support nonoperative management for most patients; however, other factors must be considered, including the patient’s occupation and physical demands as well as the age of the injury. Overhead athletes and manual labourers place high demands on their shoulders, prompting some surgeons to consider acute surgical treatment for these patients. The only advantage to operative intervention consistently borne out in the literature is an increased probability of anatomic reduction, but there is no correlation between reduction and improvement in pain, strength or motion, however. On the other hand, these patients are usually able to return to full sport with no deficits if appropriate rehabilitation is emphasized, and for those patients who fail conservative management, a multitude of surgical techniques exist to reconstruct the ACJ. This survey was therefore carried out in 2014/2015 to document the clinical practice of shoulder surgeons in the United Kingdom (UK) when treating the controversial Rockwood type III injuries and to determine what factors influence their decisions.
Materials and methods
A one-page, web-based survey was created using a survey creation tool (http://www.surveymonkey.com, supplement online link with questionnaire). Approval for the study was gained from the British Elbow and Shoulder Society (BESS) Research Committee. The survey link was sent via email to all consultant members of BESS, which was kept open for a 3-month period.
The survey questions included clinical experience (number of years as a consultant surgeon), the preferred method of differentiating between Rockwood type III and IV injuries, the preferred treatment protocol for type III injuries and the indications for surgery and the preferred procedure for symptomatic patients. The responding surgeons were invited to provide this information for different patient subgroups: overhead athlete, collision athlete, young (<35 age) male, young (<35 age) female, male or female (35–65 age) with high functional demand and elderly (>65 age) patients.
Results
Overall, the survey received a response from 137 consultant surgeons (response rate: 30%). Of these, 51% had at least 10 years of experience in shoulder surgery.
Diagnosis and initial management
It was found that 86% of surgeons made a differentiation between Rockwood type III and IV injuries based upon clinical examination. This was also confirmed by some form of radiograph imaging to assist in the diagnosis (axillary radiograph – 48%, AP radiograph – 43%, Zanca view radiograph – 13% and lateral Y view radiograph – 10%).
One hundred percentage of all responders indicated a preference to treat type III injuries conservatively initially. This was indicated to be with sling immobilization for a period of up to 4 weeks in 90% of all acute injuries, with a slightly shorter period of time for elderly patients (> 65 age). Routine physiotherapy would be offered by 86% of surgeons surveyed for injuries in the acute setting and 14% of responders would never refer their patients for physiotherapy (Table 1).
The time for physiotherapy referral after type III ACJ injury.

ACJ: acromioclavicular joint.
Surgical intervention
With regard to consideration to proceed with surgery, there were a number of factors that seemed to influence the decision-making process (Table 2). The factors that seemed to have the largest bearing were pre-injury functional demand, current functional deficit, pain and patient request for surgery. The age, gender and hand dominance of the patient had no significant bearing on whether or not surgery was offered.
The patients’ factors that influence the decision to consider surgery.

Surgeons were then asked to specify their treatment plans for different patient subgroups and no immediate surgical intervention was advocated in any group. Across all groups, the mean time to surgical intervention from injury was 3.8 months (Table 3). There was no difference in the way in which overhead or collision athletes were treated or any difference between males and females. There was a slight difference between the mean time to surgical treatment for acute injuries (i.e. <3 weeks) and delayed cases (>3 weeks) across all patient subgroups.
Decision to proceed with surgical treatment.

It was evident that consultants who had less than 10-year practice had a tendency towards earlier operative intervention compared to those who had 10 or more years of experience.
Surgical technique
Forty-five percentage of responders surveyed said that they would use a single technique for all cases of ACJ instability, regardless of whether they were acute or not. The remaining 55% stated that they would use a different technique for acute and delayed cases. LockDown ACJ Ligament (previously called the Nottingham Surgilig; LockDown Medical Ltd, Redditch, UK) was the most widely used technique in all subgroups of patients. In the acute setting, the second most popular surgical technique was Ligament Augmentation & Reconstruction System (LARS, Arc sur Tille, France), followed by Arthroscopic TightRope/DogBone device (Arthrex, Naples, Florida, USA) and clavicular hook plate (DePuy Synthes; Table 4). Techniques were similar across all subgroups of patients in the acute setting. For patients who presented with a delayed injury (>3 weeks), LARS was the second most popular technique, followed by an open Weaver–Dunn (WD) technique with modifications. This was the same across all patient groups, with the exception of patients over the age of 65 years, where an arthroscopic ACJ excision was the third most popular choice (Table 5).
Surgical techniques for acute (<3 weeks) type III ACJ injuries.
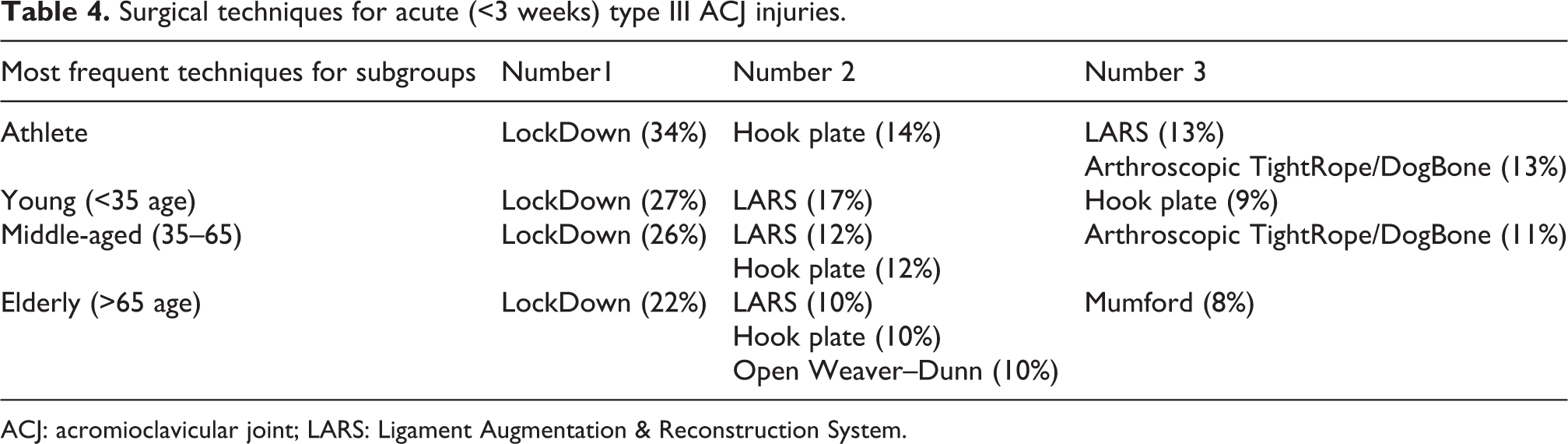
ACJ: acromioclavicular joint; LARS: Ligament Augmentation & Reconstruction System.
Surgical techniques for delayed (>3 weeks) type III ACJ injuries.

ACJ: acromioclavicular joint; LARS: Ligament Augmentation & Reconstruction System.
There were differences between the varieties of techniques used by surgeons, depending on their degree of experience. As already mentioned, consultant surgeons who had been in independent practice for less than 10 years on average opted for surgical intervention in all non-acute cases 1 month earlier than their colleagues who had practiced for 10 years or more. The surgeons with greater than 10-year experience (group A) tended to use a single technique more frequently than those with less experience (group B). There was a tendency towards newer techniques in the less experienced group, perhaps reflecting changes in training and recent developments in technology (Table 6).
Different surgical techniques by the clinical experience of the surgeons.

ACJ: acromioclavicular joint; LARS: Ligament Augmentation & Reconstruction System; PDS: polydioxanone.
Discussion
The management of Rockwood type III ACJ injuries remains controversial. There is no clear consensus as to whether these injuries should be managed conservatively or by operative intervention. 1,10 Interestingly, the ISAKOS Upper Extremity Committee has provided recently a more specific classification of this shoulder pathologies to enhance the knowledge of, and clinical approach to, these injuries. 11 They suggested the addition of type IIIA (stable ACJ without overriding of the clavicle on the cross-body adduction view and without significant scapular dysfunction) and type IIIB (unstable ACJ with therapy-resistant scapular dysfunction and an overriding clavicle on the cross-body adduction view) injuries to a modified Rockwood classification.
In an earlier survey, in the 1970s, the department heads of all approved US orthopaedic training programmes were polled. The results of this questionnaire revealed that there was a preference for surgical treatment of these injuries; however, they used the Tossy classification, which probably included injuries type IV and V of Rockwood classification. 12 Although in the 1990s, the fixation between the clavicle and coracoid became more accepted than fixation across the ACJ, another survey of Cox et al. found different results. There was a dramatic reversal in treatment choices of the surveyed US orthopaedic programme residency directors and orthopaedic surgeons, with 72% and 86%, respectively, advocating non-operative treatment for type III ACJ injuries. 13 This is a view that was supported later by McFarland et al., who surveyed all US major league baseball team orthopaedists, 69% of whom would treat throwing athletes initially conservatively but 31% would offer immediate surgery. 14 Our survey also supports the current view of the majority of clinicians that these difficult injuries can be managed conservatively, at least in the initial period.
However, a survey of Brazilian orthopaedic surgeons showed that there is no consensus in the selection between traditional and surgical treatment for 386 (80.7%) respondents, with the most important factor for selecting a given treatment method being the patient’s level of sports practice and age. 15 Another recent survey of all members of the American Orthopaedic Society for Sports Medicine (AOSSM) and approved Accreditation Council for Graduate Medical Education (ACGME) orthopedic programme residency directors showed that 81% of AOSSM members and 86% of the directors would continue to treat uncomplicated type III ACJ separations conservatively. 16
The factors that led surgeons to surgery in our survey related primarily to the patients’ premorbid function, current functional deficit and, to a lesser extent, patients’ preference. As mentioned, it is suggested that patients have a trial of conservative management for a period of 1–3 months before consideration of surgery. 1,8,10,14 Mean time to surgery for our surveyed group was 3.8 months with no difference between the timing of the injury or any patient subgroups. Functional deficit, after initial conservative management, appears to be an accepted indication for surgical intervention. 1,8,10,14 Early surgery may well be easier, especially within the ‘acute’ period (i.e. within 3 weeks), as anatomical reduction of the joint is more readily enabled. 10 However, immediate intervention without a trial of conservative management for type III injuries may well lead to unwanted complications, which may not have existed had surgery not been undertaken. 10,17 There also appears to be a paucity of evidence, based upon systematic reviews, that the outcomes from early operative intervention are superior to conservative management, in the acute period. 18,19 In type III ACJ injuries, each patient and pathology must be carefully analysed to ensure that the correct treatment option is chosen. 17 Broadly speaking there is support, from a number of studies, for the initial conservative management of these injuries. 1,8,10,14 A systematic review was carried out by Spencer favoured conservative over surgical management. 18 This is in contrast to a more recent systematic review by Korsten et al., the outcome of which suggested a possible benefit from surgery in young more active patients. 8 Our survey has shown that 100% of clinicians would choose to treat type III injuries conservatively. The recent Cochrane review also suggested that there is insufficient evidence from randomized controlled trials to determine when surgical treatment is indicated for acromioclavicular dislocation in adults, in current practice. 20
Interestingly, we found a trend for earlier surgical intervention for surgeons who had been practicing for less than 10 years. Consultants who had been independently practicing for less than 10 years (group B) offered surgery for delayed presentations (i.e. > 3 weeks) 1 month earlier, compared to those who had been practicing for greater than 10 years (group A). We hypothesize that this may reflect a more ‘aggressive’ approach by more recently appointed surgeons, compared to practice by more senior colleagues who have more experience of management and its subsequent outcomes. This difference in clinical practice also seems to be reflected in the choice of surgical technique. There were a greater variety of techniques used by consultants who had practiced for less than 10 years. This may well be as a result of recent developments in arthroscopic shoulder surgery, new advances in technology and changes to training within the UK. Other authors have already observed that younger surgeons may be more likely to adopt newer techniques without evidence of superior results. There is certainly an intrinsic attraction towards newer technologies or techniques and surgeons may perceive certain pressures to offer these. 21 On the other hand, the greater experience of surgeons could mean that they are correct to be less optimistic about the results and continue to use reliable, reproducible and well-established techniques.
There is good evidence in the literature for all the surgical techniques that were identified within the survey. 22 –29 LockDown and LARS techniques represented the first and second most popular techniques, for both acute and delayed injury groups. Helfen et al. also proved that due to inconsistent study designs, there is no evidence for a general superiority of any of the open or arthroscopic procedures. 30 Randomized controlled studies are necessary to demonstrate whether arthroscopic techniques show a potential benefit, in terms of a better functional outcome.
The limitations of this study are that it is a survey without statistical analysis, which carries a low power in terms of evidence and the conclusions we can draw from it. The response rate was low, which potentially limits generalizability, and could have been higher, to add further weight to our findings. The questionnaire was deliberately designed as a simple one-page survey in an attempt to increase response rates, but the selection bias towards those most likely to respond to this voluntary internet-based questionnaire means that respondents may not be representative of the entire population of shoulder surgeons. One of the strengths of our study was to provide an insight into the current trends in the management of type III acromioclavicular injuries in the UK. It demonstrates a consensus opinion that initial management of these injuries should be conservative and on average for a period of 3 months, before surgical intervention is offered. This is in keeping with the current evidence provided in the literature. Surgery, when offered, is tailored to the individual needs of the patient, as demonstrated by a wide variety of surgical techniques employed. The surgical techniques being used are again supported by evidence that appears to show good overall outcomes. However, the level of evidence to support a number of these techniques is inadequate for meaningful conclusions to be drawn. There is a clear need for further research into the individual techniques themselves, both in terms of the long-term outcomes and their superiority over each other. The undertaking of randomized controlled trials in the future is likely to be key in adding further clarity to the effective management of these controversial ACJ injuries.
Conclusion
Our survey revealed the current trends in clinical practice to treat symptomatic Rockwood type III ACJ injuries, but it also confirmed the controversial and complex management differences, which vary among shoulder surgeons in the UK. The reasons for this variation are understandable, in the context of our current knowledge and evidence. Further studies, with proper methodologies, are warranted for providing evidence regarding the effectiveness of surgical therapy versus conservative treatment as well as for addressing the best surgical and conservative method for treating Rockwood type III ACJ injuries.
Footnotes
Acknowledgements
The authors would like to acknowledge the support of the BESS Research Committee for the preparation of the questionnaire and the podium presentation at the Annual BESS meeting.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.